Altitude Chamber

Altitude Chamber (Hypobaric) Training
Photo: Edwards AFB Altitude Chamber
Author: Kevin Svetcos
Foreword:
This article documents the "Altitude Chamber" flights as they were performed at Beale AFB in California. As a
Physiological Support Division (PSD) instructor, Kevin Svetcos is uniquely qualified to describe the hypoxic dangers of high altitude flight and those effects on the human body. Also included is an article by Terry
Pappas, a pilot who became hypoxic in an SR-71.
Leland Haynes, Webmaster, SR-71 Blackbirds
From Kitty Hawk to 80,000 Feet:
While flying remains one of the safest and most effective modes of transportat ion in the world today, there are definite inherent risks associated with anything that travels through the air at speeds sometimes greater than sound and at heights greater than the distance some of us drive to work. No one is more aware of those risks than those who crew the airplanes and receive extensive training before even climbing onboard an aircraft for the first time. It is this training that they will be required to repeat through out their flying careers. This article will review some of the classroom and chamber training requirements for aircrews to maintain their flying status. Also included is some of the specialized training that the high-fliers (SR-71 and U-2) were required to accomplish prior to flying the Blackbirds.
Ground School:
The first part of the training given to aircrews is classroom training in which they were educated in the basic principles of physics governing altitude. They learned about the barometric pressure changes and its affect on trapped gases, dry gases, wet gases, the change in temperature associated with these barometric changes as well as how the physical composition of ambient (regular) air is affected by pressure changes.
After receiving this overview, the physiological effects of flight were integrated and reviewed, and connections identified between the basic principles of physics and their unavoidable affects on the human body. While every portion of this training could literally determine the survival or loss of aircrews and their aircraft in times of a physiological event, this initial phase of the training was paramount because it was the cornerstone upon which the remainder of the training was based. It remained constant regardless of the numerous types of aircraft that would be flown during the course of one’s career.
After students were taught what could happen to them as a result of exposure to atmospheric changes in a more traditional classroom environment, they progressed to a more hands-on, interactive phase that taught prevention, recognition and recovery.
The first part of this training was prevention. It was here that the students learned about their life support systems and equipment. They received a basic overview of how an aircraft’s oxygen system worked, what a basic oxygen systems panel looked like and how to operate it, the function of oxygen masks, flying helmets and how to properly use them. They also learned about cabin pressurization, the role it played and how vitally important it was.
The next part of the training was recognition, and it was during this time that things like night vision, autokinesis and the coreolis affect were taught. The main purpose of this training was to show students how unreliable and potentially deadly their physiological instincts were in flight. During night vision training, students were taught how long it took for their eyes to adapt to dark, how quickly they could lose their night vision, and some methods to maintain it. Autokinesis and the Coreolis Effect were covered to impress upon the fliers the biggest lesson: trust the airplane’s instruments
The last part of this section, recovery, involved some aspects of recognition. It was stressed that while everyone has different levels of tolerance and different reaction times involving the effects of altitude on the human body, it is only a matter of time before everyone succumbs. Very generic timelines were laid out with the caveat that everyone is different and that they all should pay close attention to their own reactions during the ensuing altitude chamber flight. Students were taught the symptoms of oxygen deprivation and the normal physiological changes that they could expect at altitude. To combat the symptoms of oxygen deprivation, they were taught how to connect their masks to their helmets and properly operate their oxygen panels. For their physiological changes, they were taught how to equalize the pressure in their ears and were encouraged to loosen their clothing to accommodate the swelling of the abdominal cavity that accompanies an increase in altitude. Needless to say, the instruction regarding flatulence was always the one that received the largest response. The altitude chamber was definitely not the best place for the meek or reserved.
The Chamber:
The next phase of training involved the altitude chamber itself. Students were taken to the chamber and assigned seats. All doors were left open during this dry run of the chamber flight as some students were understandably apprehensive. After being assigned their seats, a quick overview of the flight was
given and the students were told what to expect at what time or what simulated flight level, and the safety procedures covered. At that time the students also practiced connecting, disconnecting and checking their survival gear several times to ensure that they were doing it properly and that they were comfortable with it when the time came to do it for real.
Preparation:
Preparation for a chamber flight was very involved. Vacuum pumps that were to remove air from the chamber to create a low atmospheric pressure to simulate various altitudes had to be inspected and turned on. Oxygen banks required to get the 100% pure oxygen to the chamber for students and inside observers were checked and activated; emergency oxygen bottles and masks inside the chamber were checked and the staff required to “fly” the chamber assembled. For United States Air Force chambers, the usual crew consisted of 9 people. The crew chief was responsible for all mechanical functions of the chamber before, during and after the flight.
