CC4C Workgroup Best Practices for Reducing Non
advertisement

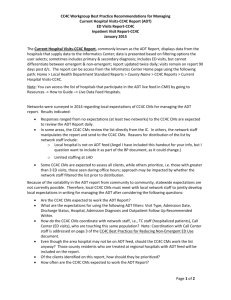
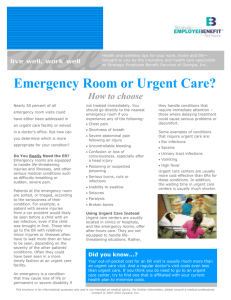
CC4C Best Practices for Reducing Non-Emergent ED Use by Focusing on Local Systems of Care & Improving the Quality of the Touch January 2015 Applicable CC4C Guidance Found in CC4C Tool Kit: CC4C WG BP Recommendations Priority Population Report Sept 2014 CMIS Step-by-Step for CC4C Care Management Developing Local Systems of Care that Work: CCNC networks have learned that non-emergent emergency department (ED) utilization is a tough measure to impact, but a critically important Key Performance Indicator (KPI) in terms of inappropriate utilization and cost. From a data perspective, lessons learned include: It is possible to wrap care management services around children who frequently use the ED for non-emergent care and impact both the quality of care these children receive (in a medical home) as well as the cost of their care. However, to truly impact the overall rate of ED utilization, there must also be systems level approaches that complement these individual efforts. In focusing on systems-level strategies, it is important for CCNC networks & LHD CC4C staff to work together on an integrated, collaborative approach. The beginning point is to know your community. If you are uncertain about the answers to the following questions, some of your CCNC or CC4C CM colleagues who are linked or embedded in the practices may be a resource: What are the 24/7 after-hours coverage policies for the practices that serve your children? Which practices have open access scheduling or some system for accommodating same day appointments? What call centers are being used to handle after hours calls and what kind of guidance are they providing with respect to ED use? Where are the urgent care centers in your community? Which urgent care centers operate as an outpatient clinic as opposed to urgent care centers that are owned by a hospital? Urgent care centers that operate as an outpatient clinic are paid a lower rate of reimbursement. What are their hours of operation? What ages are served by the urgent care center (e.g. young children; older children; adults)? Do they accept Medicaid & how do they handle the prior approval requirement? Are communities physicians/pediatricians comfortable with urgent care centers treating infants and young children (birth to 2 years old)? And, if yes, to the previous question, are urgent care centers comfortable receiving these referrals? As part of a continuous quality improvement process, it will be important for network & LHD staff to consider the factors in their local communities that create barriers to reducing non-emergent ED use and then develop strategies to successfully intervene. Some common challenges and potential opportunities are presented on pages 5-7 of this document. As an option in your CQI effort, consider collaborating with your network QI team to map how your ED is currently being utilized and then map how this could be improved in the future. Be creative! For example, are Behavioral-Mental Health clients in crisis being routinely referred to the ED? Are there more appropriate and skilled resources available in the community that could become the primary referral source? From a “systems perspective”, what are the opportunities to improve quality of care and impact cost? Page 1 of 7 CC4C Best Practices for Reducing Non-Emergent ED Use by Focusing on Local Systems of Care & Improving the Quality of the Touch January 2015 Choosing the Best Informatics Center Lists to Impact ED Utilization: The Current Hospital Visits –CC4C (also called the ADT List) is available from the Informatics Center and provides timely information about ED utilization. It displays data from the hospitals that supply data to the Informatics Center. The number of hospitals participating is increasing steadily. Note: You can access the list of hospitals that participate in the ADT live feed in CMIS by going to Resources -> How to Guide –> Live Data Feed Hospitals. ADT data is presented based on the filtering options the user selects. The report is updated twice daily & visits remain on the report for 90 days post discharge. Some networks, whose hospitals are not sending data to the IC, are able to access data that provides ADT-type information directly from the hospitals. It is important to appreciate that the Current Hospital Visit (ADT) Report does not differentiate between emergent and non-emergent visits. To do this type of sort requires ICD-9 Diagnosis Codes that are only available from claims data. The ADT includes Admission Date/Time and Discharge Date/Time which helps in evaluating access to other services at the time of the ED visit. Current CCNC and TC Priority List-CC4C (also known as the Priority Population Report) is updated monthly and contains information on all Medicaid-Enrolled patients. Data columns included in this report are color coded to indicate current information (GREEN column headers) versus data from the July 2013 S1 Chronic Care report (BLUE column headers). CCNC and Transitional Care priority