Queen Mary`s Hospital, Sidcup, Kent DA14 6LT
advertisement

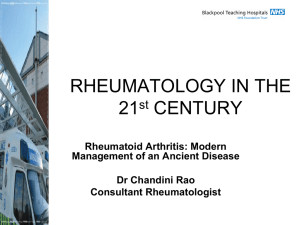
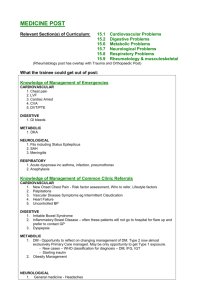
Queen Mary's Hospital, Sidcup, Kent DA14 6LT Service review: Department of rheumatology: September 2006 Dr Andrew Bamji FRCP Lead clinician Introduction What is Rheumatology? A subspecialty of internal medicine that involves the non-surgical evaluation and treatment of the rheumatic diseases and conditions. Rheumatic diseases and conditions are characterised by symptoms involving the musculoskeletal system. Many of the rheumatic diseases and conditions feature immune system abnormalities. Therefore, rheumatology also involves the study of the immune system. What is a Rheumatologist? A rheumatologist is a physician who is qualified by additional training and experience in the diagnosis and treatment of arthritis and other diseases of the joints, muscles and bones. Many rheumatologists conduct research to determine the cause and better treatments for these disabling and sometimes fatal diseases. What kind of training do rheumatologists have? After four or five years of medical school and three years of training in either internal medicine, rheumatologists devote an additional four years to specialized rheumatology training. What do rheumatologists treat? Rheumatologists treat arthritis, certain autoimmune diseases, musculoskeletal pain disorders and osteoporosis. There are more than 100 types of these diseases, including rheumatoid arthritis, osteoarthritis, gout, lupus, back pain, osteoporosis, fibromyalgia and tendonitis. Some of these are very serious diseases that can be difficult to diagnose and treat. Service Review: Dept of rheumatology, Queen Mary's Sidcup NHS Trust 1 Injection of the carpal tunnel When should you see a rheumatologist? If musculoskeletal pains are not severe or disabling and last just a few days, it makes sense to give the problem a reasonable chance to be resolved. But sometimes, pain in the joints, muscles or bones is severe or persists for more than a few days. At that point, you should see your physician. Many types of rheumatic diseases are not easily identified in the early stages. Rheumatologists are specially trained to do the detective work necessary to discover the cause of swelling and pain. It's important to determine a correct diagnosis early so that appropriate treatment can begin early. Some musculoskeletal disorders respond best to treatment in the early stages of the disease. Because some rheumatic diseases are complex, one visit to a rheumatologist may not be enough to determine a diagnosis and course of treatment. These diseases often change or evolve over time. Rheumatologists work closely with patients to identify the problem and design an individualized treatment program. Children are not immune to arthritis How does the rheumatologist work with other health care professionals? The role the rheumatologist plays in health care depends on several factors and needs. Typically the rheumatologist works with other physicians, sometimes acting as a consultant to advise another physician about a specific diagnosis and treatment plan. In other situations, the rheumatologist acts as a a manager, relying upon the help of many skilled professionals including nurses, physical and occupational therapists, psychologists and social workers. Team work is important, since musculoskeletal disorders are chronic. Service Review: Dept of rheumatology, Queen Mary's Sidcup NHS Trust 2 Health care professionals can help people with musculoskeletal diseases and their families cope with the changes the diseases cause in their lives. Rheumatologists also work closely with orthopaedic surgeons, who perform joint replacements, soft tissue reconstruction and repair and nerve decompression, and with radiologists who report on X-rays, CT, MRI and ultrasound scans. They may also call upon neurosurgeons (in particular for neck and back problems). Population needs Current RCP guidelines for Consultant Rheumatologist numbers suggest a norm of 1 consultant to 85,000 population. Based on a local population of 220,000 for Bexley Borough that represents a requirement of 2.6 wte posts. QMH has 1.75. The Rheumatology unit at Queen Mary's Hospital See “Hospital Doctor” Team of the Year submission, 2005 (appendix 1). The department sees all rheumatological problems and runs clinics both at QMH and Erith. An emergency access system is available for patients with an acute flare-up of one or more joints. Dr Bamji sees children with arthritis. The back pain triage service has significantly reduced inappropriate referrals to orthopaedics and the Pain Clinic and has had an enormous impact on the waiting time to first appointment in these and the rheumatology departments. Staffing The department has acquired associated staff who have helped to achieve the current ARMA Standards of Care (specialist nurse – essential for biologics monitoring and the helpline; specialist physiotherapist(s) for back and knee pain and a specialist OT for hand work. These latter are also important for the orthopaedic team). The specialist nurse post has been the subject of review and was put “at risk” as part of the Fit for Future programme. The department’s response was robust – see Appendix 2. It is now accepted that a specialist nurse (or more than one) is essential to the management of patients with chronic rheumatic diseases and this is acknowledged both in Royal College and Arthritis & Musculoskeletal Alliance (ARMA) guidelines as well as in the new Musculoskeletal Framework document published this year (see www.18weeks.nhs.uk/public/default.aspx?load=ArticleViewer&ArticleId=449). The nurse provides emergency clinics, a telephone helpline, direction of the new rheumatoid arthritis patient group and monitoring of RA patients on biologic agents. The appendix outlines the cost implications of withdrawing the post; even without a mechanism to charge for telephone consultations there would be a net loss of income from withdrawal of the post, as the consultants would have to abandon new patient clinics to provide the intensive follow-up care required. This is further addressed in proposals for change at the end of this paper. Service Review: Dept of rheumatology, Queen Mary's Sidcup NHS Trust 3 The other AHP departmental members are not directly funded under rheumatology but are recharged as an overhead in the Trading Account, as are the HCAs. We are exploring the charging system for the Back Pain Triage service. Secretarial cover was previously provided by 2 secretaries who worked solely in rheumatology. This has been changed, and they now have to cover neurology in addition and the typing support time is now completely inadequate. The current arrangements are entirely unsatisfactory; the secretaries are diverted from rheumatology care and as a result communication with local GPs and patients is suffering. In the context of the drugs used in rheumatology this is creating a serious clinical risk. The potential problems were identified before the introduction of the new system (Appendix 3), but the views of the clinicians were overruled. We continue to monitor the situation carefully but as it appears that some secretarial redeployment has led to underutilisation we believe that the original status quo should be restored, not least because the neurologists are largely off site and the secretaries are therefore carrying an unreasonable clinical responsibility in an unfamiliar area. Departmental achievements Runner-up, “Hospital Doctor” Rheumatology Team of the Year, 2005 Catriona Howse (RSN) is one of 20 national Healthcare Champions chosen by the National Rheumatoid Arthritis Society (NRAS) for 2006. Dr Bamji is President of the British Society for Rheumatology (2006-8), is a Regional Advisor for NRAS and a member of Council of RCP (London). He has judged the HD competition this year and lectures nationwide on rheumatology topics in particular relation to service delivery The department has an unrivalled digital image bank for teaching The Back Pain Triage service and the departmental website are included on the ARMA website as examples of good practice Throughput The unit has one of the highest throughputs of patients per doctor in the UK (see Table 1). Inpatients are minimal. Day case drug administration (infliximab) is performed on the Elmstead Unit. The Musculoskeletal Framework underpins the need for a secondary care rheumatology service for the management of inflammatory arthritis (IA) Current Payment by Results tariffs are £230 for a new patient, £90 for a follow-up. High cost drugs are excluded. Service Review: Dept of rheumatology, Queen Mary's Sidcup NHS Trust 4 Table 1. Departmental statistics 2000-2001 Dr Bamji Dr Cheung Attended Cancelled Cancelled by patient by hospital DNA 685 87 9 0 Follow-up 2214 400 70 0 Total 2899 487 79 0 New 764 108 26 0 Follow-up 1061 192 24 0 Total 1825 300 50 0 New 656 71 12 0 Follow-up 2490 244 64 0 Total 3146 315 76 0 New 2001-2002 Dr Bamji Dr Cheung 734 97 21 0 Follow-up 1161 145 39 0 Total 1895 242 60 0 New 584 70 20 1 Follow-up 2662 285 73 37 Total 3246 355 93 38 New 2002-2003 Dr Bamji Dr Cheung 734 91 5 3 Follow-up 1226 155 25 5 Total 1960 246 30 8 New 2003-2004 Dr Bamji Dr Cheung 522 48 5 4 Follow-up 2695 252 75 20 Total 3217 300 80 24 New 722 103 12 14 Follow-up 1311 165 41 16 Total 2033 268 53 30 New 2004-2005 Dr Bamji Dr Cheung 543 35 14 0 Follow-up 2836 279 69 32 Total 3379 314 83 32 New 