The main chamber was designed to hold up to 16 students and two inside observers. The main chamber operator “drove” the main chamber and controlled the interior pressure from start to finish with two different levers. The secondary chamber operator did the same thing for the "lock" or secondary portion of the chamber, which was the back end and was designed to accommodate up to four students and one inside observer. The lock had several applications. It could be sealed off and operated independently from the main chamber to facilitate the extraction or insertion of personnel. If there was an emergency involving anyone in the main chamber, the person affected was stabilized, transferred to the lock and an inside observer accompanied them back to ground level where the appropriate assistance would be rendered. Conversely, if someone from the outside needed to join the students at altitude, the two chambers could be separated and the lock equalized to the ground pressure. The new addition would get in and then be taken to meet the rest of the group. The lock was not only the equivalent of a barometric elevator, but it was also used for the rapid decompression portion of training which will be covered later on in this article. It should be pointed out at this point that the entire chamber could be operated from either the primary or secondary chamber operator’s positions.
The recorder, or timekeeper, recorded all times for the flight. The time the inside occupants started their 100% pre-breathe, when specific flight levels were achieved, how long and at what flight level the primary and secondary chambers were at. If there were any instances either inside or out of the chamber that could have a potential impact on the flight a detailed account of the situation or activity, who was involved, actions taken, minutes into the flight and durations was included. There were two inside observers on all flights for safety. Their primary job was to ensure that all students were safe and watched after at all times, and in case there was ever an extreme situation where a student had to be removed during a flight, one of the instructors could seal themselves off with the student and be brought back to ground level where other members of the crew could render any assistance needed.
Another person in attendance to monitor and advise was the Physiological Training Officer (PTO) on duty. This was one of the officers assigned to the chamber unit and trained specifically in the operation of the chamber and the effects of flight. The PTO was physically present from the time the chamber left the ground until training was over and all occupants had safely exited the chamber. Another member of the training crew was the Flight Doctor. The flight doc was a physician specially trained to deal with pilots and aircrews in order to address the unique physiological situations that could result from exposure to either a decrease or an increase in barometric pressure. This would include diving as well as flying. Chamber flights were never started until the PTO was in the chamber room and ready
to go, and they requested permission from flight doc to begin the flight. During this time, if the flight doctor was not physically present, they were at standby at the hospital and were able to be immediately contacted should an incident arise. At Beale AFB, the flight doctor was never more than 5 minutes away
Last but not least was the instructor, or “outside observer”. While the PTO had the overall responsibility, the outside observer was primarily responsible for the actual flight itself. They maintained contact with all the other members of the crew to ensure the chamber was running smoothly, all occupants were safe, the proper times were met and that all training objectives were covered. They were the ones who conducted the training from the outside and reiterated major points that were taught in the classroom. The outside observers were the main point of contact between the crew, the PTO and the flight doctor.
While most people in the unit were qualified to physically operate all areas of the outside chamber positions and function as inside observer, not everyone was qualified as an instructor. Instructors were trained in all aspects of the overall training, but could teach classes only after demonstrating their knowledge and proficiency in any specific subject. Due to the nature of the training, however, we tried to keep one instructor with the same group of students for the sake of familiarity. The instructor assigned to be the outside observer for a flight was always the one to do the primary chamber training in class and dry run prior to the actual flight.
During class time, not only did the instructors teach the course material, but we also worked very hard to learn as much about our students as possible in so far as personality traits, physical mannerisms, sense of humor (or lack thereof), etc. We did this because during a flight when students would be required to expose themselves to the harsh environment, we needed to be able to spot changes in their behavior and reaction times as soon as possible so we knew how far we could let them go before stepping in if need be. The whole purpose of chamber training was to let them experience the physiological effects and teach them how to cope with high altitude flight. The purpose of the instructors was to teach them how to do that, and then do it for them if they could not.
The Flight:
When the time came for the actual chamber flight, the outside chamber crew was already in place and ready for show time when the students entered the chamber. At that time they donned their helmets and masks, hooked up and checked the communications and oxygen systems, and started the mandated 30 minutes of pre-breathing 100% oxygen prior to exposure to the decreased atmospheric pressure. The inside observers did a physical check on every one’s oxygen connections and panels to ensure proper hookup and function. The outside observer would then do an intercom check with everyone in the chamber, one at a time to ensure that everyone could hear and be heard, starting with the students and ending with the inside observers. They would then switch to a secondary channel that was reserved only for the outside crew running the chamber, again verifying proper communications.
