Integrative Psychology: Theories, Research, and Training
advertisement

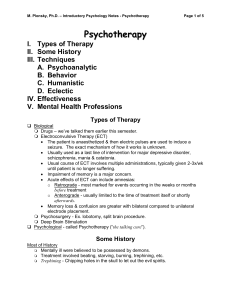
1 Integrative Psychology: History, Research, and Theories Christina Zampitella, Psy.D. Introduction In graduate training, psychologists are exposed to multiple schools of psychology such as psychodynamic, behaviorism, and humanistic approaches. Through our training we learn to apply theories of personality and psychopathology to our clinical cases. As one matures in our personal and professional development, the pure-form orientation with which one may have originally aligned can sometimes feel too narrow to address all clients in all settings. Additionally, we become more aware of alternative modalities of treatment and wellness, often coined as Complementary/alternative medicine (CAM), which is often discussed in the media, but rarely in psychological books, journals, and scholarly presentations (Bassman & Uellendahl, 2003). Psychologists also find that as the field of psychology advances, clients must be conceptualized with the global culture, which identifies a broader, holistic model incorporating mind, body, and the transpersonal. As a result, many psychologists find they begin to pull in other theories, techniques, and interventions from other approaches within and outside of psychotherapy as a way of supplementing their primary orientation. Alford and Beck (1997) state, “Most therapists in ‘single-school’ approaches (like cognitive therapy) do not rigidly believe in their own theories. They do believe in their theories, but only in the restricted sense that the theoretical formulations are advanced as testable hypotheses” (p.277). Consequently, psychologists often find they are more flexible in their treatment of clients. It may take the form of suggesting the client engage in alternative forms of 2 treatment, such as mindfulness, yoga, nature-based assignments, etc, as a compliment to their treatment in the therapy room. Or possibly it is being open to exploring spirituality and incorporating the client’s belief system not only to conceptualization, but also treatment. It also may appear as pulling in approaches from other schools of psychology, such as the empty-chair technique from Gestalt Therapy. This eclectic approach, although with the best intentions to be responsive in meeting the needs of the client, often created a subjective, random, and haphazard treatment plan. Without professional training to guide practitioners in applying alternative and/or complimentary treatment, a coherent and conceptualized application of the approaches can not be ensured. The following article is intended to introduce the emerging field of Integrative Psychology by discussing the historical influences leading to its development, the research that is currently being conducted in the integrative movement, and the theoretical routes towards integration. History of Integrative Psychology Although a complete review of the history of Integrative Psychology is beyond the scope of this article, some of the main influences will be introduced. Readers can find a more in depth discourse in Goldfried and Newman (1992), listed in the references at the end of this paper. It has been primarily in the past 25 years that Integrative Psychology has developed into its own clearly delineated area of interest. However, what perhaps was one of the earliest attempts at integration was at the 88th APA meeting in which French (1933) discussed the parallels between psychoanalysis and behaviorism, specifically how 3 extinction is similar to repression. Needless to say, his speech was met with mixed reactions. In 1934, Kubie supported French’s idea by theorizing that some psychoanalytic techniques in terms of conditioned reflexes. Kubie suggested that Pavlov’s hypothesis that some associations exist outside of an individual’s awareness because of their inhibitions could be treated using the free association technique from psychoanalysis to remove such unconscious obstacles (Goldfried and Newman, 1992). In another attempt to find similarities across psychological approaches, Rosenweig (1936) wrote an article that examined the common elements. He suggested three common factors; (1) the therapist’s personality affected the effectiveness of treatment; (2) interpretations are helpful because they help to reframe one’s problems; and (3) when change occurs in one area of functioning, it often affects other areas of psychological and behavioral functioning. His hypothesis was the first evidence of the common factors theory which has been investigated in greater depth since the 1960’s. A landmark in the history of Integrative Psychology was Dollard and