indicators have been updated to incorporate Care Triage(TM) Risk Score information that predicts a patients risk for admission within the next 12-months. The Report Details indicate the service dates of claims data used to indicate the number of ED visits, which could be used to prioritize CCNC Priority patients with multiply ED visits. A third report, the ED Visit Report – CC4C displays ED Visits for all Medicaid-eligible children based on the filtering options you select. This report has the option to pull in up to 15 months of ED claims history. As stated in the ED Report Details: “This report is based on ED visit claims with the most recent processed/paid claim as of mm/dd/yyyy (recent visits may not appear).” Claims typically pay with a 3 month delay “on average”. A filter can be applied to distinguish emergent from nonemergent ED use. This report can be used to identify chronic over-utilizers of the ED by the # of times that they have utilized the ED over the time period being reviewed. For example, a “Top 25” /ED Utilizer List (for CC4C or for individual practices) can be created to focus attention on those that are utilizing the ED most often. In this report, the Date of Service / Day of the Week is presented, but not the Time of Day which is no longer received in claims data. All three of the above reports are available from the Informatics Center (IC Home Page -> Local Health Department Standard Reports -> County Name -> CC4C Reports -> Choose name of report desired from above list). Review the “Report Details” for each report so that you understand the way each report is generated and what patients it does or does not include. Filtering the Lists: Collaborate with your CC4C Network Lead to determine the best approach to filtering the lists for your area. That will assure that the filtering is applied based on local realities: urban vs. rural; how the care managers choose to assign work (by practice; geographic area; etc.); how CCNC & CC4C have chosen to collaborate to reduce non-emergent ED use; and the regional differences in the way EDs are marketed & utilized. Page 2 of 7 CC4C Best Practices for Reducing Non-Emergent ED Use by Focusing on Local Systems of Care & Improving the Quality of the Touch January 2015 Quality of the Touch at the Individual Family Level: Before deciding to call a child’s family re: their ED use, check FIRST to see if the CCNC Call Center has recently contacted this family. Check Patient Demographic Page under “Utilization” and “Call Center Support Calls”. By clicking on the number, you can review survey results in CMIS. If they have called and no new activity has been reported since that date, then you can document your “Claims Review” +/or “Case Review/Chart Audit” Task(s), update the CC4C Case Status to show your evaluation of this patient and move on. If the CCNC Call Center staff feel that active CM is indicated based on their family contact, they will make a referral to their CCNC contact who re-distributes referrals to the appropriate CCNC, CC4C, OB CM or HCC. Some survey responses trigger automatic referrals. Once you decide to contact the family, follow the principles of engagement as outlined beginning on page 3 of the CC4C WG BP Recommendations Priority Population Report Sept 2014. Avoid a deferral for “Unable to Contact” until you have documented at least 3-5 unsuccessful attempts at different times/ different days/different ways using diverse strategies as noted in CC4C CM Standardized Plan & the above-mentioned PPL Best Practice document. Initially focus on the child and the child’s well being, not the ED visit. Gently explore their reasons for choosing the ED over their child’s medical home. (Sample questions below). Were doctors at the ED able to help your child? Did they give you discharge instructions? Were you given a prescription? Were you able to fill the prescription? Is child taking it? Did the ED ask you to follow-up with your PCP (or specialist)? If yes, were you able to follow-up? Based on the parent’s goals, teach self-management of disease, side effects, and red flags, as appropriate. Provide education about how to handle red flags. SW care managers may need to collaborate with a nurse care manager depending on the child’s medical needs. (Some of the patient education resources listed below may be helpful). Use MI skills to set future goals re: ED use. Assess understanding of their doctor’s 24/7 coverage policies including availability of after-hours care (as applicable). Empower families to ask questions & seek answers they need to care for their child. Educate family on benefits of the Medical Home as the ONE place where the staff knows the child and the child’s health history. It is where their child can receive the comprehensive and coordinated quality of care they deserve. Encourage use of Urgent Care rather than ED if access to their child’s medical home is not available. Consider providing a list of nearby urgent care centers if after hours medical home access is a concern. Remember: Visits to outpatient (rather than hospital-owned) urgent care centers are reimbursed at a lower