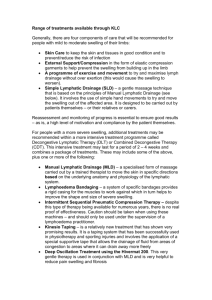
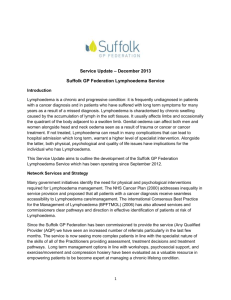
Renal Health Services Plan
advertisement

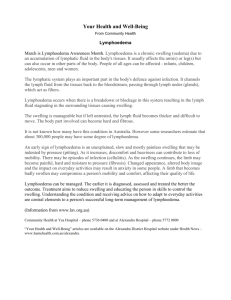
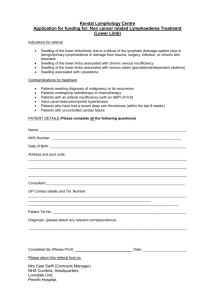
ACT Lymphoedema Services Plan 2015 - 2018 ACT Lymphoedema Services Plan 2015 – 2018 March 2015 1 ACT Lymphoedema Services Plan 2015 - 2018 Version Control: Version 1.1 1.2 1.3 Date 16/10/2014 16/11/2014 11/02/2015 1.4 18/03/2015 Modifications Initial draft for SC meeting 3 Modified following pre-consultation adjustments Incorporating Lymphoedema Steering Committee feedback Endorsed Final by ACT Health Executive Council 2 ACT Lymphoedema Services Plan 2015 - 2018 1. Overview The ACT Lymphoedema Services Plan 2015-2018 (the Plan) provides strategic direction for the provision of lymphoedema services in the ACT region to best meet current and projected population needs. The Plan outlines the future directions and service requirements to 2018 for the provision of safe and efficient services. The Plan represents the culmination of a consultation process involving a broad range of stakeholders including consumers, community representatives, peak bodies, service providers in the public and private sector, Southern NSW Local Health District, non-government organisations and researchers. The government election commitments and 2014-15 budget allocation of just over $1.85 million towards expanding lymphoedema services are implemented through increased staffing and resources. Efficiency and quality of services is achieved through education and promotion providing increased capacity for community based services and primary care involvement such as GPs and Allied Health Professionals. This Plan has been developed to provide direction to address current issues. There will not be a need to repeat this planning process after the expiration of the plan. 2. What is Lymphoedema? Lymphoedema is the accumulation of excessive amounts of protein-rich fluid resulting in the swelling of one or more regions of the body. It commonly presents in the limbs however swelling may also affect other areas, for example, the head and neck, breast or genitalia. This is due to a mechanical failure of the lymphatic system and occurs when the demand for lymphatic drainage exceeds the capacity of the lymphatic circulation. The lymphatic system is a network of vessels and nodes throughout the body that transports fluid (lymph) from the body tissues back to the bloodstream. The functions of the lymphatic system are to maintain the volume and composition of the extracellular fluid in the body and to assist the immune system in destroying bacteria and removing waste products from the tissues. Lymphoedema is often categorised by cause and hence divided into two categories: Primary - Arising due to issues with the formation of lymphatic vessels or nodes through the body’s development process; or Secondary - Secondary lymphoedema is the most common type of the condition, developing following damage to the lymphatic system. The damage may occur as a result of some cancers and their treatment or due to conditions such as, but not limited to; Obesity, tissue trauma, immobility or infection such as lymphatic filariasis. Lymphatic filariasis is a mosquito born, tropical, parasitic infection uncommon in Australia. The disease tends to occur in migrants from endemic countries. Multiple mosquito bites are needed to develop the condition so it tends not to occur in tourists to those areas. Lymphoedema may produce significant physical and psychological morbidity and the associated increased limb size can interfere with mobility and affect body image. Pain and discomfort are frequent symptoms, and increased susceptibility to acute skin infection can result in frequent hospitalisation and long term dependency on 3 ACT Lymphoedema Services Plan 2015 - 2018 antibiotics. Lymphoedema is a chronic condition which, at this time, does not have a cure. With appropriate management symptoms can be reduced, however if ignored, the symptoms can progress and become difficult to manage. 3. Current Context The demand for lymphoedema services in the future is expected to increase due to population growth and increases in the incidence of cancer and prevalence of obesity. The incidence of Cancer in the ACT region is increasing at a rate of around 4% per annum1 and the percentage of the adult population that is overweight or obese is expected to increase to 66% by 20192. Surgical and radiotherapy treatments for cancers that affect the lymph nodes are considered a risk factor for developing lymphoedema and these risks are increased with increased body mass. ACT hospital admissions for cellulitis have been increasing at an average rate of 6.4% per annum for the last three years and are expected to continue to increase. Cellulitis is both a risk of and a risk for chronic oedema/lymphoedema and thus would benefit from