Miller’s (1950) book Personality and Psychotherapy, which described in detail how psychoanalytic concepts such as regression, displacement, and repression may be conceptualized with the framework of learning theory. They contended that there are certain factors common to all therapeutic approaches such as empathy, reinforcement for attempts at changing behavior, and instillation of hope. Furthermore, they supported Herzberg’s (1945) assertion that homework can be used as a compliment to psychoanalysis. They state, “behavioral changes must be made in the real world of the 4 patient’s current life. If benevolent changes are to occur, the patient must be doing something new” (Dollard & Miller, 1950, p.319). In the 1960’s, the Integrative Psychology movement gained significant momentum in the face of many societal changes. Perhaps one of the most important contributions was Frank’s (1961) Persuasion and Healing which addressed the common factors across orientations. He stated that psychotherapy is intended to produce corrections in an individual’s conception of themselves and others. Instillation of hope creates an increase in self-esteem and improved functioning. During this decade, multiple practitioners and theorists (Alexander, 1963; London, 1964; Marks & Gelder, 1966; Rogers, 1963;, and Wolf, 1966) suggested that pure-form approaches to psychotherapy were not sufficient enough to treat all clients in all contexts, and that integration of therapies was inevitable. Although they acknowledged that such integration would be extremely challenging, if not impossible, they believed that the commonalities could increase a practitioner’s repertoire of theories, techniques, and interventions from a more integrative framework. Another very important influence on the Integrative Psychology movement was Lazarus’ (1967) ‘technical eclectic’ approach, which eventually led to the development of multimodal therapy developed in the 1970’s. He suggested that a therapist could utilize techniques from other school of psychology without assimilating the theory associated with the approach. He believed that techniques that were empirically validated could be systematically incorporated into treatment. Moving to the 1970’s, behaviorism was revisited in relation to psychodynamic concepts (Bergin, 1971; Marks, 1971; and Woody, 1971). A flurry of articles and books 5 explored in greater depth the commonalities between theories, and that they were not mutually exclusive, but rather could compliment each other effectively. A shift occurred from opposition to exploration between the orientations, which produced a substantial amount of literature on topics such as the concepts of rapprochement (Wachtel, 1975), convergence of clinical procedures (Wachtel, 1977), and therapeutic integration (Applebaum, 1976; Strupp, 1976; and Wandersmann, Poppen, & Ricke, 1976). In 1976, Lazarus published Multimodal Behavior Therapy which “refined his broad-spectrum approach to behavior therapy so as to systematically take into account the individual’s behaviors, affects, sensations, images, cognitions, interpersonal relationships, and drugs/physiological states (the ‘BASIC I.D.’)” (Goldfried & Newman, 1992, p.58). The 1980’s, integration made significant advancements which produced over 200 articles and boos on the topic (Goldfried & Newman, 1992). Goldfried (1980) suggested that a comparative analysis between theories could be found between specific techniques and theoretical underpinnings of theories, which was termed ‘clinical strategy.’ The sophistication of integrative theories increased during this decade. Other secondary integrative theories, such as cognitive-behavioral, Gestalt, Existential, and neoFreudianism were further evaluated for their ability to compliment each other and how they could integrate with the original ‘Big Three’ schools of psychology; psychodynamic, behaviorism, and humanistic. Conferences on the topic of integration emerged, if not informally, and communication between practitioners and researches expanded into the international arena. Books addressing eclectic approaches (Beuler, 1983) addressed what techniques could be used for which type of client at what particular time by which therapist. Client-technique matching emerged as a result. Conceptualization of treatment 6 from an integrative perspective also originated. For example, Fensterheim and Glazer (1983) suggested that a psychoanalytic approach could be used to formulate assessment hypothesis while a behavioral approach could be adopted to encourage behavior changes. In 1983, the Society for the Exploration of Psychotherapy Integration (SEPI) was established with the intention of