777 58 11 6 Follow-up 1260 177 55 10 Total 2037 235 66 16 New 497 45 10 2 Follow-up 1833 198 38 11 Total 2330 243 48 13 New 478 35 12 3 792 117 17 1 1270 152 29 4 New 1/424/11/2005 Dr Bamji Dr Cheung Follow-up Total Casemix Service Review: Dept of rheumatology, Queen Mary's Sidcup NHS Trust 5 A large proportion of new patients have non-inflammatory musculoskeletal problems which can be dealt with on a “one-stop” basis. Of the first 123 patients analysed since June 2006, 67 were not offered a further appointment. Of those that were, 23 had newly diagnosed inflammatory joint disease or were transfers from other units with inflammatory arthritis. The remainder required assessment of the results of treatment. Thus we have a robust approach to discharging patients and given the pressure on clinics we are not keen to hold on to patients unnecessarily. However in response to a request from the PCT we have agreed an approach to reducing follow-up numbers (see Appendix 4). Follow-up patients are predominantly suffering from inflammatory joint disease. They may need frequent monitoring in the early stages to stabilise treatment and require at a minimum a yearly review (ARMA Standards of Care). Dr Bamji currently has 589 RA patients and 411 other IA patients on the books. Of 141 “other” patients, 42 have PMR and 5 have GCA – which in many units are counted as non-RA IA 164 patients in total are on biologic agents. The cost implications are outlined below. The department runs spreadsheets for patient listing and currently uses a commercial program, RheDAS, for monitoring RA patients Monitoring Shared-care monitoring is not formalised and many local practices, particularly those from outside Bexley, are unhappy to monitor if they are not prescribing. All Biologics monitoring and submissions of data to BSRBR are coordinated by the RSN Website The URL is www.sidcuprheum.org.uk. The Introduction is taken from the site. We established the site to improve communication in the then absence of a hospital site. The site is being submitted as an innovation in the Health and Social Care Awards round, 2006. It provides a wealth of information for patients, GPs and specialists and is highly regarded. It also provides an alternative contact portal. Costs The department has a small budget which is largely in balance. We understand that this review was requested because the deficit showing in the first 2 months of the financial year 2006-7 was in the order of £140,000. The rheumatology nurse post was initially funded from a grant but on the understanding that funding would be taken over by the Trust after the first year. The overall cost is less than expected because the postholder has chosen to work part-time, but as outlined above the loss of revenue consequent upon disestablishment of the post outweighs any savings, so it makes no economic sense. Furthermore my presidency of the British Society Service Review: Dept of rheumatology, Queen Mary's Sidcup NHS Trust 6 for Rheumatology was conditional on the establishment of the post, and its removal would break a verbal undertaking from the previous Chief Executive and Medical Director which I was given in February 2005. MRI costs are above budget. In the financial year 2005-6 the “overspend” against notional allocation was in the order of £16,000. Analysis of this showed that a substantial proportion were shoulder and back scans. The former cannot be reduced on clinical grounds (although offering open access to GPs, clinically suspect as this is, may transfer this cost). Shoulder scans could be reduced by making orthopaedic referrals without scans, but this would burden that department with unnecessary referrals (often a scan identifies a problem that will require medical rather than surgical intervention) and would transfer any spend to that department. The inadequacy of the allocation represents a failure in our view to uprate with changes in clinical practice. The use of ultrasound is being discussed; however this requires a capital outlay for a machine, though it would undoubtedly produce a revenue saving on MRI and has major advantages in the investigation and monitoring of small joint and other soft tissue problems such as carpal tunnel syndrome – thus additionally saving on electromyography.. Pathology costs are generally low. Use of anti-CCP testing may enable us to target treatment more effectively. The hospital does not have a DEXA scanner. This is because a detailed analysis undertaken some 10 years ago indicated that the convenience of local scanning was outweighed by the capital and revenue consequences of maintaining and running the machine. As there is no waiting list of consequence at neighbouring sites (QE and Guy’s) the cost per scan using these units is significantly lower than providing an in-house service. However, changes in screening policy may make it cost-effective to provide scanning that accrues GP income. High cost drugs Biologics cost £10,000 per year per patient. These are currently licensed for rheumatoid arthritis and psoriatic arthritis; we await a decision on ankylosing spondylitis, but the clinical effects are little short of amazing in the small eligible group we have commenced. We have 165 patients currently on biologics. A breakdown by PCT will follow. We are thus spending over £1.5m on them The available drugs are etanercept (Enbrel), infliximab (Remicade) and adalimumab (Humira) – they are collectively known as TNF-α blockers. More recently a B-cell depletion drug, rituximab, has been licensed for TNF-α failures; the cost per cycle is approximately half that of a year’s TNF-α blockade, but holds the prospect of inducing remission after 2-3 courses. Further research evidence is awaited. Analysis of invoices suggests that over 90% of the 2006 overspend is attributable to this expenditure alone and our advice from the Accounts department confirms this. The problem is twofold – a failure to recharge to host PCTs and an inadequate allocation from Bexley (or both). Bromley, Greenwich and Kent agree patients on a cost per case basis and so all invoices should automatically be paid when presented. However the total allocation for NICE approved high cost drugs from Bexley CT is simply insufficient. They claim a statutory duty to stay within budget, but Service Review: Dept of rheumatology, Queen Mary's Sidcup NHS Trust 7 we have a statutory duty to provide NICE-approved drugs. In this context it should be noted that the Bexley CT HSS return shows that they claim compliance with section 5a (the section covering this) – but in view of the current problems this is untrue, and I have notified the Department of Health of this. In my capacity as President, British Society for Rheumatology I have also been invited to discuss matters of moment with the Healthcare Commission, who have specifically asked to cover problems on NICE HTAs, so I will be notifying them of our local problem as well as the many others around the country. The impact of biologic drugs could be reduced by the introduction of subcutaneous methotrexate. Use of oral MTX is limited by its absorption and the development of side-effects. S/C administration allows higher doses without concomitant higher toxicity. MTX failure is a precondition for biologics administration; thus, enabling more effective use of MTX may delay or avoid the need for biologic agents. S/C MTX costs, on home delivery, about £75 monthly compared to £710 for a biologic agent. There is resistance from the Pharmacy on this; further discussions will be held later in the year. Problems The unit is struggling to cope with the pressures of cuts. Continuing threats to staff posts have caused damage morale-wise. That said we believe that we provide an excellent service, and this is underpinned by the comments of patients, relatives and GPs – indeed we attract a substantial number of referrals from all the surrounding PCTs. Compared to other units we are grossly underprovided with specialist nurses and as noted are short on consultants. We have some support from a rehabilitation SpR but problems in the rotation have led to long gaps, and this is anyway a supernumerary post. Pressures on us to reduce follow-ups have been unreasonable, but this issue is being addressed; however, hard data on reduction will not be available for at least 6 months. Proposals Restructure of the Choose & Book clinics to reflect GP and patient need, and bring the Back Pain Triage service into the system as a rheumatology assessment clinic. (Note: this will be delayed as the national keyword/clinic type lists have been modified without consultation with the British Society for Rheumatology and are now inappropriate and incorrect) The Specialist Nurse post must be agreed as a permanent post. Its costs are outweighed by the income it brings in; it is essential for monitoring and audit as required by specialist standards of care; and without it the withdrawal of biologic drugs from patients who are not responding will be delayed Service Review: Dept of rheumatology, Queen Mary's Sidcup NHS Trust 8 The secretarial service must be restored to its previous level to avoid delays in communication and thereby patient risk. We do not feel that our clinical concerns at the time of re-organisation were taken sufficiently seriously, and regret that our fears have been entirely justified. This impacts on neurology as well as on rheumatology. The secretaries are under enormous and unacceptable pressure, while other