After this was completed, the timekeeper would be instructed to start time for oxygen pre-breathe in preparation for the high altitude exposure.
It was during this time that some of the information covered in the classroom and during the dry run was gone over again. Questions were answered and sometimes conversation not related to the flight was pursued in order to pass time and relieve some of the anxiety of those inside the chamber. At the end of 30 minutes a final check was made with everyone, the outside door was closed, and the chamber flight was under way. Normal rate of ascent was 5,000 feet per minute, during which the instructor
would remind the students what physiological effects they would be experiencing as they passed through that specific altitude. As an instructional aid, two rubber gloves - one empty and one with a little water
- were hung from the middle of the chamber ceiling to demonstrate the effect of altitude on trapped gasses much like in the students' sinuses, ears and stomach. As the chamber went higher, the gloves grew bigger.
The one with the water grew faster because wet gasses expand faster than dry gasses.
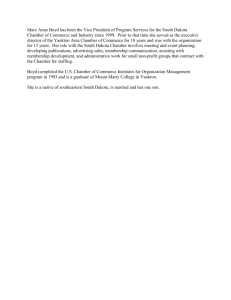
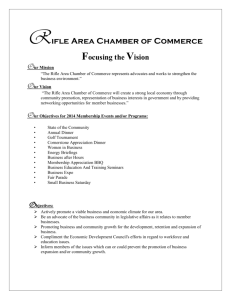
There were two different flight profiles for chamber flights. The
Type I chamber flight was to a maximum altitude of 35,000 ft, with hypoxia demonstrations at 35,000 ft
(1 person), 30,000 ft (1 person) and
25,000 ft (all remaining persons).
The Type II chamber flight was to 43,000 ft with the hypoxia demonstration at 25,000 ft only.
Although the chart on the left reflects only the 25,000 ft hypoxia demo altitude, actual USAF chamber flights progressed to 43,000 feet.
When the chamber reached 25,000 feet simulated altitude, students that did not volunteer for the demonstrations at either 30,000 or 35,000 ft. were divided into two groups. When everyone one was ready, one group at a time would drop their masks and shut off their oxygen panels so that they could experience hypoxia, or oxygen deprivation. If the reader recalls from the first part of this article, everyone reacts differently to different physiological situations. It was important for the students to experience hypoxia in order that they could recognize their own individual signs, how long it took them to experience it after exposure and their reaction time for recovery actions. They would go through the various stages, hold out as long as they felt comfortable and then recover by themselves by hooking up and restarting their oxygen systems. While one half of the students had their masks off exploring their personal boundaries, the other half of the chamber sat and watched, equally involved in the lesson. It was during this time that those watching learned how to look for signs of hypoxia in
their fellow crewmembers. This passive lesson was equally important for them to learn for their safety later on, and they were lessons better learned in a vacuum chamber sitting firmly on the ground than in an airplane 25,000 feet or more above it.
For the demonstrations at 30,000 and 35,000 feet, the volunteers were taken one at a time and put through some simple exercises. When the instructor and inside observers were ready, the volunteers would drop their masks, and the outside observer would ask simple things like name, day of the week, maybe give them a puzzle to work on. This was done to demonstrate how quickly hypoxia could come over someone, how unnoticeable (insidious) it could be, and how easily distracted one can become when concentrating on simple tasks like checking gauges, reading checklists or maps, etc. The volunteers were told to hook up their oxygen when they felt they needed it, but they usually had to be told to hook up by the instructor and it was common for the inside observer to step in and assist the student. Sometimes it was to help the student find where the mask fastened to the helmet, and other times the student was completely incapacitated and the inside observer had to hook up the mask and adjust the oxygen panel to force a high amount of oxygen into the system to revive the student. That is what we called an “attention getter” and really drove home the danger these people faced and how important this training was. It was at this point that the difference in the time of onset and severity was highlighted between the class exercise and individual examples at the different altitudes. It was common during the higher altitude demonstrations for students to go a little further than what they should have and needed a little help from the inside observers. While not exactly what we as instructors wanted to see, it served as a great learning tool for the student who over-extended their personal threshold and to the rest of the students in the chamber as well. Where before they had heard that this wasn’t a game, now they saw first hand that it wasn’t.