creating a place for professionals interested in Integrative Psychology to discuss and research integrative theories and techniques. SEPI is now internationally recognized as an organization formally dedicated to the sharing of ideas. Journals also began to emerge, such as the Journal of Integrative and Eclectic Psychotherapy and the International Journal of Eclectic Psychotherapy. These journals not only address theoretical concepts, but also integrative training and supervision models. In 1988, NIMH sponsored a workshop in psychotherapy integration. It was their belief that “treatments of greater efficacy, efficiency, and safety will result from efforts to integrate the best elements from different school of psychotherapy. In addition, research on integrated treatment models may lead to the development of a comprehensive model of psychotherapy process that will have a solid empirical backing” (Norcross & Goldfried, 1992, p. 4). Other topics, such as psychopharmacology treatment, spirituality, alternative wellness models, and cultural and ecological dimensions of human development were discussed in terms of psychological assessment and treatment. Multicultural concepts were employed in greater detail, and different modalities of treatment (i.e., individual and marital/family counseling) were emerging. Then towards the end of the 1980’s, the focus on the development of empirical methodology emerged stronger than ever. 7 The 1990’s proved to be a move towards empirically supported or validated treatment models, known as EVT. The American Psychological Association has supported the call for EVT’s, which represent treatment programs for specific disorders that have shown to have significant effectiveness via well-designed and controlled outcome studies. However, most of these treatment models are behavioral or cognitivebehavioral with a spattering of interpersonal therapy and brief dynamic therapy (Glass, Arnkoff, & Rodriguez, 1998). This movement has proven to be an area of hot debate, as integrative theorists have argued that manualized treatments for specific disorders will hinder the integrative movement by reducing the innovative work of those therapists trying to match treatment to a client’s problems. Others are concerned that EVT may squelch dialogue regarding common factors, prescriptive matching, and newly developing integrative therapies (Garfield, 1998). Yet other integrationists feel that EVT will force the Integrative Psychology field to attend to the discrepancy between research and practice, which may prove beneficial in the long run (Goldfried & Wolfe, 1998; Shohan & Rohrbaugh, 1996). Now, in the new millennium, research and theory is focusing on the development of different routes towards integration. Discussion of the current key areas of investigation is also beyond the scope of this article. Briefly, those areas are; (1) combining techniques from existing approaches; (2) prescriptive matching and eclectic psychotherapy, including client-treatment matching, systematic treatment selection, and multimodal therapy; (3) common and specific change factors across different pure-form therapies; (4) psychotherapy derived from integrative theories of psychological disorders; 8 and psychotherapy derived from integrative models of therapeutic change, including the transtheoretical approach, cognitive analytic theory, process-experiential therapy, and EMDR and reprocessing (Glass et al., 1998). While the above five areas of investigation can not be covered here, the six distinct movements that have been cultivated over the past 10 years can be briefly discussed. Integrative Psychology Approaches Integrative Psychology, regardless of the approach one might take, strives for in creasing therapeutic efficacy, efficiency, and applicability by looking beyond the confines of single theory and technique. There are many routes by which the school of Integrative Psychology is attempting to accomplish this goal (the following was adapted from Gilbert & Evans, An Introduction to Integrative Psychotherapy, 1995); 1. 2. 3. 4. 5. 6. Meta-theoretical integration; Technical eclecticism; Common factors; Assimilative integration; Complimentary; and, Neurobiological. The meta-theoretical models of Wilber (1980), Clarkson (1990), and Opazo (1997) are examples of a theory of theories, spanning all approaches to psychotherapy, often focusing on the commonalities between schools of psychology. It attempts to provide an overall map or narrative to inform conceptualization of the client and treatment utilizing a significantly modified theory of human beings. Norcross & Napolitano (1986) state, “The eclectic selects among several dishes combining different ingredients, the integrationist creates new dishes by combining new ingredients” (p.7). 