secretaries appear under-employed. We propose that the neurology secretary post be re-established immediately and the work returned to its previous (excellent) incumbent. A managed reduction of follow-up patients is possible but limited by the needs to provide a high quality service as recommended in professional standards of care. We may be able to reduce some RA follow-ups from 6 months to one year if stable; however it is possible that this will generate additional urgent appointments. Removing some other groups (such as chronic pain patients) may result in rapid rereferral. We believe, given the pressure on our clinics, that we should be allowed to manage this process without interference; it is in our own interests to reduce our follow-up burden but clinical need is paramount. Introduction of S/C MTX is a priority and will save money – if two patients yearly are deferred by one year then the overall saving is about £18,000. Recharging for biologics must be tightened up. Negotiations are urgently needed over the high-cost drug allocation from Bexley CT, which is woefully inadequate and will accordingly lead to rationing and/or breach of our statutory duty to provide the drugs for eligible patients. Sorting this out will solve the financial issues Anti-CCP antibody testing was agreed in a business case at the end of 2005 and has not yet been introduced. This is a priority and may enable advance screening for disease severity – thus targeting therapy more effectively. Consideration should be given to a financial analysis of provision of a DEXA scanner to be sited in the Erith Hospital X-ray department A business case for musculoskeletal ultrasound should be developed to enable savings on MRI and electromyography The Musculoskeletal Framework requires the development of a CATS (Clinical Treatment and Assessment Centre). We believe this is best provided by a triage service comprising rheumatology (including our GP(SI)), orthopaedics and physiotherapy. Any other proposal will cause chaos with Choose & Book and will duplicate work at unnecessary expense. I am concerned that continuing threats to the department’s staffing will cause medical and medicolegal risks or result in unfavourable or unwelcome publicity. It is well recognised that the patient lobby in chronic diseases is both vocal and influential and has already Service Review: Dept of rheumatology, Queen Mary's Sidcup NHS Trust 9 intervened locally; this has resulted in pressure from patient groups and MPs, press reports and culminated in a visit from the All-Party parliamentary group for Rheumatoid Arthritis. I hope that this document indicates our understanding of the problems facing us and the willingness to explore innovative solutions, but clinical integrity and avoidance of risk remain paramount If the hospital configuration remains the same, then these proposals will suffice. However, if the development of an on-site ISTC and proposals for changing the configuration of acute hospitals lead to the withdrawal of A&E then I propose that serious consideration be given to a network arrangement for musculoskeletal services using Queen Mary's as a hub for both outpatient and inpatient work as well as diagnostic facilities, and drawing in the appropriate departments from the QE and Princess Royal. Another possibility would be to adopt the Stoke model where musculoskeletal outpatient (and this includes rheumatology inpatient and day case work) are moved, managerially, into the PCT. I will be pleased to appear before the Board to discuss this document. Dr Andrew Bamji FRCP 18th September 2006 Service Review: Dept of rheumatology, Queen Mary's Sidcup NHS Trust 10 Appendix 1 Queen Mary's Sidcup rheumatology department: Submission for “Hospital Doctor” Team of the Year The Hospital and the Department Queen Mary's Hospital Sidcup serves a base population of 215,000 and provides a rheumatology service to four PCT areas – Bexley, Greenwich, Bromley and Dartford – a total catchment population of about 260,000. It does so with a consultant base that is well below the recommended level of 1:85,000, with 1.75 whole time equivalent sessions. The population is mixed, with a relatively small number of ethnic minority patients. The Department is based within the therapies area of the hospital and has its own dedicated consulting rooms which double as offices. This offers the opportunity of immediate liaison with the therapists; furthermore the waiting area is shared additionally with the orthopaedic clinics. Thus all the staff can consult rapidly and informally with each other. In addition the team do clinics at the cottage hospital 6 miles away in Erith. The Department deals with all rheumatology problems (including children) and has a large follow-up population of patients with inflammatory joint disease. Where possible a “one-stop” service is provided for new patients. 127 patients are currently on TNF- blockade. Services are almost exclusively provided on an outpatient basis. New patient clinic appointments are prioritised by the consultants. Concordance with the half-hour waiting time in outpatients is over 95% in all clinics. The team Until the last two years the rheumatology service was entirely consultantbased but in that time a competent and compact multidisciplinary team has been developed. Its philosophy is simple – to provide timely and appropriate care for the whole range of musculoskeletal conditions. It now comprises Dr Andrew Bamji (Lead Clinician) – Consultant in rheumatology (7.5 sessions) and rehabilitation (2.5 sessions) and Director, Elmstead Rehabilitation Unit Appointed 1983 and full-time at Sidcup from 1987. President-Elect of the British Society for Rheumatology and Curator of the hospital archives; previous Associate Medical Director and Clinical Tutor Service Review: Dept of rheumatology, Queen Mary's Sidcup NHS Trust 11 Dr Nap Cheung – Consultant in rheumatology (full-time) Appointed 1999. College Tutor 2005-. Joint Hand Clinic with Mr G. Mani (orthopaedics) Dr Shanti Mendonça – GP with Special Interest Appointed 2002 Dr Bijay Sinha – SpR in rehabilitation medicine On rotation with Medway Maritime Hospital (to July 2005) Catriona Howse – Rheumatology Nurse Specialist Appointed 2004; previous experience as a renal medicine Specialist Nurse Elaine Willett – Physiotherapy Specialist Practitioner Appointed 2001. Co-ordinator of the Back Pain triage service Chris Boyles – Extended Scope physiotherapist (Knee Pain) Appointed 2004 Sara Glassberg – Occupational Therapist (Hand specialist) – Locum Appointed 2005 Stuart Rickman – Occupational therapy Technician Appointed 1988 Karen Brickenden – Secretary Appointed 2001. Hospital Audit Co-ordinator 1992-2000 Wendy Dyke – Secretary Appointed 2000 The department works closely with the Orthopaedic service and has direct access to specialists in knee replacement, shoulder problems, hand and foot surgery as well as to general services. It is supported by an excellent radiology department with ultrasound, spiral CT and MRI (routine waiting time about 8 weeks) and by an efficient Appliance Department. There are also close working relationships with the Pain service. The department runs several databases but these are self-developed due to lack of funding. Service Review: Dept of rheumatology, Queen Mary's Sidcup NHS Trust 12 Special services The department provides the following special services Helpline (intended for rheumatoid arthritis patients and carers, to provide support and advice relating to any aspects of their disease) Information service. A number of patient information leaflets are locally produced (for example on osteoporosis, diet and methotrexate treatment). Several protocols for use by generalists are on the hospital’s intranet database, including a management algorithm for the acute hot joint Specialist Biologics Clinics. These have been established to provide relevant information for patients prior to starting treatment, so that they are able to make a fully informed choice about their Anti-TNF treatment. They also ensure that patients are monitored for any adverse events, and long term efficacy. Nurse-led follow-up Clinics provide: support and education to newly diagnosed RA patients long term follow up, with the aim of empowering patients with information about their disease, thus enabling them to take responsibility for their own health care needs. Innovations Emergency Access slots (for A&E referrals, flare-ups, acute hot joints, diagnostic appointments; appointments can usually be made within 24 hours of request). Patients for whom emergency appointments may be needed are issued with an information sheet giving weekday contact numbers. Patients may be seen outside clinic times. The system provides timely expert treatment but in particular is key to the diagnosis of intermittent problems – such as crystal synovitis or palindromic rheumatism – in which acute episodes may have settled before a standard appointment can be obtained. Indeed the service provides quicker access to care than is available in general practice. Back pain service. This triage service ensures that all patients with back pain are assessed within two weeks and are triaged to physiotherapy, rheumatology or the Pain Clinic. It was established in 2001 and was initially developed to control the waiting list for the Pain Clinic, which had reached 18 months. The orthopaedic surgeons at Sidcup do not perform back surgery and so no back pain referrals now go to that