Characteristics of Hypoxia
On the following day a second chamber flight occurred to a maximum pressure equivalent to
43,000 ft. This was done purely to demonstrate positive pressure breathing and the physical discomfort that accompanies this altitude. No masks were taken off or exercises performed at this altitude; merely an exercise in recognition. After about one minute at this altitude, the chamber began its 5,000 fpm descent back to the ground. Students were again reminded how to relieve the pressures in their ears and other areas as they descended and the negative consequences their bodies would suffer if they did not. During descent, the main chamber operator would do their best to vent the chamber of the “stale” air within, which was more of a humanitarian gesture than anything else. Because the pressure change is not considered hazardous between sea level and 10,000 feet, supplemental oxygen is not required so those inside were allowed to drop their masks as the chamber passed through 10,000 on its way back to ground level. Early in my career as an inside observer, I found that my personal comfort level was greatly enhanced when I stayed on oxygen until the outside door opened and I could unhook and walk right out.
Rapid Decompression:
The next phase of chamber training was the rapid decompression. The first part of training was intended to teach students the effect of hypoxia and to demonstrate what it would be like if the aircraft experienced a slow loss of pressure. Rapid decompression was to simulate an immediate loss of pressure from extreme instances like a bird strike to the canopy or a large hole in the side of the airplane.
As mentioned before, there were two different sections of the altitude chamber: the main chamber and the secondary chamber, or "lock". These two chambers could work independently from each other, and there was a valve that was used to separate the two in order to run at different pressures concurrently. For the rapid decompression training, the main chamber was sealed off and taken to a simulated altitude of about 40,000 feet. While this was happening, the inside observer and 4 students would go into the lock; hookup; do their checks, then begin their ascent to 8,000 feet. For this portion of the training the students did not have their masks on their face, but instead they were left dangling from their helmets with the oxygen off.
During ascent, the inside observer would go through and explain what happens during a rapid decompression (RD). These included, but were not limited to: a loud “bang”, a noticeable drop in temperature, immediate fogging of the air, and moderate to severe air movement that could move entire books should the decompression be strong enough. When the lock reached its altitude of 8,000 feet, the crew chief would open the valve separating the two different sections and the lock operator would prepare to push the button that would cause the RD. They would notify the inside observer that the chamber and outside crew were ready and the inside observer would then give the signal and the
RD would occur.
The signal always came during the brief and was, “A rapid decompression could occur at any time…”At this point, the lock operator would push a button that would open another valve and hold it for 3-5 seconds before releasing. A thunderous
“BANG!” announced that an RD had occurred as the two chambers equalized pressure at about 22,000 ft. within seconds.
The air in the secondary chamber fogged up, there was a big wind; it got colder and some checklists and paperwork in the chamber rustled around. The students jumped like they got poked with a needle. They quickly recovered from the surprise and got their masks on and working before the descent back to ground level. The experience of a rapid decompression was so extreme that even those who knew it was coming and what to expect jumped when it happened. When it was all over, the outside crew shut down the chamber and finished their paperwork, and the students went back to the classroom to finish off their training. After receiving the initial training, anyone that was on flying status was required to undergo refresher training every three years, instructors included.
While most people only saw the inside of a chamber once every three years, it was not uncommon for an aircrew member to require a short flight in between their training. Everyone on flying status had special medical considerations and was therefore required to go to the flight surgeon’s office instead of the regular medical staff. Period. Even for things a seemingly minor as a runny nose or sore throat.
Whenever someone got sick or injured, they were almost automatically DNIFed (“de-niffed”, or Duty
Not Involving Flight) and not returned to flying status until the flight doc said so. This also happened during some dental procedures because of the potential of trapped air in a tooth that could expand if exposed to altitude. This condition was called “barodontalgia.”. No matter what type of treatment someone on flying status received, the flight doc was kept in the loop and had a direct say in it. Not all, but some medical conditions required a chamber flight to ensure that the aircrew member was physically ready to face barometric changes after their treatment before they were returned to full flying status. These flights were usually informal with one inside observer and the flier. The rate of ascent was between 2’000 to 3’000 fpm and usually to about 25’000 feet. The flight doc was always in attendance during these flights and on occasion where even in the chamber themselves.