9 The main criticism of the meta0theoretical approach is that it is too idealistic to be practically applied. Second is the technical eclectic approach (originally inspired by Lazarus in 1967) , which is an empirically supported form of integration that focuses not on theory of personality or psychopathology, but rather on validated interventions that work for a specific individual for a specific problem (i.e., systematic desensitization). It often is approached by assessing the client’s problems followed by systematically choosing interventions appropriate to the client’s location in the change process (i.e., precontemplation, contemplation, or action). Lazarus (1967) suggested that a metatheoretical approach is impractical. He states, “To attempt a theoretical rapprochement is as futile as trying to picture the edge of the universe. But to read through the vast amount of literature on psychotherapy, in search of techniques, can be clinically enriching and therapeutically rewarding” (p. 416). The main criticisms are that this approach does not address the possible incompatibility between technique and other aspects of therapists’ practice. It also does not consider the client’s entire worldview, including cultural, ecological, or transpersonal dimensions of functioning and self-conceptualization. The third approach to psychological integration in the common factors model. As previously discussed, this model’s roots span to the 1930’s and focuses on the commonalities between approaches such as instillation of hope, empathy, acceptance, corrective emotional experiences, etc. Some theorists are now focusing on a common language between theories, which in turn is hoped to increase dialogue across theoretical barriers. The main criticism of this approach is that if therapy is based on common factors alone, one may lose the richness of highly developed theories and techniques. 10 Fourth, the assimilative integration route is characterized by a gradual assimilation of techniques and concepts into the psychologist’s original theoretical orientation. The meaning of new concept interacts with the original orientation, and as a result, transforms both. The goal is to maintain one’s original theoretical orientation while using empirically validated techniques to fill in the gaps that the original orientation is unable to fill in an unaltered state. The result is to have a theoretically meaningful and clinically appropriate orientation. The main criticism to this approach is that the power of the original orientation may become too diluted. The complimentary approach is the fifth route towards Integrative Psychology. This is when two or more distinct approaches contribute to the final product. For example, Linehan’s Dialectical Behavior Therapy (1993) combines Zen awareness and acceptance with Behavior Therapy to focus on overt behavioral changes. The criticism to this approach is that each approach or contributions may become unintentionally lost in the compliment. Finally, the sixth approach to Integrative Psychology is the neuroscience route. The main focus is the neurobiological underpinnings of psychological processes, such as with attachment between the primary caregiver and the child. For example, Schore (2003) suggests that the non-verbal conveyance of empathy (right-hemisphere) “allows for dysregulations in a client to be corrected in an atmosphere of mutuality” (as cited in Evans & Gilbert, 2005, p.32). The criticism is that research is very new and does not yet provide evidence for integration. 11 Conclusion Integrative Psychology is a continuously developing theoretical orientation with roots spanning over 70 years. As psychology’s understanding of the person continues to expand, the need for an integrative orientation will increase because of its ability to hold all domains of an individual’s holistic existence in a coherently conceptualized construct. Such an approach affords psychologists the opportunity to utilize a variety of traditional treatments with alternative modalities of complimentary techniques. All this, while maintaining a firm stance in a sound understanding of the uniqueness and contextual processes of the client and the therapeutic relationship. I shall end with a poignant quote, as it sums up the intention of this article. Greben (2004) writes, “Proponents of both traditional and newer unimodal psychotherapeutic disciplines can well remain highly valued within this broader integrative clinical…context, with the relevance of their approaches to general [psychological] care reaffirmed rather than