department. Development of the service was undertaken in liaison with local GPs and resulted in major reductions in waiting times for routine rheumatology outpatient appointments (from an average of 21 weeks to 10 weeks) as well as a significant drop in the routine orthopaedic clinic waiting time. Referral is by protocol on a form which enables “red flag” signs to be identified and the triage team liaise closely with Service Review: Dept of rheumatology, Queen Mary's Sidcup NHS Trust 13 the rheumatology consultants in difficult cases. The triage physiotherapists can order MRI scans. Figures for the triage service are appended below. Prior to start-up about 40% of referrals came to physiotherapy, 30% to rheumatology, 20% to orthopaedics, with the remaining 10% to the Pain Clinic; many of these latter three would be referred back for physiotherapy. Thus over 200 “unnecessary” referrals per year to rheumatology have been avoided yearly. Knee pain service. This new service, commenced in 2005, is designed to reduce the numbers of non-surgical knee consultations within the Orthopaedic department, but sits more naturally in management terms within the rheumatology department and so has been subsumed. Chris Boyles, the ESP, performs joint injections, can make direct referrals for MRI scans and can add patients directly to surgical waiting lists. In addition he is training the A&E nursing staff in back pain triage Hand service. Apart from the Combined clinic (see above) the OT department offer a responsive care and splinting programme with a particular focus on rheumatoid arthritis. Extended roles. Our secretaries have an excellent reputation for patient liaison and their success in this culminated in the award of hospital “Team of the Month” to the outpatient secretaries in March 2005. Special treatments Intensive lobbying on a local basis has ensured that the department has no problems with the administration or supply of TNF- blockade, either in rheumatoid arthritis or in ankylosing spondylitis or psoriatic arthritis (see figures appended). Viscosupplementation injections are also performed; this is not confined to the knee but includes injection of shoulders, ankles and elbows. In particular, elbow injection in secondary osteoarthritis of the elbow following RA can be highly successful in relieving symptoms. Dr Cheung performs epidural injections for discogenic pain and sciatica Research Dr Cheung is a participant in a number of multicentre clinical trials Audit The Back Pain Triage service undertakes a rolling audit of workload and last year assessed outcomes. Catriona Howse has commenced an audit of TNF- Service Review: Dept of rheumatology, Queen Mary's Sidcup NHS Trust 14 patients. The department participates in the sub-regional rheumatology audit group. Management and budget The multidisciplinary team has a monthly meeting to discuss problems, strategy and finance What is special about the Queen Mary's department We excel in providing patient focussed service that is readily accessible, comprehensive, friendly and flexible. Seamless teamwork by the team ensures a quality and responsiveness that is an exemplar for the Trust. The department’s workload is heavy but waiting times for new appointments are low. Follow-up appointments are flexible; some patients only attend yearly, or less frequently, but all have the opportunity to arrange an early appointment directly with the department. We take special pride in the management of acute inflammatory disease activity with our emergency access service; this is vital to avoid both diagnostic delays, and the inappropriate attendance of our patients either in orthopaedic clinics or in the A&E department. The Back Pain Triage service is a particular example of successful multidisciplinary working which has not only streamlined the management of rheumatology patients (and reduced waiting times accordingly) but removed a large tranche of unnecessary referrals from the orthopaedic surgeons. All this adds up to a service that meets the needs of the users whilst also operating in an effective and efficient way. Acknowledgement to Schering-Plough (start-up money for specialist nurse post) 2002 Wyeth (grant for database development) 2004 Butterfly Appeal (Mayor’s fund – for computer/educational equipment) 2005 Service Review: Dept of rheumatology, Queen Mary's Sidcup NHS Trust 15 Appendix 1.1 Department statistics Total patients with rheumatoid arthritis in long-term follow-up: 927 Disease breakdown of follow-up patients (%): RA 55 Seronegative arthritis (inc reactive arthritis, spondarthritis, psoriatic arthritis) 21 SLE and other connective tissue disease 10 PMR/GCA 5 Osteoarthritis 5 JIA 1 Crystal arthropathy 1 Chronic pain 1 Osteoporosis 1 TNF- patients: Total 127; approximately half from outside Bexley PCT RA 109 AS 13 Psoriatic arthritis 4 Other 1 Service Review: Dept of rheumatology, Queen Mary's Sidcup NHS Trust 16 Back pain triage statistics Sept 20012 2002-3 2003-4 2004- May 2005 835 1023 1406 1016 Physiotherapy 75.9 75.2 76 84.5 Orthopaedics 4.8 0 0 0 Rheumatology 8.1 8.1 6.5 2.9 Pain Clinic 4.2 2.2 5.7 4.0 Returned to GP* 5.9 14.3 10.8 8.2 Total referrals Triaged to (%) *Proforma not appended to referral, or incomplete Rheumatology Helpline This service was established at Queen Mary’s Hospital in December 2004 to provide patients with greater access to advice and information about their condition, medication, and reduce the number of emergency telephone calls and appointments with the Consultant Rheumatologists or secretaries. The helpline was also established to provide information and advice to general practitioners, and district and practice nurses. The service has resulted in: Patients being provided with additional advice and information between appointments. Patients and carers being provided with an additional support resource between appointments. Provision of a screening service by a qualified health care professional for patients requesting emergency appointments to prevent inappropriate use of resources. Reduction of the number of telephone calls from patients dealt with by Consultants and the departmental secretaries. Nature of patients and callers using helpline Helpline calls were made for a variety of reasons, principally: Service Review: Dept of rheumatology, Queen Mary's Sidcup NHS Trust 17 Medication query Medication side-effect Blood test query General exacerbation of disease Exacerbation of disease – specific joint involvement Request for emergency or earlier Outpatient appointment Requesting outpatient appointment Requesting change of outpatient appointment (Note: the helpline is now taking nearly 200 calls monthly. We are looking at how these may be converted into face-to-face appointments) Appendix 2: Business case for rheumatology specialist nurse post This post has been operational since November 2004. Its establishment followed advice from a Departmental Peer Review (see attached appendix 1) and a visit from the All-Party Parliamentary Group on rheumatoid arthritis, both of which emphasized the need for the post. At the time of establishment Queen Mary’s was the only local hospital without such a post. Start-up funding was available following a substantial grant from ScheringPlough pharmaceuticals, who provided approximately £19,000 towards the first year’s salary. There was subsequent agreement with Trust management that the post would remain funded as part of the requirement to provide the necessary infrastructure for administration of biologic agents. The Department, having established the post, was successful in being nominated for the “Hospital Doctor” rheumatology Team of the Year Award in 2005, and was runner-up in the category; the other shortlisted departments were Southampton and King’s College Hospital, both large teaching centres. This achievement underpinned the transformation of a small department unable to fully manage biologics to one which is recognized nationally as a centre of excellence. It should also be pointed out that the number of consultant sessions is well short of recommendation of the Royal College of Physicians and the British Society for Rheumatology (BSR); we have 1.75wte compared to an expected level of 2.5. The nurse post goes a considerable way to meeting the shortfall and as a result of the establishment of the post we have put on hold our outstanding request for additional consultant sessions. The importance of rheumatology specialist nurses is outlined in the Standards of Care document produced by the Arthritis and Musculoskeletal Alliance (ARMA). Many of the information functions now expected by government are covered by the post but, most importantly, NICE guidance on the administration of biologic agents places a statutory duty on funding both of the drugs and of the necessary infrastructure for doing this. Thus it is expected Service Review: Dept of rheumatology, Queen Mary's Sidcup NHS Trust 18 that the costs and personnel needed to manage registration and monitoring are met. This was underlined by a letter to me, in my capacity as a member of the External Relations Committee of the British Society for Rheumatology, from the Department of Health which gave specific direction on the issue (see appendix 2). Regardless of national directives there is also a local issue. Dr Bamji is the next President of the British Society for Rheumatology. He discussed the implications of this to his own Job Plan with the Medical Director before agreeing to