High Fliers
While the crewmembers of the SR-71 and U-2/TR-1 required chamber training as well, their training was significantly different. The primary objective of initial chamber training was to expose students to simulated altitude so that they would learn about their own physical limitations and the dangers of operating in that environment, but the purpose of the high flier’s training was to familiarize them with their suits and demonstrate the dangers of the altitude at which they routinely flew. From the flier’s and PSD’s initial standpoint, preparation for the chamber flight was the exact same as for an actual airplane launch with the pre-flight of the suit, seat kit and parachute the day before.
While there was a separate chamber specifically designed and built to accommodate the requirements for this training, preparation and manning was basically the same as for the regular chamber, which was a major part of this special chamber flight. Except for the
PTO now conducting the training from the outside observer's position, the outside crew remained the same and now the crew chief had to ensure that the main air valve that allowed pressure equalization between the two chambers was secured shut, then run the main chamber up to altitude in order to prepare for the rapid decompression portion of the chamber flight. The smaller chamber had two separate sections, just like the larger chamber. The main portion of the chamber was about 8'X 8' square and had a mock-up of an ejection seat in it that the aviator was hooked into just as if they were in the aircraft. The second section of the chamber was a little bit shorter, and this is where the two inside observers stayed during the chamber
flight. ( Photo: Colonel Phil Loignon, SR-71 RSO at Beale AFB, Ca)
Pre-Flight Preparation and Briefing:
Preparation for the chamber flight was the exact same as for a regular flight, where the suit was preflighted the day before and set aside. The flier came in and got suited up and tested, then began the 30minute pre-breathe before being moved to the chamber. Some people may wonder why crews still had to do the pre-breathe if they weren’t going to fly. Remember that the danger was not the altitude, but the lack of atmospheric pressure at altitude, and this is what the hypobaric chambers simulated.
Physically, their feet never left the ground, but physiologically they would be traveling up to over
60,000 ft. in altitude.
The PSD technicians who suited up the aircrew member (ACM) would notify the inside observers what time their guy went on oxygen so that the observers could go on as well. The recorder took down what time everyone went on O
2
, then started the clock counting 30 minutes at the latest time. When it came time, the techs who suited up the ACM hooked them up to the portable oxygen cooler, transferred them to the chamber and did the hook up into the seat as the inside observers looked on.
When everyone was ready and the people inside had their 30 minutes in, the signal was given and the chamber flight was under way.
Under direction of the PTO, the flier did some low-level tasks such as pull pens from pockets, look for the “D” ring on their ejection seat; find their drinking bottles and tube food, inserting them into the feeding port on their helmet and then they tested their manual inflation systems. First they did the press-to-test, which was the back up for the back up and was an all-or-nothing pressurization. Push the button in and the suit inflated, take the finger off and the pressure was released. The flier also experimented with the dial in pressure that would regulate and maintain various pressures. This was used as a primary back up and to assist with the operation of the urine collection device (UCD). After they played with the pressurization system enough to be comfortable with it and ran through the UCD
procedure a couple of times, one of the inside observers came in and did a final re-check of the flier's equipment and the chambers were prepared for separation. Because of the extreme altitude that they would be exposed to from this point on, the guy in the suit was on his own. The door separating the two chambers was closed, the two chamber operators manipulated the atmospheric pressures, and the flier was on their way to a simulated altitude of over 60,000 ft. while the observers on the other side of the glass stayed at between 15,000 and 20,000.
"High Flight"
As the chamber “climbed” in altitude, different things were pointed out to them. One of the main things was how the suit felt as it began to inflate, and to remind the wearer that the suit could inflate to the required pressure without becoming stiff and immobile, which was more often than not the case.
As they passed through 63,000 feet, the leather and suede patches on their suits and gloves began to smoke. Room temperature water in a beaker on a shelf inside the chamber about two feet from the flier began to boil. This was the point where they learned about “Armstrong’s Line”, which is the atmospheric pressure that allows the gasses in fluids to escape from those fluids without the aid of an increase of temperature, and how the body’s various fluids like blood, sinuses, etc. behaved the same way. This is also the point where the PTO pointed out that between the time the water started to boil and the time he finished describing it, the flier would have already been dead for some time had they not been wearing the suit. Even those that had already been in the program for some time showed signs of discomfort after hearing that. They were then walked through their emergency egress checklist and had to find and touch each item while the suit was fully inflated.
