DONOR INSEMINATION
ISO
certified
9001:2008
1
CONTACT NUMBERS ........................................................................................................... 2
2
OPENING HOURS ................................................................................................................. 2
3
Background .......................................................................................................................... 3
4
What is Donor Insemination ................................................................................................ 3
5
Who are the donors? ........................................................................................................... 3
6
Matching ............................................................................................................................... 4
7
Before treatment starts ........................................................................................................ 4
8
General Advice ..................................................................................................................... 4
8.1 Folic Acid ............................................................................................................................... 4
8.2 Smoking................................................................................................................................. 5
8.3 Alcohol ................................................................................................................................... 5
8.4 Rubella .................................................................................................................................. 5
8.5 Tubal patency test ................................................................................................................. 5
9
Treatment .............................................................................................................................. 5
9.1 Natural cycle .......................................................................................................................... 5
9.2 Stimulated cycle (Superovulation and Donor Insemination (SO + DIUI) ........................... 6
9.3 What is a treatment cycle? ................................................................................................. 7
9.4 Who will do my injections? ................................................................................................... 7
9.5 How long will I be on injections for? ....................................................................................... 8
9.6 Are there any risks ? ........................................................................................................... 8
10 Further attempts ................................................................................................................... 8
11
Treatment for Sibling Pregnancy ........................................................................................ 9
12
Confidentiality ...................................................................................................................... 9
13
HFEA Register ...................................................................................................................... 9
14
What is the success rate? ................................................................................................. 10
15
Will the pregnancy be normal? ......................................................................................... 10
16
Costs ................................................................................................................................... 11
17
Are there any problems? ................................................................................................... 11
18
Welfare of the Child............................................................................................................ 11
19
Counselling......................................................................................................................... 12
20
Parental Responsibility ...................................................................................................... 12
21
Outcome of Treatment ....................................................................................................... 13
22
Complaints.......................................................................................................................... 13
M Rajkhowa/E Lowe, April 2007
Revision: 09
Reviewed: August 2014
Due for review: August 2015
Authorised
QM A McConnell
D:\533562538.doc PL013
© 2007, ACU Dundee – all rights reserved
Page 1 of 13
DONOR INSEMINATION
1
CONTACT NUMBERS
Ward 35
01382 633835 (voicemail outwith 8.00 am – 5 pm)
Appointment secretary
01383 496475 (8.45 am – 4.45 pm)
Anne McConnell
01382 632111 (voicemail outwith 8 am – 5.30 pm)
Email anne.mcconnell@nhs.net
Dr V Kay/
01382 632111
Dr S Kini/
Dr S Martins da Silva/
Dr N Patravali
Emergency calls for medical staff outwith 8.00 am – 5 pm –
mobile ‘phone 07774 694765
2
OPENING HOURS
The Unit is open 8 am to 5 pm Monday – Friday and
8 am – 12 noon, Saturday and Sunday
M Rajkhowa/E Lowe, April 2007
Revision: 09
533562538
Page 2 of 13
© 2007, ACU Dundee – all rights reserved
DONOR INSEMINATION
3
Background
Male infertility is an increasing problem and some 25% of all couples who are infertile
probably have a sperm problem as the main cause.
However, the requirement for donor
insemination has fallen in recent years due to the development of new techniques for
previously
untreatable
male
infertility,
particularly
surgical
sperm
recovery
and
intracytoplasmic sperm injection, or ICSI. There are still many occasions where even this is
not possible, or couples may prefer not to use this and donor insemination (DI) provides them
with a chance to have their own child.
4
What is Donor Insemination
Sperm donated by a fertile man (the donor) and are used instead of the partner's sperm to
try to produce a child. The donor's sperm are transferred through the cervix to the woman
using a small cannula.
5
Who are the donors?
They are all healthy men who donate semen on a voluntary basis.
They may or may not
already have a family. Before accepting a new donor we check their medical history and carry
out several tests to try to exclude any infectious diseases which might be passed on; in
particular, all donors are screened for hepatitis and the AIDS viruses as well as sexually
transmitted diseases. We are also careful to accept only those men who have a healthy
family background and we will not accept a donor if there is any suggestion of inherited
disease. In addition, all donors are screened for cystic fibrosis.
M Rajkhowa/E Lowe, April 2007
Revision: 09
533562538
Page 3 of 13
© 2007, ACU Dundee – all rights reserved
DONOR INSEMINATION
6
Matching
As far as possible we try to match the general characteristics, e.g. height, hair and eye
colour. Often exact matching is not possible because of a shortage of donors. However, it is
a fact that there is a very great variation in the characteristics of children even when both
partners are the natural parents.
We may have donors from different ethnic backgrounds
and you should let us know if this is something you are prepared to accept.
