FORM 22: FIELD NEUROLOGICAL EXAM RECORD FORM
advertisement

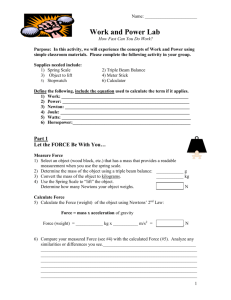
FORM 22: FIELD NEUROLOGICAL EXAM RECORD FORM Diver’s Name: ................................................................... Examiner’s Name: ....................................... Date: ...................... Initial Complaint: ................................................................................................................................................................................ ............................................................................................................................................................................................................ TIME : : : : : : : : : : YES NO YES NO YES NO YES NO YES NO Mental Status: Does he/she know 1. His/her name? 2. Where he/she is? 3. Time of day? 4. Most recent activity? 5.. Speech is clear/correct Sight: 1. Correctly counts fingers? 2. Vision clear? Eye movements: 1. Move in all four directions? 2. Nystagmus absent? Facial Movements: 1. Teeth clench OK? 2. Able to wrinkle forehead 3. Tongue moves in all directions 4. Smile is symmetrical? Head & Shoulder Movements: 1. Adam’s apple movement? 2. Shoulder shrug normal, equal? 3. Head movement normal, equal? Hearing: 1. Normal for that diver? 2. Equal in both ears? Sensations: Present, normal and symmetrical across: 1. Face 2. Chest 3. Abdomen 4. Arms (front) 5. Hands 6. Legs (front) 7. Feet 8. Back 9. Arms (back) 10. Buttocks 11. Legs (back) Muscle Tone: Present, normal and symmetrical for: 1. Arms 1 2. Legs 3. Hand grips 4. Feet Balance and Coordination: 1. Romberg OK? 2. Pulse 3. Respiration Nystagmus – involuntary oscillation of the eyeball. Usually lateral, but sometimes rotary or vertical. Romberg – Patient stands bare footed with feet heel to toe, arms crossed over chest, eyes closed and attempts to remain upright. 2