After the flier sat above this altitude for a little bit and had the opportunity to realize the potentially fatal situation they were in and gain some faith in their suits, the chamber was vented and brought down to about 25,000 feet and final preparations for the rapid decompression were made. The event was described from beginning to end and the ACM was told what to expect, when to expect it, and what to do. When the crew chief had verified that the main chamber was at the proper altitude and opened the transfer valve, the signal was given and the main chamber operator hit the button. With a loud “BANG!” and a tremendous rush of air, the air in the chamber fogged, papers flew about, the water literally exploded out of the beaker used to demonstrate Armstrong’s Line, the suit got rockhard and the two chambers equalized pressures at about 70,000 feet. (Note: Those that read the previous articles on the suit know that inside the suit, the flier was at an atmospheric pressure that topped
out at about 35,000 feet. After the RD was completed, safety procedures were done again and a normal descent of 5,000 feet per minute was achieved until the main chamber reached the same pressure that the inside observers were at. When this happened, the door opened and the two observers were free to move between the two separate chambers. When the flight was over, the crewmember was unhooked and taken to the suit up room to be undressed while the chamber crew shut the chamber down and the recorder closed out the flight and archived the records for future reference if needed. The suit had a post-flight inspection and was hung back up, ready to be worn again. When all the post-flights were done, records filled out, briefings completed and equipment returned to their rightful places, everyone went back to work doing whatever they were doing before the flight.
The True Spirit of Training:
Chamber training is a vital part in the overall training cycle of any aircrew member. A physiological event is one that holds no preferences or prejudices regarding rank, age, marital status, gender, race, religion or creed. Under the right circumstances it will come upon any one at any time and in the past
has claimed many lives; its process of selecting and claiming its victims is merciless and no one is immune to it. The threat is real and the penalty severe for those who don't respect it. Because the crewmembers receive this specific, in-depth training and used it properly, negative events were rare.
Instructors taught their classes with an intensity born from the mindset that every last one of the students in their class would be needing this training to save their lives the very next time they climbed into a plane. We made sure that not only were the students comfortable with what they had learned, but that we as instructors were confident that they had learned their lessons properly and that they would be able to perform as required.
As long as there are people insistent on doing what is easily the most unnatural thing for humans to do by leaving the earth for extended periods of time, there will always be a small group of people there to teach them how to survive it.
The following article is a true story of an SR-71 pilot that became hypoxic during a training sortie out of Beale AFB in 1986.
Hypoxia, in an SR-71
Author: Terry Pappas, SR-71 Pilot
This story deals with a flight in which I suffered hypoxia symptoms due to a lack of oxygen during an SR-71 sortie out of Beale AFB, California. It happened on
June 9, 1986. I was the newest pilot in the Blackbird, and I was on my second flight in the aircraft. It was in the SR-71B model, which was the only existing
Blackbird with a second set of flight controls, allowing an instructor to check out a new pilot. I was just learning to be accustomed to the pressure suit and the aircraft. I had flown about 150 hours in the flight simulator and one subsonic flight in the aircraft. The first flight was to practice air refueling and landings.
The second flight was my first chance to go “high and hot”, for real. We prepared for each flight by purging all nitrogen from our bodies by pre-breathing 100% oxygen for 45 minutes prior to takeoff.
This minimized the likelihood of a getting the bends if we experienced a problem with aircraft pressurization while at high altitude. My first subsonic flight had included an hour of air refueling practice with one of Beale’s KC-135Q model tankers. It also included 90 minutes in the traffic pattern, flying normal and single-engine approaches and landings. This second flight was special, since it would be my first Mach 3 flight. There was a party planned afterwards and people had come from all over for the event. (Photo: Lockheed)
I had learned some things about the pressure suit and helmet on my first flight. My instructor pilot,
Lt Col Jerry Glasser , had taught me that it was an acceptable technique to unlock and raise the helmet’s Baylor bar while flying in the traffic pattern, as long as you knew you weren’t going back to high speed and altitude conditions. This allowed me to open the helmet’s faceplate, and wipe the sweat out of my eyes occasionally, and still leave the dark visor down to help control glare. In the SR-71 helmet, raising the Baylor bar turned off oxygen flow to the helmet and caused the pilot to breathe
ambient cabin air. The Physiological Support Division (PSD) technicians had taught me to keep the suit and helmet sealed throughout the flight, even until engine shutdown. So I was reluctant to comply with Jerry’s suggestion at first. Finally, I relented and did so for the last half-hour of pattern work on that first flight. The first flight had gone very well, and I was eager for the second flight. It would allow me to fly the Blackbird at Mach 3, which is something that I had practiced in the simulator for five months. I had practiced long and hard for this moment.