7
Before treatment starts
Before agreeing to go ahead with treatment, we advise that you meet with our fertility
counsellor, Anne Chien to discuss the implications of this treatment, particularly for
yourselves and for any children you might have.
You will also meet with one of our fertility
nurses who will discuss the procedure with you and take bloods for screening. You should be
aware that there may be a delay before treatment can commence, due to the shortage of
suitable samples. A senior nurse from the Unit will contact you when we are able to offer you
treatment.
8
8.1
General Advice
Folic Acid
There is very real evidence that the incidence of abnormalities of the brain and spine of a
baby are greatly reduced if patients are taking Folic Acid at the time of conception and
thereafter. Please have a word with your own doctor about this, or you can buy appropriate
supplements at any chemist. Please start to take these supplements at any time prior to
treatment.
M Rajkhowa/E Lowe, April 2007
Revision: 09
533562538
Page 4 of 13
© 2007, ACU Dundee – all rights reserved
DONOR INSEMINATION
8.2
Smoking
There is data available to show that the likelihood of treatment being successful is reduced
if patients smoke. We cannot emphasise too strongly the advantages of stopping before
starting treatment. For NHS funded treatment, both partners must be non-smokers.
8.3
Alcohol
We do recommend that couples trying to conceive should take less than 4 units of alcohol per
week.
8.4
Rubella
We would expect all women to have had a check that they are immune to rubella prior to
starting treatment. If not immune, immunisation should be arranged through your general
practitioner at least one month before starting treatment.
8.5
Tubal patency test
Depending on your medical history, your clinician may carry out either a laparoscopy or HSG
(hysterosalpingogram) to check tubal patency either before you start treatment or if the
first three cycles of treatment have been unsuccessful.
Depending on your medical history, generally we will offer three cycles of treatment in a
natural cycle, followed by three further treatment cycles using drugs (tablets or injections)
in stimulated cycles.
9
9.1
Treatment
Natural cycle
Insemination will be carried out at the fertile time of your cycle. This occurs approximately
14 days before your next period. Some women are aware of their fertile time as the amount
of vaginal discharge increases and becomes clearer. We recommend the use of an ovulation
M Rajkhowa/E Lowe, April 2007
Revision: 09
533562538
Page 5 of 13
© 2007, ACU Dundee – all rights reserved
DONOR INSEMINATION
predictor kit to detect your most fertile time. The kits are based on detecting a colour
change in urine which represents increased levels of the hormone "LH" that occurs just prior
to ovulation. When your kit turns positive, you should telephone the Unit and speak to the
infertility nurse on duty, who will arrange a suitable time for insemination. The telephone
number is 01382 633835. Insemination will usually be within 24 hours of the kit turning
positive.
Insemination will be carried out in the Assisted Conception Unit, Ward 35 of Ninewells
Hospital. If you think your kit will go positive over the weekend, you should contact the Unit
on the Friday to ensure that staff will be available to carry out insemination at the weekend.
Do not hesitate to contact the nursing staff if you have any problems with the kits.
Patients sometimes require a fertility drug to help stimulate the ovaries;
9.2 Stimulated cycle (Superovulation and Donor Insemination (SO + DIUI)
This treatment will usually be offered if three cycles of insemination in a natural cycle have
been unsuccessful. Usually a tubal patency test (HSG or laparoscopy) will be performed prior
to commencing this treatment.
Superovulation is the use of daily injections of a gonadotrophin hormone called FSH (Follicle
Stimulating Hormone) to stimulate the ovary to produce up to two to three follicles within a
cycle with the aim of enhancing the chances of fertilisation and conception.
This is
monitored with vaginal ultrasound scans (follicle tracking) to monitor the growth of the
follicles. When the largest follicle reaches 17-18 mm in size and injection (Ovitrelle) is given
to mature and release the egg. The release of the egg(s) (ovulation) into the fallopian tube
usually occurs 36-4 hours after this injection.
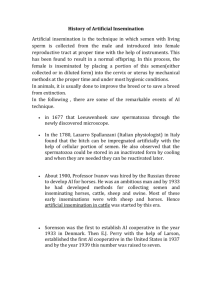
Intrauterine Insemination (IUI) involves inserting the prepared sample of donor sperm into
the uterine cavity (womb) to coincide with ovulation, in order to increase the chances of
conception taking place. The prepared sample is processed in a very small volume and passed
M Rajkhowa/E Lowe, April 2007
Revision: 09
533562538
Page 6 of 13
© 2007, ACU Dundee – all rights reserved
DONOR INSEMINATION
through the cervix, using a fine tube (catheter) into the upper part of the uterus (womb).
This procedure is very similar to a cervical smear test. The procedure takes only a few
minutes. After this you rest for a short while and then go home.
tube
uterus
ovary
cervix
You will usually be offered a maximum of three cycles of treatment including only those
cycles where insemination has been performed, provided there are no medical contraindications.
