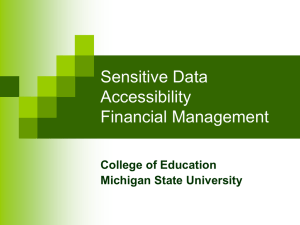
International Prostate Symptom Score (IPSS)
")
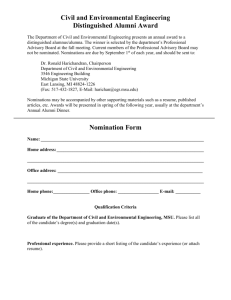
Provisional Diagnosis
Macro Haematuria
Micro Haematuria
Renal / Staghorn / Ureteric
Calculi
Elevated PSA / Prostate
Disease
Bladder Outlet
Obstruction/LUTS
Urethral Stricture
Incontinence
Renal Lesions / Cysts
Urinary Tract Infection
Testicular Tumour / Mass
Penile Ca+ /Penile
Discharge/Erectile
Dysfunction
Baseline Investigations (dated within 3 months of referral date)
MSU FOR M/C/S, CYTOLOGY X 3
ELFT’S, FBC, ESR
CT : NON-CON, CON & DELAYED EXCRETORY PHASE
< 50 NON-SMOKERS:
MSU FOR M/C/S, CYTOLOGY X 3
RENAL USS + KUB
ALL OTHERS:
MSU FOR M/C/S, CYTOLOGY X 3
ELFT’S
CT : NON-CON, CON, DELAYED EXCRETORY PHASE
MSU FOR M/C/S
ELFT’S, FBC, ESR
KUB + NON–CONTRAST CT
FOR URETERIC STONES - PLS REPEAT CT + KUB 2/52 AFTER
1 ST PRESENTATION OR 1/52 PRIOR TO OPA TO CONFIRM
STONE STILL PRESENT
MSU FOR M/C/S
PREVIOUS PSA RESULTS
ELFT’S, FBC
MEDICAL / SURGICAL HISTORY
FAMILY HISTORY
MSU FOR M/C/S
PSA, ELFT’S, FBC, ESR
RENAL USS WITH RESIDUAL
PHARMACOLOGICAL HISTORY
MSU FOR M/C/S
RENAL USS WITH RESIDUAL
PHARMACOLOGICAL HISTORY
SURGICAL / MEDICAL HISTORY
ASCENDING AND DESCENDING URETHROGRAM
MSU FOR M/C/S
ELFT’S, FBC, ESR
RESIDUAL VOLUMES (USS)
MEDICAL / SURGICAL / SOCIAL HISTORY
MSU FOR M/C/S
FBC, ELFT’S
RENAL USS
CYTOLOGY X 3
TRIPLE PHASE CT (IF SOLID LESION OR SUGGESTED BY USS)
MSU FOR M/C/S
PREVIOUS MSU RESULTS
RENAL TRACT USS WITH POST VOID RESIDUAL
PHARMACOLOGICAL HISTORY
MSU FOR M/C/S
ELFT’S, FBC, ESR
ALPHAFOETOPROTEIN (αfp)
USS TESTES, CXR
β
HCG, LDH
MEDICAL / FAMILY HISTORY
MSU FOR M/C/S, CYTOLOGY X 3
URETHRAL SWAB
SEXUAL HEALTH HISTORY
MEDICAL / SURGICAL HISTORY
* NOTE: CT IF CREATININE NORMAL. IF NOT USE RENAL USS AND KUB
Abbreviations:
βHCG – Beta (sub unit) Human Chorionic Gonadatropin
IVP – Intravenous Pyelogram
KUB
– X-ray of Kidneys, Ureters & Bladder
USS – Ultrasound
CON – Contrast
International Prostate Symptom Score (IPSS)
Questions to be answered
Not at all
Less than
1 time in 5
Less than half the time
About half the time
(Circle one number on each line)
1. Over the past month, how often have you had a sensation of not emptying your bladder completely after you finished urinating?
0 1 2 3
More than half the time
Almost always
4 5
3 4 5 2. Over the past month, how often have you had to urinate again less than
2 hours after you finished urinating?
3. Over the past month, how often have you found you stopped and started again several times when you urinated?
0
0
1
1
2
2
4. Over the past month, how often have you found it difficult to postpone urination?
5. Over the past month, how often have you had a weak urinary stream?
6. Over the past month, how often have you had to push or strain to begin urination?
0
0
0
1
1
1
2
2
2
7. Over the past month, how many times did you most typically get up to urinate from the time you went to bed at night until the time you got up in the morning?
0
(none)
1 (1 time)
2 (2 times)
Sum of circled numbers (symptom score): _______
0 to 7: Mild symptoms
8 to 19: Moderate symptoms
20 to 35: Severe symptoms
3
3
3
3
3 (3 times)
4
4
4
4
4 (4 times)
5
5
5
5
5 (5 or more times)
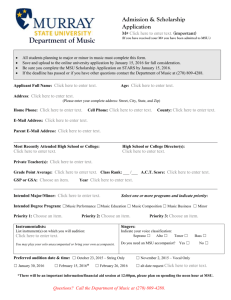
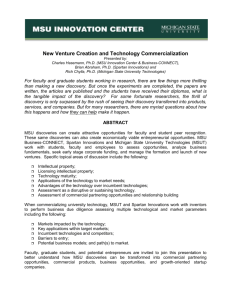
PRINCESS ALEXANDRA HOSPITAL
TIME / VOLUME BLADDER CHART
PATIENT IDENTIFICATION
Name:
Address:
DOB:
DAY 1 Date: / / DAY 2 Date: / / DAY 3 Date: / /
TIME
Fluid
Intake
Type of
Fluids
Volume of Urine
Passed
Leakage
Fluid
Intake
Type of
Fluids
Volume of Urine
Passed
Leakage
Fluid
Intake
Type of
Fluids
Volume of Urine
Passed
Leakage
6 am
7 am
8 am
9 am
10 am
11 am
12 nn
1 pm
2 pm
3 pm
4 pm
5 pm
6 pm
7 pm
8 pm
9 pm
10 pm
11 pm
12 mn
1 am
2 am
3 am
4 am
5 am
TOTAL
LEAKAGE column coding: D (damp), S (soaked) or CC (needed to change clothing); SZ (sneezing), L (laughing), C (coughing), ST (straining), SU (standing up).