Two days later, Jerry and I were strapping into our cockpits for my second flight. As I was doing the preflight checks in the front cockpit, I noticed it was hard to see because the sun was rising, and it was shinning directly into my eyes. The contrast of the bright sun outside and the dark cockpit inside made it difficult to read the instruments. So I put my helmet in the now-familiar configuration of faceplate and dark visor down, and Baylor bar up. I knew the checklist would remind me later to seal the helmet by lowering and locking the Baylor bar.
A few minutes later, when we challenged each other on the configuration of our respective suits and helmets, Jerry said “Baylor bar, latched and locked.” And I repeated this. But I did not actually complete the steps. I noted that my faceplate was down, but I failed to lower and lock the Baylor bar.
During the engine runs that I did at the approach end of the runway, I remember noticing some unfamiliar odors, as I ran each engine to 100% power. It didn’t occur to me at the time that I shouldn’t be able to smell anything, with a properly sealed pressure suit and breathing 100% oxygen.
Soon, we got clearance from the tower for takeoff.
I taxied onto the runway, pushed up the power, got the IGV shift on each engine, released the brakes, and lifted the throttles up and forward into afterburner range. Each afterburner lit abruptly, and things began to happen fast. It’s only two minutes from brake release to level off at 24,000 feet in a
Blackbird, so I had my hands full of 100,000 pounds of airplane screaming upward. We usually flew with a cabin pressure selection of 26,000 feet, so as I leveled off at 24,000 feet enroute to the air refueling point, the cabin was also at 24,000 feet. As most Air Force pilots know, the time of useful consciousness at that altitude is not very long, but it varies with each person and the level of work at hand. Fighting that 50-pound pressure suit and the workload of flying the Blackbird for only the second time, allowed me about three minutes of useful consciousness from the moment I climbed through 12,000 feet.
Soon after leveling off, I began to feel tingling sensations all over. I became warm and felt uncomfortable. These were some of my typical hypoxia symptoms, but they were also slightly different this time, because of the unfamiliar pressure suit. I was concentrating so hard on flying the aircraft that I didn’t notice the symptoms, particularly since I had only experienced them in the suit once, and that was while training in the altitude chamber four months earlier. Within a minute of leveling off, my faculties began to deteriorate. Jerry saw that I was struggling to maintain control of the aircraft, and he asked me about it. I fought even harder to maintain precise control of the
Blackbird. Jerry told me later that he had asked me a few questions to see if I was all there. He said,
“What’s your airspeed?” And I said, “400”, which was true. Jerry said, “What’s your heading?” And
I said, “400”, which was impossible. He immediately took control of the aircraft, declared an emergency, and began a recovery to Beale AFB.
My recollection of the next several minutes of the flight is somewhat incomplete. Jerry swore that I was just “a poor conversationalist for a while”. I think I was out cold. At any rate, I remember regaining my faculties as we were descending through 9,000 feet toward Beale AFB. Jerry asked me how I felt. I said, “Okay.” I thought I could help with some of the switches for the approach, and
landing checklists. He asked me if I could lower the landing gear for him. This is doable from the back cockpit of the B-model, but for systems reasons, we preferred to extend the gear from the front cockpit. I said, “Sure.” I wanted to make the landing. But Jerry wouldn’t let me touch the stick. I couldn’t understand why we were coming back so soon and why he wouldn’t let me fly the airplane. I still didn’t know what had happened.
After the landing and rollout, as we taxied clear of the runway, I got this terribly sinking feeling.
There were a dozen vehicles with red flashing lights waiting for us, and I knew they weren’t there to congratulate me for flying Mach 3. As we shut it down, a pickup truck with a platform above it pulled up beside the aircraft. The first guy to reach the cockpit was the senior PSD supervisor, Tom Bowen .
As he knelt down beside me on the platform, Tom reached forward, put his hand on my helmet and pushed open my faceplate. I thought, “He’s not supposed to be able to do that. I haven’t unlocked my
Baylor bar.” That’s when I realized that I had not locked it. Tom also commented later that he noticed that my helmet configuration was non-standard, and that it was identical to the configuration of the other crewmember, the IP in the back seat.