9.3 What is a treatment cycle?
Day one of your cycle is the first day of bleeding when you get your period. We would ask you
to contact the nursing staff on the ACU to arrange a scan for day three of your cycle (you
will still be bleeding but this is quite normal). Providing the scan shows that both ovaries are
“quiet” (do not contain follicles or cysts) and the lining of the womb is thin, then you will be
ready to start daily injections. A scan appointment will be arranged for you to monitor your
response to the drugs after about 5 days. Further appointments will depend on your response
to the injections.
9.4 Who will do my injections?
We will teach you how to self-inject. If you prefer you can ask your partner or a friend or
your practice nurse to help you.
M Rajkhowa/E Lowe, April 2007
Revision: 09
533562538
Page 7 of 13
© 2007, ACU Dundee – all rights reserved
DONOR INSEMINATION
9.5
How long will I be on injections for?
It is difficult to predict how you will respond to the dose of drugs prescribed for you, but on
average we would expect you to be on injections for seven days. Depending on your response
you should on average have a minimum of three scans.
9.6 Are there any risks ?
Multiple pregnancy: An obvious concern is that this might lead to a multiple pregnancy and
even when ultrasound is used to monitor the ovaries, the risk cannot be entirely removed.
Twins, but more particularly pregnancies with triplets or more, carry significant risks. There
is an increased risk of miscarriage and premature labour; with prematurity comes the risk of
long term health problems or disability. We try to keep the number of multiple pregnancies as
small as possible, but it is important that you understand the risks before starting. N.B if
more than three follicles of 15mm are recorded treatment will be abandoned and
protected intercourse advised.
Ovarian Hyperstimulation Syndrome (OHSS): This is rare, but potentially a very serious
condition that can happen when too many follicles grow. The symptoms include abdominal
discomfort, nausea and difficulty in breathing. Careful monitoring will usually identify those
at risk and OHSS can be prevented by abandoning the treatment cycle. In extreme cases
hospitalisation may be needed but simple measures often suffice and a contact number is
provided for all patients.
10 Further attempts
If the treatment is unsuccessful, we will continue to offer you D.I. on a monthly basis for a
total of six cycles, if that is what you wish. This will be dependent on the supplies of donor
sperm available in the sperm bank. At the end of six cycles (natural and stimulated) a review
appointment will be arranged with the doctor to consider other treatment options such as
IVF.
M Rajkhowa/E Lowe, April 2007
Revision: 09
533562538
Page 8 of 13
© 2007, ACU Dundee – all rights reserved
DONOR INSEMINATION
11 Treatment for Sibling Pregnancy
We know that patients who are successful in having a child as a result of donor insemination
may wish to have further treatment using sperm from the same donor. While we will try to
offer this if possible, we cannot guarantee that these will be available and it is important to
remember that sperm can only be stored for a maximum of ten years from the date of
donation and patients requesting treatment beyond this date would have to use sperm from a
different donor.
12 Confidentiality
The D.I. clinic records are kept separately from the main hospital records. We would usually
write to your doctor with details of the treatment but can only do so with your written
permission. You may prefer not to have any information passed outside the Unit and should
discuss this with your consultant.
13 HFEA Register
The HFEA keeps a confidential register of information about donors, patients and
treatments. This register was set up on 1st August 1991 and therefore contains information
concerning children conceived from licensed treatments from that date onwards.
As from the year 2008, people aged 16+ (if contemplating marriage) or 18, who ask the HFEA,
will be told whether or not they were born as a result of licensed assisted conception
treatment, and if so, whether they are related to the person they want to marry.
Until 2005, donors could choose to remain anonymous and, although they had to give
identifying details for the HFEA register, these remained confidential. However, on 1st April
2005, the law changed to allow people conceived through donation to find out who the donor
was, once they reach the age of 18; the HFEA are legally obliged to contact and forewarn
donors if such a request is made.
M Rajkhowa/E Lowe, April 2007
Revision: 09
533562538
Further changes to the HFE Act apply from 1st October
Page 9 of 13
© 2007, ACU Dundee – all rights reserved
DONOR INSEMINATION
2009 which mean that donor-conceived people over 16 years of age will be able to access
anonymous information about their donor and find out whether they have any genetically
related donor conceived siblings. They will also be able to make contact with genetically
related donor-conceived siblings (provided both parties consent).
At your request, we can provide you with non-identifying information about donors.
14 What is the success rate?
The likelihood of pregnancy is rather lower than that which is achieved under normal
conditions with fertile couples. In the year ending 30th June 2012 the live birth rate per
treatment cycle started was 13.5% and the continuing pregnancy rate for the year ending 31st
December 2013 was 12.3%.
As with other fertility treatments, it tends to be more
successful in younger women *. There were no twin pregnancies during this period. The
chances of the first cycle being abandoned for over or under response may be up to 30%.