do it (in January 2005), indicating that it was only possible to proceed on the basis that the department had a specialist nurse in post. There has been no subsequent discussion indicating that there would be any problem with maintaining the post. It should also be noted that the RCP recommendations on consultant workload are for 4-5 clinics weekly (for a full-time equivalent) with either 6 new or 12 follow-ups per clinic. Dr Bamji (who is only 0.75wte in rheumatology) does 4-6 rheumatology clinics, and occasionally 7 weekly notwithstanding his outside commitments, with 8-12 new or 17-25 follow-up patients on each. This is grossly in excess of the recommended numbers and is only sustainable because of the specialist nurse support. Workload of the post The specialist nurse now manages all patients on biologic agents. She runs her own clinics for monitoring and for acute disease flares. She also operates the Department’s Helpline and is setting up the monitoring database (RheDAS) for RA patients. Work on this was commenced at the beginning of March 2006. The numbers of patients seen are substantial; 190 patients were seen in the nurse clinics in the last 3 months (this includes TNF monitoring patients, other RA patients and emergency consultations). Implications of withdrawal /failure to fund Problem Failure to meet NICE guidelines on prescribing and monitoring of biologic agents Loss of rheumatology helpline Implication Postcode prescribing which is unacceptable to the DoH and government; without the nurse our capacity to mange new start-ups in a timely fashion is zero. Two separate government ministers have stated that there should be no impediment to patients who are eligible for treatment; thus any patients who fulfil NICE criteria for the prescription of biologic agents but who cannot receive them due to funding issues will be told to contact their Members of Parliament. Ongoing monitoring requires a clinician. The Helpline has taken 172 calls from Service Review: Dept of rheumatology, Queen Mary's Sidcup NHS Trust 19 January 2006 to date. See Table 2 for the breakdown. Without it there will be increased pressure on the Department’s secretaries, and further pressure on urgent consultant appointments. Failure to set up database Loss of audit capacity Loss of coordination for patient information and education Increased pressure on consultant follow-up clinics The helpline is an essential part of any rheumatology department and is a recommended service both in BSR guidelines and in the “Consultant Physicians Working with Patients” guidelines from the Royal College of Physicians (in which there is a specific recommendation that a senior nurse specialist runs it.). Failure to meet NICE guidelines on monitoring. Failure to monitor serially in a timely fashion resulting in patients staying on biologic agents for longer than is appropriate. At present the specialist nurse is conducting an ongoing audit of biologic agents. This includes patients with conditions other than RA and patients started on etanercept for whom there is no longer a requirement to enter data on the BSR Biologics Register. This function would be unsupportable at consultant level due to pressure of work. A first Study Day for RA patients has been arranged under the auspices on the National Rheumatoid Arthritis Society in line with government aspirations for patient education and the development of an Expert Patient network. This and any future days will be lost. Most are already full. Adding back those patients currently under review by the specialist nurse will have a catastrophic effect on new patient throughput, as the only way to manage inflammatory joint disease will be to cancel new patient clinics. This runs counter to the Trust’s wish (and need) to attract more new patients into the system to maintain income. The loss of one new clinic a week (8-12 patients per consultant) produces a substantial income loss Service Review: Dept of rheumatology, Queen Mary's Sidcup NHS Trust 20 which is greater than the cost of the nurse post. As noted above the nurse uses the new database to do serial assessments and judge treatment failure; if patients return to ad hoc consultant clinics this will necessarily be assessed less often, and so unnecessary drug expenditure will be incurred. See Table 1. The DoH has made it clear that it will condone job losses where clinical services are not affected. By implication it will not agree damaging cuts to clinical services. Removal of the rheumatology specialist nurse is unquestionably damaging to patient care and safety If patients are not being properly monitored, and if GPs have to be told that their access to new patient slots is being curtailed, it will generate significant adverse publicity for the Trust. “Patient power” may also generate negative publicity in the local press. That is a high-risk strategy, as it may encourage a belief that the hospital is unsustainable. Political repercussions Local implications Table 1: Capacity of nurse-led clinic Monday AM Tuesday AM Tuesday PM QMS Weekly Capacity 10 10 10 4 Week Capacity 40 40 20 Tuesday PM EDH 8 8 Wednesday AM Thursday AM 6 6 24 12 Comments Alternate Weeks Alternate Weeks Alternate Weeks Total 40 80 100 108 132 144 Service Review: Dept of rheumatology, Queen Mary's Sidcup NHS Trust 21 Table 2: Rheumatology helpline calls Rheumatology Helpline Calls Dec 1st 2004 - March 29th 2006 80 70 60 Number of 50 Calls Per 40 Month 30 20 10 0 75 70 55 35 38 55 41 37 18 21 Feb 28 Oct Dec 13 3 Dec 26 Apr Jun 0 0 Aug Feb Month Funding The bottom line is that we are expected, indeed required, to meet NICE guidelines for the prescribing of biologic agents and this is impossible without specialist nurse input. The cost of the nurse post should be met from the overall cost of biologic agents. In comparison to the total cost and given the costs of failure to monitor (Table 3 below shows the breakdown) the nurse post effectively pays for itself. Number Of Patients Anti - TNF Patients March 2006 N = 156 120 100 80 60 40 20 0 97 24 Etanercept Infliximab 23 Adalimumab 7 5 Rituximab Suspended Drug Type Furthermore the loss of the post has a direct impact on costs. The Payment by Results tariff has been re-published. This indicates that a new patient will be chargeable at £219 and a follow-up at £97 (adults). On the assumption that the nurse specialist workload would have to be subsumed by the consultants a total of 760 consultant appointments would be lost annually (source: nurse specialist clinic figures for November 2005 - February 2006). Given the follow-up burden this could only be achieved by losing new patient slots; clinics are currently full on the follow-up side and indeed overbooked. This would mean a loss of new patient income of £92,720 annually. Service Review: Dept of rheumatology, Queen Mary's Sidcup NHS Trust 22 From a financial viewpoint, given that we are trying to increase income, this is ridiculous – and indeed such a sum would pay for three specialist nurses. Thus there are two ways forward for agreeing continued funding for the post. The cost of lost income leaves the Trust with a sensible fall-back position of continuing to fund the post on the basis that its continuation costs one-third of the potential lost income from its disestablishment. The Care Trust, which directly funds biologics and must continue to do so under PbR, be asked to allocate, on an ongoing basis, a specific sum from the biologics budget to cover the salary of the rheumatology specialist nurse, or it will effectively breach its statutory responsibility. Dr Andrew Bamji FRCP Clinical lead, Department of Rheumatology Queen Mary's Hospital, Sidcup, Kent DA14 6LT 28th March 2006 Appendix 2.1: Report of Peer Review visit 2001 BRITISH SOCIETY FOR RHEUMATOLOGY PEER REVIEW SCHEME REVIEW OF RHEUMATOLOGY UNIT AT QUEEN MARY’S HOSPITAL, SIDCUP 28th September, 2001 Reviewers: Professor DL Scott (King’s College Hospital, London) Dr J Wojtulewski (Eastbourne General Hospital, Eastbourne) SUMMARY AND RECOMMENDATIONS The rheumatology unit at Queen Mary’s Hospital, Sidcup is providing high quality clinical opinions on newly referred patients with rheumatic disorders. The service is organised by dedicated and highly motivated staff and operates in a pleasant and highly suitable environment. We have identified the following resource issues that need consideration by the Trust: There is no provision for the long-term management of patients with inflammatory arthritis. The most cost-effective method of providing this is to appoint a full-time rheumatology specialist nurse. This action is urgent and needs to be undertaken within the next 6 months. National recommendations from the British Society for Rheumatology are that each rheumatology unit should have one specialist nurse. There is insufficient medical secretarial input for the workload. National recommendations from the British Society for Rheumatology are that each full time consultant rheumatologist should have one full-time rheumatology secretary. We estimate the shortfall in medical secretaries is approximately 7 hours/week. This shortfall needs to be addressed in the next 12 months. Service Review: Dept of rheumatology, Queen Mary's Sidcup NHS Trust 23 There are too few consultant sessions in rheumatology for the population served by this Trust. Currently there are 18.5 consultant sessions for a population of 220,000; this represents one session per 12,000 population. National