lymphoedema related assessment and management. The overall prevalence of lymphoedema/chronic oedema has been estimated in the literature at 0.13-2% of the population. This estimation equates to 802 - 12,341 people when extrapolating from the total catchment population (617,071 at June 2012)3 of the ACT region. Currently, public lymphoedema services are primarily provided at Calvary Hospital with a smaller services provided at Clare Holland House and Canberra Hospital as well as in some regional centres. Private sector services are also provided in Canberra and the surrounding region. These services provide screening, assessment, advice, education and clinical management of lymphoedema. Complex cases are often referred to Calvary Hospital where a medical lead multidisciplinary clinic is run. Gaps are evident in current services which have been operating with waiting lists of up to 7 months, over 3 times the benchmark response time for low risk patients. There is limited capacity for service provision to inpatients and knowledge of lymphoedema in the workforce more broadly could be improved. The complex management of lymphoedema requires specialised experience and training and, as a result, the services available to people with lymphoedema are reliant on maintaining staff with appropriate expertise. The current disbursement of staff means that supervision and succession planning are difficult to ensure. Increased education and promotion of lymphoedema within the primary care and private sectors may increase capacity and provide more options for patients which in turn may reduce pressures on specialist services. 4. Goals and directions for lymphoedema services Strategic directions for lymphoedema services have been developed to meet increasing service pressures for the current planning horizon. Increased articulation 1 Australian Institute of Health and Welfare: Radiation oncology areas of need, cancer incidence projections 2014-2024. http://www.aihw.gov.au/ 2 OECD- obesity epidemic: analysis of past an projected future trends in selected OECD countries. http://www.oecd.org 3 ACT Health – ACT Chief Health Officer’s Report 2014. http://www.health.act.gov.au 4 ACT Lymphoedema Services Plan 2015 - 2018 with private sector services within the ACT and surrounding region will be promoted throughout the life of the plan. During the planning process the following principles for service development were identified to guide the development of the Lymphoedema Services Plan. Services will be: Patient centred. Multidisciplinary and collaborative. Accessible and Equitable. Safe and high quality; have a Population health approach; and include focus on Research and Education Lymphoedema services will focus on the following objectives: Objective 1 – Primary prevention: That Lymphoedema Services contribute to a planned strategy of integrated chronic disease primary prevention program focusing on nutrition and physical activity. Objective 2 Early detection and secondary prevention: To provide an optimal integrated service in lymphoedema detection and management. Objective 3 Lymphoedema services: Establish a sustainable multidisciplinary service to meet needs of lymphoedema patients, which is safe and high quality in an environment with a community health focus. Objective 4 Research and education: There will be a strong research component across all lymphoedema services within the ACT supporting and informing the delivery of clinical services. Objective 5 – Access and equity: There will be a greater focus on improving access and equity across all lymphoedema services within the ACT and surrounding regions 5. Framework for Lymphoedema Services ACT Health has identified a need to shift the focus of services from the hospital to the community environment and to increase the capacity of private practice and primary care to be involved in lymphoedema service provision. This will help to improve access by providing services closer to where people live and also to make the most efficient use of health resources. It is expected that an expanded and holistic lymphoedema service would reduce the lymphoedema related admissions, however, this does not preclude the provision of services to inpatients. This shift will be balanced by improved capacity for inpatients to access services. Lymphoedema Services will be provided using a Hub and Spoke Model whereby complex lymphoedema management is performed in the Hub and non-complex management will occur in community locations such as Community Health Centres. This framework (represented in Figure 1) aims to reduce current duplication of processes and increase efficiency by providing one ‘Hub’ where lymphoedema clinicians have access to support, training and education by creating a critical mass of staff to enable this. Training, support and outreach services to community centres, 5 ACT Lymphoedema Services Plan 2015 - 2018 inpatient