threatened” (p.245). References Alford, B. & Beck, A. (1997). The relation of psychotherapy integration to the established systems of psychotherapy. Journal of Psychotherapy Integration, 7(4), 275-289. Applebaum, S. (1976). A psychoanalyst looks at gestalt therapy. In C. Hatcher & P. Himmelstein (Eds). The handbook of gestalt therapy. New York: Jason Aronson. Applebaum, S. (1979). Out in inner space: A psychoanalyst explores the therapies. Garden City, NY: Anchor. Bassman, L., $ Uellendahl, G. (2003). Complementary/alternative medicine: Ethical, professional, and practical challenges for psychologists. Professional Psychology: Research and Practice, 34(3), 264-270. Bergin, A. (1971). The evaluation of therapeutic outcomes. In A.E. Bergin & S. L. Garfield (Eds.) Handbook of psychotherapy and behavior change. New York: Wiley. Beutler, L. (1983). Eclectic psychotherapy: A systematic approach. Elsmford, NY: Pergamon. Clarkson, P. (1990). A multiplicity of psychotherapeutic relationships. British Journal of Psychotherapy, 7(2), 148-163. 12 Dollard, J., & Miller, N. (1950). Personality and Psychotherapy. NY: McGraw-Hill. Fensterheim, H., & Glazer, H. (Eds). Behavioral psychotherapy: Basic principles and case studies in an integrative clinical model. NY: Brunner/Mazel. Frank, J. (1961). Persuation and healing. Baltimore: Johns Hopkins University Press. French, T. (1933). Interrations between psychoanalysis and the experimental work of Pavlov. Ameerican Journal of Psychiatry, 89, 1165-1203. Garfield, S. (1998). Some comments on empirically supported treatments. Journal of Consulting and Clinical Psychology, 66, 121-125. Gilbert, K., & Evans, M. (2005). An introduction to integrative psychotherapy. NY: Palgrave-MacMillan. Glass, C., Arnkoff, D., & Rodriguez, B. (1998). An overview of directions in psychotherapy integration research. Journal of Psychotherapy Integration, 8(4), 187-209. Goldfried, M. (1980). Toward the delineation of therapeutic change principles. American Psychologist, 35, 991-999. Goldfried, M. & Newman, C. (1992). A history of psychotherapy integration. In Norcross, J. & Goldfried, M. (Eds). The handbook of psychotherapy integration. New York: Basic Books. Goldfried, M. & Wolfe, B. (1998). Toward a more clinically validated approach to therapy research. Journal of Consulting and Clinical Psychology, 66, 143-150. Greben, D. (2004). Integrative dimensions of psychotherapy training. Canadian Journal of Psychiatry, 49(4), 238-248. Herzberg, A. (1945). Active psychotherapy. New York: Grune & Stratton. Kubie, L. (1934). Relation of the conditioned reflex to psychoanalytic technique. Archives of Neurology and Psychiatry, 32, 1137-1142. Lazarus, A. (1967). In support of technical eclecticism. Psychological Reports, 21, 415-416. Lazarus, A. (1976). Multimodal behavior therapy. New York: McGraw-Hill. Lazarus, A. (2005). Is the still a new for psychotherapy integration? Current Psychology: Developmental, Learning, Personality, Social, 24 (3), 149-152. Linehan, M. (1993). Cognitive-behavioral treatment for borderline personality disorder. New York: Guilford Press. Marks, I. (1971). Common ground between behavior therapy and psychodynamic models. British Journal of Psychiatry, 118, 69-73. Norcross, J. & Goldfriend, M. (Eds.). (1992). Handbook of psychotherapy integration. New York: Basic Books. Norcross, J., & Napalitano, G. (1989). Defining our journal and ourselves. International Journal of Eclectic Psychotherapy, 5, 249-255. Opazo, R. (1997). In the hurricane’s eye: A superparadigmatic integrative model. Journal of Psychotherapy Integration, 7(1), 17-54. Rosenweig, S. (1936). Some implicit common factors in diverse methods in psychotherapy. American Journal of Orthopsychiatry, 6, 412-415. Schore, A. (1994). Affect regulation and the origin of the self. Hillside, NJ: The Analytic Press. Shoham, V., & Rohrbaugh, M. (1996). Promises and perils of empirically supported psychotherapy integration. Journal of Psychotherapy Integration, 6, 191-206. 13 Strupp, H. (1976). Some critical comments on the future of psychoanalytic therapy. Bulletin of the Menninger Clinic, 40, 238-254. Wachtel, P. (1975). Behavior therapy and the facilitation of psychoanalytic exploration. Psychotherapy: Theory, Research, and Practice, 12, 68-72. Wachtel, P. (1977). Psychoanalysis and behavior therapy: Towards an integration. New York: Basic Books. Wandersmann, A., Poppen, P., & Ricks, D. (Eds.). (1976). Humanism and behaviorism: Dialogue and growth. Elmsford, NY: Pergamon. Wilber, K. (1980). The atman project. Illinois: Quest. Woody, R. (1971). Psychobehavioral counseling and therapy: Integrating behavior and insight techniques. New York: Appleton-Century-Crofts.