recommendations from the British Society for Rheumatology are for one consultant session per 8,500. This shortfall needs addressing in the longterm but it is not a matter of immediate concern. GENERAL INFORMATION Queen Mary’s Hospital Sidcup is a District General Hospital serving a population of 220,000. It has a busy acute medical service involving 10 consultant physicians. Two consultants provide rheumatology services and one of these consultants also provides rehabilitation services. RHEUMATOLOGY STAFF Consultants Dr A Bamji (Maximum part-time) 8.5 sessions rheumatology and 1.5 sessions rehabilitation Dr N Cheung (Maximum part-time) 10 sessions rheumatology Medical Secretaries 2 posts 28 hours with Dr Bamji 25 hours with Dr Cheung Junior Staff None Specialist Nurses None Other Professionals Reasonable levels of support from physiotherapy/occupational therapy FACILITIES Clinics Dedicated rheumatology clinics that operate full time High quality facilities that are well designed for people with arthritis Day-Care No special facilities Access to space on rehabilitation unit Functionally adequate for current needs In-patients No special facilities Access to general medical beds Functionally adequate for current needs OUTPATIENT ACTIVITY Overview The unit provides high quality clinical opinions on patients referred for specialist advice. As the workload is relatively high for a unit with only 18.5 consultant sessions it is unsurprising that the wait for appointments slightly exceeds the 13 week NHS target. With an adjustment in the unit staffing levels this target should be met. It is unlikely that any other unit in the country provides higher quality specialist opinions on the assessment of new referrals. Service Review: Dept of rheumatology, Queen Mary's Sidcup NHS Trust 24 By contrast there is a significant problem with the long-term specialist follow up of patients with rheumatoid arthritis and other forms of inflammatory arthritis and connective tissue diseases. As the unit has no specialist nurse, no day care facilities and no dedicated in-patient beds the needs of these patients are being ignored. The consultant rheumatologists are fully aware of the extent of the problem, but cannot do more within their current resources. This matter needs urgent attention from the Trust. Data from NHS Statistics (http://www.doh.gov.uk/hospitalactivity/statistics) Year 1996/7 1997/8 1998/9 1999/2000 New 1241 1280 953 1064 Follow-up 3038 3273 2372 2720 Ratio 2.4 2.6 2.5 2.6 Waiting Times from NHS Statistics (http://www.doh.gov.uk/waitingtimes/) 2000/1 GP Referrals 293 335 First Quarter Second Quarter Third Quarter 306 Fourth Quarter 389 Waiting over 13 weeks 97 131 Percent Waiting Over 13 weeks 33% 39% 103 107 34% 28% Outpatient Clinics Clinics held each week Patients seen by consultant Average wait for new patient Wait for urgent new patients Average wait for follow-up patients Wait for urgent follow-up patients 12 100% 16 weeks 0-2 weeks 12 weeks 0-2 weeks Facilities for Clinics Present Appropriate clinic environment Good support from receptionists and health care assistants Access to pathology and imaging services Support from physiotherapy, occupational therapy and surgical Absent No specialist rheumatology nurse No system for monitoring DMARD therapy in rheumatoid arthritis Limited combined clinics with other specialists No junior staff Service Review: Dept of rheumatology, Queen Mary's Sidcup NHS Trust 25 appliances INPATIENT AND DAY CASE ACTIVITY Patients with acute medical problems can be admitted as and when the need arises. There are sufficient junior medical staff to meet this need, though the arrangements are not ideal. There is some access to day care facilities on the rehabilitation unit, but no dedicated day care access or support. OTHER ASPECTS OF UNIT Continuing Professional Development Consultants in the unit are involved with national and local schemes for education within rheumatology and are well informed on all aspects of the speciality. Audit The unit participates in local and regional audits. Research The unit is involved in regional research initiatives and would wish to increase its activity in this arena. Dr Cheung has considerable research expertise in rheumatoid arthritis. The unit should be attracting sufficient NHS R&D income to the Trust to fund at least part of a rheumatology nurse, though it is unclear that the Trust is actually claiming this income. Teaching The unit has little opportunity for undergraduate or postgraduate teaching and this is an area for potential development. National Activities Dr Bamji has taken a leading national role in setting standards and clinical affairs. He continues to hold responsibilities in these areas. Secretarial Support The unit has two dedicated medical secretaries, who work part-time (28 and 25 hours/week). The amount of secretarial work exceeds the time available and at least one of the secretaries is putting in additional hours on a voluntary basis to maintain a high quality service. Regional Context The changes in the NHS in the next 5 years, with the introduction of primary care trusts and the formation of new strategic health authorities for London, will change the context in which specialist rheumatology services are delivered. We do not believe that rheumatology services should be centralised, as they need to be delivered locally to meet the needs of people with arthritis. Nevertheless the interactions with other local Trusts could change in this new environment. Therefore recommendations about junior medical support and consultant staff should be deferred until more information is known about the general pattern of specialist services in South East London. Service Review: Dept of rheumatology, Queen Mary's Sidcup NHS Trust 26 Appendix 2.2: Letter from the Department of Health: 9th June 2004 Thank you for your recent email to Rosie Winterton about NHS funding for treatments recommended by National Institute for Clinical Excellence (NICE) appraisals. Due to her busy schedule Ms Winterton cannot respond to all of her correspondence personally, therefore I have been asked to reply. Having spoken to policy officials I can confirm that the costs for drugs are dependent on the specific appraisal, on the whole drugs are fairly cheap to administer and facilitate but if a drug has an administration cost then this will be factored into NHS funding. In conclusion, the answer is yes - the statutory obligation quoted covers both the drugs and the costs of the administration. I hope you find this reply helpful. Yours sincerely, Victoria Adams Customer Service Centre Department of Health Appendix 3: Outpatient secretary proposals March 2006: effects on rheumatology services Introduction A suggestion has been advanced as part of the Queen Mary's Hospital “Fit for Future” review that will reduce the complement of outpatient secretaries. The proposal is flawed in its reasoning and will potentially cause severe damage to rheumatology and rehabilitation patient care. It is regrettable that no-one involved in developing the proposal has at any time discussed it with the department’s consultants; no-one has sought the consultants’ views following publication of the proposal; and it appears that it is being treated as a “faitaccompli”. We believe that the proposal is unsustainable, is in breach of statutory guidelines for NICE-approved drugs, will cause delays in communication with primary care and is clinically unsafe. It also runs contrary to the spirit of developing multidisciplinary teams and the guidelines for a musculoskeletal service as laid down in the Standards of Care produced by the Arthritis and Musculoskeletal Alliance (ARMA). Background The Royal College of Physicians and British Society for Rheumatology have set guidelines for rheumatology secretarial staffing as 1 wte per consultant. Service Review: Dept of rheumatology, Queen Mary's Sidcup NHS Trust 27 In 2001, as part of an exercise to develop the management of TNF-α blocking drugs for rheumatoid arthritis, a Peer Review was conducted on the department. At that time there were only 2 consultants and a part-time SpR (4 sessions) in the department supported by part-time secretaries. The visiting team comprised Professor DL Scott from King’s College Hospital and Dr J Wotjulewski from Eastbourne. They concluded that the department ran a good service but was seriously hampered by inadequate backup staff. In particular they identified the need for a rheumatology specialist nurse and increased secretarial hours. By 2004 both of the issues had been addressed, with the establishment of a Nurse Specialist post and an increase in the hours of Dr Bamji’s secretary. These were agreed by management at the time as necessary developments to maintain a high quality, safe clinical service and fulfil College guidelines. The secretaries have been through an Agenda for Change review which established their posts on Band 4. It appears that the current proposal will have the effect of reversing these changes. Secretarial duties These are appropriate for a Band 4 post and include a large component of direct patient contact (dealing with urgent enquiries, booking urgent appointments, sorting out problems with drugs and test results). The secretaries also deal with GPs who may likewise request appointments to be made. The secretaries may receive up to 40-50 calls per day. To deal effectively with these requires them to know the patients – and this is best achieved by typing