Triplet pregnancies can occasionally result even if there are only two follicles due to one
fertilised egg forming identical twins.
If the treatment is successful, you will have an
appointment made for an early pregnancy scan approximately five weeks later.
*Because the success rate with donor insemination in older women is very poor (approximately
4%) and there is a shortage of sperm donors, we are unable to offer treatment to women
aged 40 and over.
15 Will the pregnancy be normal?
The risks of a child from D.I. being born with a congenital problem or handicap are exactly
the same as for any other pregnancy. There are no special risks of D.I. and we would advise
routine antenatal care for any such pregnancy.
This would normally include an offer of
antenatal screening and the risks of an unexpected birth abnormality are small.
M Rajkhowa/E Lowe, April 2007
Revision: 09
533562538
Page 10 of 13
© 2007, ACU Dundee – all rights reserved
DONOR INSEMINATION
16 Costs
For patients who are eligible for NHS-funding there is no charge to patients. For those who
do not meet the criteria for NHS funding, the cost per cycle is £430 in an unstimulated
cycle. For stimulated cycles, the charge is £590 which includes the cost of drugs.
17 Are there any problems?
There are many possible problems - here are some examples:
1.
People react differently to the actual process of D.I. Some partners accept it quite
readily. Others find it upsetting. If either of you is upset be sure to talk it over with
the other. You may want to talk it over with your consultant, infertility nurse or involve
our independent counsellor.
2. Couples should decide themselves whether to tell any children born by D.I. of their
biological origins. Clearly, you would be under no obligation to do so, but there is some
evidence from work carried out on adoption that it is well worth considering telling your
child at a fairly early stage, just in case they should find out accidentally at a later time.
This might be an area that you could explore in counselling, but obviously if donor
insemination is carried out for some genetic problem in either partner, then it is even
more important that any child should be told of this.
18 Welfare of the Child
The Human Fertilisation and Embryology Act of 1990 requires that the welfare of the child
(or any existing children) must be taken into account before treatment can start. (A separate
leaflet covering the HFEA statement on this is included).
M Rajkhowa/E Lowe, April 2007
Revision: 09
533562538
Page 11 of 13
© 2007, ACU Dundee – all rights reserved
DONOR INSEMINATION
19 Counselling
Implications counselling will be organised for patients who are considering treatment which
involves either donating (including sharing) or using donated eggs, sperm or embryos and also
for those considering surrogacy.
Implications counselling enables you to consider your
thoughts and feelings about the complex emotional, practical and ethical issues around such
treatment in a supportive way. You will be encouraged to consider how you might manage the
information around donation or surrogacy and how that might impact on yourselves, any child
born as a result and on others involved in your treatment. Each counselling session lasts
around an hour and your counsellor can help you to decide about further appointments. This
counselling is not an assessment, it is to help you make a fully informed decision about your
treatment.
20 Parental Responsibility
From 6th April 2009, the law with regards to parenthood changed.
Where couples are
unmarried, it is now possible for the male partner to be legally recognised and named on the
child’s birth certificate, but only if both partners consent to this. We will provide you with
these consent forms.
Same sex couples who are not in a legal partnership can also consent
to the partner who does not give birth being named as the second legal parent.
For married couples, the situation has not changed. The husband will be the legal father of
any child born as a result of treatment (unless he does not consent to this treatment).
M Rajkhowa/E Lowe, April 2007
Revision: 09
533562538
Page 12 of 13
© 2007, ACU Dundee – all rights reserved
DONOR INSEMINATION
21 Outcome of Treatment
We have an obligation to inform the Licensing Authority of every donor insemination,
therefore we emphasise the importance of letting us know the outcome of each treatment
cycle. Please keep in touch with Anne McConnell.
22 Complaints
If you feel that there is any area for complaint regarding your treatment, there are various
ways to deal with this;
1.
Contact Anne McConnell at the Assisted Conception Unit.
2.
Contact the Consultant in charge of your care.
3.
The Trust also has its own complaints procedure which you may wish to use. The
normal process would be for patients to write to the Chief Executive of the Trust;
however, any correspondence may be read by other members of his staff or those
working in the Patient Liaison Service, therefore you must bear in mind that, although
the normal rules of confidentiality would apply, the special protection offered by the
Human Fertilisation and Embryology Act for patients undergoing assisted conception
treatment would not be followed.
You may therefore wish to address any letters of
complaint to either of the following, c/o the Assisted Conception Unit, Ward 35;
Alison Moss, Complaints and Feedback Team Lead
Ms L McLay, Chief Executive
The above are both named on our licence held by the HFEA.
M Rajkhowa/E Lowe, April 2007
Revision: 09
533562538
Page 13 of 13
© 2007, ACU Dundee – all rights reserved