services, surrounding regions, General Practice (GPs) and other Allied Health Professionals (AHPs) can be best provided through one centre which can develop models of care and perform research into best practice concepts. A Lymphoedema Services Network will be established. This Network will work collaboratively to continue to break down barriers between services, develop referral pathways and information sharing avenues including the collaborative development of pamphlets and handouts. The Network will help to resolve service wide issues and connect with the public and private sectors and community organisations both locally and in NSW. This work should integrate with HealthPathways to help share information and referral pathways with GPs. Actions and activities performed by the Lymphoedema Services Network will be undertaken with the goal of improving patient centred care and patient outcomes. 6. Resources The growth funding anounced by the government in the 2014/15 budget will enable the implementation of the Hub and Spoke model and reduce gaps in services through additional staff. The adidional staff will include the provision of a senior clinician/management position who will also perform an clinical educator role. There will be additional clinical staff and the addition of an administration staff member will enable clinicians to spend more time providing clinical services. The administration staff member will provide services to improve patient flow and facilitate comprehensive data collection and management to enable continued assessment and improvement of services. The implementation of the model will also involve acquisition of equipment and consumables for screening and treatment services. Consumables such as bandaging and electrodes for BIS screening will be provided consisitenly across publicly provided services in line with ACT Health policy. The governance structures will change to enable support for staff delivering services in the community and the inpatient setting. 6 ACT Lymphoedema Services Plan 2015 - 2018 Figure 1 – Lymphoedema framework 7 7. Patient Pathway The patient pathway has been illustrated below in Figure 2. This pathway reflects the three tiered approach illustrated in Figure 1. Inclusion of the lymphoedema stages has been attempted to try to reflect where each stage of lymphoedema fits into the model. Tier one, including GPs, AHPs and treating medical specalists will identify patients who are at risk of developing lymphoedema (Stage 0 lymphoedema). At this tier, secondary prevention initiatives should be put in place, including education and advice regarding pro-active ways to reduce the risk of developing lymphoedema. A referral should be made to services (tier two) which have access to screening technology such as BIS. The designated community health centres will be equipped with this technology to enable screening of patients at risk. Regional services and private practice may also provide screening services. Education and support to clinicians in these locations will be provided by a clinical educator and patient services will be provided by mobile lymphoedema specialist staff from the lymphoedema hub. In addition to screening, patients will be provided with further education. Screening and secondary prevention should include a multidisciplinary approach to care. Group education sessions will be run from the community centres. Patients who have or go on to develop lymphoedema (Stage I and II lymphoedema) should be referred to be treated in the community centres, private practice or at regional services. If the lymphoedema condition is deteriorating, becomes complex (Stage III lymphoedema) or complicated by comorbidities, the patient will be referred on to the lymphoedema hub (tier three), currently at Calvary Hospital. Patients will receive further education, and complex management of their condition. A multidisciplinary clinic will be run from this location with a medical specialist for the menagement of difficult complex cases. Patients will be referred back to tier two services for regular maintainance once the complexity of their condition has reduced. For patients who do not require input from the medical/mulstidisciplinary clinic, there is some capacity for complex lymphoedema care in the private sector. The outpatient lymphoedema services at Canberra Hospital will cease and will transition to community location/s. Inpatient lymphoedema related services at Canberra and Calvary Hospitals will be provided by clinicians based at or near those locations. Education of other staff at the hospitals will be managed by lymphoedema staff from the Hub or Canberra Hospital with the support of the lead clinician at the Hub. 8 Figure 2 – patient pathway Tier one Tier two Tier three *Note: Private practice has some capacity to manage complex cases **Inpatients may be managed and referred into this pathway if appropriate 9