the correspondence. While on occasion work has been devolved to other secretaries this causes delays, and may indeed increase work if secretaries untrained in terminology and not “tuned-in” to the dictation styles of the consultants; work has to be edited and re-typed. The typing itself is a substantial work component. This is shown on the work breakdown constructed by the outpatient secretaries. Dr Bamji’s work alone, not including his two Erith clinics, encompasses four consultant, three SpR and three or four specialist nurse clinics. One is a rehabilitation clinic which is long because letters are necessarily very detailed (and often require multiple copies). This is simply not work that is appropriate for delegation to pool typists. Additional correspondence is generated in responding to results of tests. Thus the department’s work is not comparable to that of other medical specialties where the workload, clinic-wise, is not of the same order. Currently the workload is such that letters are delayed between dictation and typing for up to 10 days. Any delay is unacceptable – and where drugs doses, or types, are changed there is potential clinical risk. Dr Bamji has been on two visits to local practices as part of the “Partnership project” to encourage GPs to use Queen Mary's rather than an alternative. In each case the issue of availability and communication was raised – if consultants cannot be contacted, or if correspondence is delayed in transmission, then GPs will (and do) look elsewhere for their services. Certain departments – and the Service Review: Dept of rheumatology, Queen Mary's Sidcup NHS Trust 28 rheumatology department was among these – are deemed excellent, communication-wise. It is only thus because there is adequate secretarial support. To cut the secretarial time dedicated to the department will have a significant effect on future GP referrals and on potential income. To suggest that their posts can be subdivided into different bands is nothing short of insulting and is probably contractually illegal. Given this analysis it is all the more unfortunate that no-one involved in the review had sought out the consultants to ask them what effect the proposed changes might have. It has apparently been argued that it is not the secretaries’ remit to deal with appointment booking. However, the consultants must be asked regarding the timing and appropriateness of moving or booking urgent appointments and only the secretary is in a position to do this. Some appointment enquiries, whether patient or GP initiated, require immediate action. Failure to act appropriately will potentially expose patients to risk, and the hospital to allegations of negligence. It is unreasonable to suggest that such a function can be undertaken on a part-time basis if it would lead to messages being delayed by 24-48 hours. However such delays would be inevitable if their “PA” function is reduced to half-time. Our service only functions properly because we have sufficient dedicated support and patients will be put at risk if that support is diminished. NICE-approved drugs The role of the department’s nurse specialist has been outlined in a separate submission – but underpinning the role of both the nurse and the secretaries is the need to follow national guidelines. This is a statutory requirement and extends to the infrastructure necessary to manage both new patients and follow-ups – a requirement underlined in a memorandum from the Department to Dr Bamji dated 9th June 2004 which reads: Thank you for your recent email to Rosie Winterton about NHS funding for treatments recommended by National Institute for Clinical Excellence (NICE) appraisals. Due to her busy schedule Ms Winterton cannot respond to all of her correspondence personally, therefore I have been asked to reply. Having spoken to policy officials I can confirm that the costs for drugs are dependent on the specific appraisal, on the whole drugs are fairly cheap to administer and facilitate but if a drug has an administration cost then this will be factored into NHS funding. In conclusion, the answer is yes - the statutory obligation quoted covers both the drugs and the costs of the administration. I hope you find this reply helpful. Yours sincerely, Victoria Adams Customer Service Centre Department of Health This statement is unequivocal. As a result the Trust has a statutory obligation to comply. The secretaries play a pivotal role in the management of RA Service Review: Dept of rheumatology, Queen Mary's Sidcup NHS Trust 29 patients on TNF-α blockers. They book and rearrange appointments for infusions and help to communicate data collected by the specialist nurse to the British Society for Rheumatology’s national Register. They also communicate with GPs. As this class of drugs cannot be used in general practice there can be no escape from the need to have sufficient secretarial time to manage this – and we emphasis that the commitment in 2001, when our Peer Review pointed up the shortfalls, was only to some 30 patients. Now the department manages over 150. Given these changes it seems entirely inappropriate to cut hours which are required for a statutory responsibility that has increased five-fold since they were agreed. Other issues Dr Bamji shortly assumes the role of President of the British Society for Rheumatology. This is a national post (unpaid) for which, like the officebearers of Colleges, it has been traditional for Trusts to release post-holders without prejudice. Prior to offering himself as a candidate in January 2005 he had discussions with Liz Roberts, Medical Director, on the implications of taking up the post, and entered the election on the basis that staffing in the department was now adequate, and that the time commitments needed for the post of president would not therefore place extra strains on the department, its staff and patient care. Summary The rheumatology consultants fully support the Fit for Future process and accept that it is important to match income with expenditure. However it has been emphasised both locally and nationally that any cuts made as the result of trying to eliminate financial deficits will not jeopardise clinical services. The combined effect of local proposals to reduce secretarial hours, and remove the department’s specialist nurse, will do more than jeopardise our service – they will make it impossible to run. We are happy to enter negotiations for alternative measures that might secure financial savings. However, as we have at no time been party to any financial analysis of our service other than by receipt of the budget statements, and as we have not been consulted about the present proposals, we are unable to co-operate with them. We believe that they have been based on numerous misconceptions as to the work of the secretaries in our specialty. We have no doubt that the proposals will expose us, and the hospital, to significant risk; that they will effectively be a cut in clinical services and that they will threaten our ability to meet statutory national guidelines for NICE-approved drugs. Dr Andrew Bamji FRCP Dr Nap Cheung MD FRCP 26th March 2006 Service Review: Dept of rheumatology, Queen Mary's Sidcup NHS Trust 30 Appendix 4: Reducing rheumatology follow-ups: Analysis of the problem June 2006 Introduction The rheumatology department at Queen Mary’s has an excellent reputation for good and sensitive patient care. It has been recognised as such by its success as runner-up in the “Hospital Doctor” Rheumatology team of the Year awards. The hospital’s management of back pain is considered a model of good clinical practice. It has its own website for patients and GPs. The senior consultant, Dr Bamji, has been involved over many years in the development of care guidelines for the British Society for Rheumatology and the Royal College of Physicians, and is currently President of the former and on the Council of the latter. It is suggested that rheumatology follow-up appointments should be reduced so that Bexley Care Trust expenditure might be reduced. There are clear limits to the possibilities. Firstly it must be accepted that long-term diseases require long-term specialist input. Inflammatory joint disease can be managed at arms length if patients are stable, but the Arthritis and Musculoskeletal Alliance (ARMA) guidelines for managing rheumatoid arthritis (RA) – which have been endorsed by the Department of Health – require patients to be reviewed at least annually. Thus the potential to discharge long-term followup patients is limited. Both consultants already tailor follow-up intervals to clinical need. Secondly there are patients who “bounce”. They are happily managed in secondary care with long appointment intervals but if an attempt is made to discharge them they are re-referred. Sometimes they will be referred to other departments, and then get re-investigated at considerable cost. It should be agreed that such patients are managed both more cheaply and more effectively by continued long-term follow-up. Thirdly there are issues of patient safety. Thus patients with polymyalgia rheumatica (PMR) are managed inconsistently and sometimes badly in general practice. Fourthly, a significant number of follow-ups are emergency appointments for patients with disease flares, acutely swollen joints etc. The reason that patients request early or urgent appointments is a reflection of their trust in the secondary care service and their understanding