I had to spend a couple hours in the decompression chamber to preclude getting the bends. Then I was sent to the base hospital for numerous tests to determine if I was okay and to see if there was any explanation for this physiological incident. Fortunately, everything checked out and three days later, I flew Mach 3 for the first time. Of course, we had the requisite party. And you can bet I never again failed to lower and lock my Baylor bar prior to takeoff. In fact, they changed the Blackbird checklist to preclude a similar incident from happening again.
Had we not been able to determine exactly what had happened on that flight, they would have torn the airplane apart trying to find a problem with the oxygen system. Then they would have sent me to
Brooks Army Medical Center in San Antonio and torn my body apart trying to find a problem with me. By the way, the Mission Recording System (MRS) tapes, which normally record everything said by the pilot, even if it’s under his breath, were mysteriously found to be blank. I believe I may owe
Jerry a debt of gratitude for that. I’m thankful to have overcome a somewhat rocky start to the highspeed phase of my flying career. I went on to fly over a hundred missions in the Blackbird. It was the ultimate airplane and mission for an Air Force pilot. I’m honored to have had the opportunity to fly this aircraft in an operational environment, and to work with the professional people who supported it.
I’m sure it will remain the highlight of my aviation experiences.
Terry Pappas
Currently flying as a Research Pilot
NASA Johnson Space Center
Houston, Texas
Credit: This article is copyrighted by Terry Pappas on May 11, 2002. This article may not be reproduced in any format including electronic media retrieval systems without express written permission of the copyright holder. Permission has been granted by Terry Pappas for inclusion on the "SR-71 Blackbirds" web site.
Glenn Chapman, U-2 Pilot is debriefed by Kelly Johnson in this 1950's photo. Note the early style pressure suit Glenn is wearing.
Photo Courtesy Glenn Chapman
The Altitude Chamber at Randolph AFB,Tx in the late '40's
Where to get Training:
The FAA and the U.S. Air Force have a joint training agreement to offer high-altitude, hypobaric chamber training to civilians for a nominal $35.00 fee. Applicants should contact FAA Aeromedical
Education Division (AAM-400), Airman Education Programs, Civil Aeromedical Institute, Oklahoma
City, Okla. at (405) 954-4837 to schedule training sessions at any of the following facilities:
Beale AFB, Marysville, Calif.
Brooks AFB, San Antonio, Texas
Columbus AFB, Columbus, Mich.
Fairchild AFB, Spokane, Wash.
Holloman AFB, Alamogordo, N.M
Langley AFB, Norfolk, Va.
Laughlin AFB, Del Rio, Texas
Little Rock AFB, Little Rock, Ark.
Mike Monroney Aeronautical Ctr., Okla.
Offutt AFB, Omaha, Neb.
Peterson AFB, Colorado Springs, Colo.
Randolph AFB, San Antonio, Texas
Shaw AFB, Columbus, S.C.
Sheppard AFB, Wichita Falls, Texas
Tyndall AFB, Panama City, Fla.
Vance AFB, Enid, Okla.
Wright-Patterson AFB, Dayton, Ohio
Note: All personnel must have a current flight physical and a current DA Form 4186 (Medical
Recommendation for Flying Duty) indicating FFD before participating in any hypobaric chamber exercise.
Editor's note: The altitude chamber at Edwards AFB ceased operation on 11 July 2000 after 43 years of service. The top lead in photo shows the last class attending the Edwards altitude chamber. Most chamber flights reached a simulated altitude of 25,000 to 35,000 feet, with pressure-suit flights up to 100,000 feet.
Credits:
Proofing by: Col. Paul Sheffield, USAF (Ret), Physiological Support Division Unit Commander at
Beale AFB, Ca.
Acknowledgement: "I owe a special debt of gratitude to Dr. Paul Sheffield, Col., USAF (ret), whom I had the distinct honor and privilege of serving under during his assignment as Commander of the
Physiological Support Division, USAF Hospital Beale, Beale AFB, CA 1984-1987. Dr. Sheffield's guidance in the development of this article was invaluable. It is because of his expertise in hypobaric and hyperbaric medicine that I was able to fill in some of the details that had escaped me over the years as well as verify the accuracy of many others. I may have written the article, but Dr. Paul
Sheffield gave it that extra depth not usually found in writings of this nature.
Thank you again, Sir.
Kevin Svetcos
Photos courtesy Lockheed Martin Corporation; USAF, Glenn Chapman, Terry Pappas and Phil
Loignon's SR-71 Photo Archives. Chart graphics courtesy USAF and U.S. Army. HTML formatting and web page design by Leland Haynes, Webmaster, SR-71 Blackbirds.