that the problem cannot be dealt with in a timely fashion in primary care. We need to recognize this and that patient choice is reflected by sensible provision. There is no advantage in financial terms to discharging patients who then require re-referral, as this generates a significant cost differential (£230 for a rheumatology new patient to £90 for a follow-up) and will be time-consuming and time-wasting for GPs. Worse, the Choose & Book system will result in patients reappearing on another consultant’s list. This is not conducive to patient satisfaction or continuity of care. Service Review: Dept of rheumatology, Queen Mary's Sidcup NHS Trust 31 Finally it should be pointed out that the Department’s working figures on ratios contain a typographical error and cannot be relied on to give an accurate nationwide picture. The scope of the problem We have been requested to remove about 950 follow-up attendances from the clinic, which has a lost revenue implication of £86,500 per year to the Trust. In 2005-6 Dr Bamji saw 2214 follow-up patients and Dr Cheung saw 1061. Thus Dr Bamji would need to see 641 less follow-up patients in a year. Given two weeks study leave and 6 weeks holiday this equates to a total of 15 per week – three-quarters of a current follow-up clinic. This is neither possible nor safe. The scope of the solution The calculations below are based on Dr Bamji’s follow-up database. This comprises all patients who have not been discharged from clinic. Patients are not entered onto the database unless they have had more than one follow-up appointment. The data is not entirely complete. Patients who are seen in the specialist nurse clinic (in particular those on biologic agents) are entered onto a separate database; thus, the dates that the patients were last seen may be incorrect. However there is a certain drop-out rate of patients expected for review who have defaulted long term. Dr Bamji’s practice is broadly similar to that of Dr Cheung so the figures may be extrapolated. RA patients Total 575 Attended in last 2 years 561 Review @ ≤ 2 months 53 Review @ 9-18 weeks 151 Review @ 6 months 238* Review @ ≥ 9 months 133 (mainly once yearly, as per ARMA guidelines) First seen range September 1983 – April 2006 Average time to next 24 weeks appt Total patients seen 335 (some seen more than once) 2006 Pts on biologic agents 98 * patients seen less often than 6 monthly are unstable Seronegative arthritis, lupus and other connective tissue disease patients Total Attended in last 2 years Review @ ≤ 2 months Review @ 9-18 weeks Review @ 6 months 391 377 47 108 128 Service Review: Dept of rheumatology, Queen Mary's Sidcup NHS Trust 32 Review @ ≥ 9 months First seen range Average time to next appt Total patients seen 2006 Pts on biologic agents 108 (mainly once yearly) 24 weeks 198 28 We do not believe that any of these patients can be safely discharged entirely, not least because of the issues of guideline review. There is also a substantial number of patients whose drug monitoring would necessarily have to be done in general practice and it is certainly very doubtful that all GPs would be prepared to take this on. If one was to prolong 6 monthly follow-up patients to 1 year, that would save 360 appointments. Previous experience has shown, though, that prolonging follow-up intervals beyond that which patients find comfortable results in an increased number of requests for emergency appointments. Thus, while there may be some scope for reduction in numbers, it is probably only half this, and patients would be unhappy with any arbitrary decision. Neither do the data allow us to identify the number of patients who have had appointments brought forward on an emergency basis but it is in the region of 5-10 patients per week. In specific reference to the nurse-led clinics the patients are either on biologics monitoring or are emergencies. Thus the scope for reducing numbers in this clinic is nil. This leaves the miscellaneous largely non-inflammatory conditions, OA, PMR, gout, osteoporosis etc. There are only 151 of these, of whom only 62 have been seen in 2006. The breakdown by condition is shown below: of particular note is that there are no patients with mechanical low back pain who are being followed up. Condition Osteoarthritis PMR Chronic pain Gout Giant-cell arteritis Osteoporosis Other No on database 60 45 13 8 7 4 14 Appointments saved by discharge 81 137 N/A (see text above) 9 N/A 0 The calculations are made by using the interval to next follow-up and extrapolating yearly (thus discharging patients on 26 week reviews would save 2 appointments). The reason the figures are so small is that analysis of the interval to next appointment against the date last seen indicates that a number of patients have anyway defaulted from follow-up. Chronic pain patients on Dr Bamji’s list are only there because experience (as mentioned above) proves that discharge results in rapid re-referral; if a patient has a safety net appointment they are more likely to hold on until it is due. A number of OA patients (19) are on the regular books for viscosupplementation or other injections. These are unlikely to be taken back into primary care. Nevertheless about 190 follow-up appointments might be saved but, because Service Review: Dept of rheumatology, Queen Mary's Sidcup NHS Trust 33 of the patient expectation referred to above, some will drift back by requesting re-referral. PMR discharge will require the development of a protocol of management of steroid dose. This should be based on the PRODIGY guidelines available through NLH (http://www.prodigy.nhs.uk/pmr_and_gca/view_whole_guidance. Again, experience indicates that GP management is patchy and we have seen more than one patient treated with inappropriately high doses of steroids for relapses of symptoms that were something else – resulting in admissions and a major expenditure on rescue management. This underpins the need to examine carefully not only the savings of early discharge, but the cost of rereferral and mismanagement. We believe the risks, and potential medicolegal costs, are substantial. We estimate that 30% of our patients are from outside the Bexley Care Trust area; they are from Greenwich, Bromley and Dartford with a smaller number from further afield (Lewisham, Tunbridge Wells, Canterbury/Ashford). This underlines our reputation as a good unit and that patients choose to be referred to Queen Mary’s. We have not been asked to make any reductions in follow-up of these patients. Thus we would be developing a system of “postcode follow-up” which would be manifestly unfair. In numbers terms, though, the figures given above would have to be reduced by 30% to reflect the impact on Bexley Care Trust. Summary These figures thus show that the maximum safe reduction in follow-up appointments, based on robust data and allowing for out-of-district patients, is small. Of discharged patients a number will return because of failure of primary care management. The number of saved appointments is so small is because of the very rigorous follow-up policy already in place; the preponderance of inflammatory joint disease patients in follow-up clinics; and the requirements for ongoing specialist management laid out in Department of Health endorsed guidelines. With clinics that are overbooked almost without exception there is every incentive for the consultants to discharge patients – and they already do so when it is clinically appropriate. On that basis it would be unacceptable on grounds of patient safety, the following of guidelines and clinical decision-making, to reduce appointment numbers just for the sake of doing so. A further analysis of outpatient work in rheumatology can be found in the references below. These underline the proactive approach of the Department at Sidcup to careful analysis of workload and clinic provision; the first shows (and this has been confirmed by more recent studies) that 80-90% of new patients have non-inflammatory disease but the ratio is reversed for follow-up clinics. Interestingly there is variation in numbers of patients seen, and their diagnoses; thus in the Middlesbrough department PMR was rarely referred. This may reflect different GP experience and knowledge. Some recent work from Bristol (Kirwan et al) has proposed a model of discharge with emergency-only follow-up. This however is out of line with current guidelines and its safety is disputed within the specialty – indeed the practice has not been widely adopted. Service Review: Dept of rheumatology, Queen Mary's Sidcup NHS Trust 34 Dr Andrew Bamji Dr Nap Cheung Consultant Rheumatologists Queen Mary’s Hospital, Sidcup Dr Shanti Mendonça GP with Special Interest 18th June 2006 References Bamji AN, Dieppe PA, Haslock I, Shipley ME. What do Rheumatologists do? A Pilot Audit Study. Br J Rheumatol 1990, 24, 295-8 Bamji AN. Waiting times and referrals (Editorial). Rheumatology 2000; 39: 349-352 Kirwan JR, Mitchell K, Hewlett S, M. Hehir M, Pollock J, Memel D, Bennett B. Clinical and psychological outcome from a randomized controlled trial of patient-initiated direct-access hospital follow-up for rheumatoid arthritis extended to 4 years. Rheumatology 2003; 42: 422 – 426 (Note: Since this paper was submitted it has become apparent that classifying PMR/GCA as non-inflammatory is outdated and that there may be significant risks from failure to monitor in secondary care) Service Review: Dept of rheumatology, Queen Mary's Sidcup NHS Trust 35