rate. Explain appropriate use of the ED for true emergencies, e.g. bleeding that won’t stop; severe breathing difficulties; after a serious accident; and for poisoning (after calling Poison Control at 1800-222-1222). Ideally, the patient should be followed in Heavy or Medium Case Status until the education is complete and the family’s needs are met. Then defer as soon as appropriate so that you can engage new patients for services. As always, document your work. Treat any child you identify for follow-up from lists as a new referral. It is important to be able to demonstrate the number of patients you are touching and/or attempting to touch and the intensity of your involvement. Refer to CC4C CMIS Step-byStep and CC4C WG BP Recommendations Priority Population Report Sept 2014for more detailed information re: CMIS documentation. Page 3 of 7 CC4C Best Practices for Reducing Non-Emergent ED Use by Focusing on Local Systems of Care & Improving the Quality of the Touch January 2015 Challenges to Reducing the Rate of Non-Emergent ED Visits and Opportunities to Address the Challenges Most Important! Engage with Your Network QI Staff and CC4C Network Leads in Considering Challenges & Opportunities at the Systems Level for Impacting ED Rates Systems level impacts may help you work smarter, not harder. This section provides a menu of “systems-level opportunities” to choose from. Perhaps there is one strategy that you feel would have a big impact on the population of children you serve. CCNC QI staff work with practices & other community providers on QMAF Measures and Quality Improvement Initiatives. ED utilization is one focus of their work. Ask if and how you can help support their efforts. Marketing of EDs by Hospitals The Challenge: Hospitals have been marketing their EDs through use of billboards & other media by promoting short waiting times, easy access, incentives for coming to the ED, creating appealing waiting room environments, and recommending that patients schedule recheck appointments at the ED. The Opportunities: Employ social marketing strategies to promote the importance of a quality medical home for children. Determine if an OB/CC4C Transitional CM is employed at your community hospital, and if not, consider hiring and embedding one to monitor utilization & make referrals. Determine if ED Navigators are employed, and if not consider using them to redirect patients with non-emergent conditions to more appropriate and less expensive venues of care. By talking with the patients after a Non-Emergent ED Visit, the ED Navigator can intervene at the most teachable moment, refer the family to a care manager for continued follow-up and schedule a recheck appointment or well child visit (as appropriate) with the child’s medical home. Hospitals have been urged by the President of the NC Hospital Association to improve their collaboration with CCNC in a joint effort to reduce NC’s Medicaid expenditures including ED utilization. Request an update on how these efforts are going in your region. Ask your CC4C Network Lead how you can support these efforts. Accessibility Issues The Challenge: Use of the ED for non-emergent care is appealing for many reasons: Services are available 24/7 without an appointment. This allows families to come when it is convenient for them (in relation to work schedules; availability of transportation; etc.). EDs are usually located along bus transit routes. Page 4 of 7 CC4C Best Practices for Reducing Non-Emergent ED Use by Focusing on Local Systems of Care & Improving the Quality of the Touch January 2015 EDs typically have interpreter services (e.g. for Spanish speakers & often for other languages depending on locale). Social issues that impact patient care and access to care also contribute to inappropriate utilization of resources (e.g. homelessness; behavioral health issues; lack of transportation; etc.) Some hospitals require that individuals be admitted to the hospital through their ED as a part of the admission process. In many areas, there are not enough “other options” when a child is sick at night. The Opportunities: Work as a team (HCCs, CCNC PCMs, CC4C/OB CMs and PCPs) to assure that the children you touch receive the best quality of care and access to care possible through their medical homes and help families understand that inappropriate use of the ED is a quality of care issue. Join forces with community partners and practices to help families understand that a child’s medical home is the ONE place where the staff knows the child and the child’s health history. It is where their child can receive the comprehensive and coordinated quality of care they deserve. In concert with the Network QI Team, find out why parents in your community are choosing to go to the ED. Share that information with the medical homes that serve your children as a part of a discussion about how to reduce inappropriate ED use. Emphasize that we are all in this together and need to work as a team on this issue. Work with CCNC to encourage and support practices in offering open access scheduling, 24/7 coverage and after-hours access. (See Primary Care Providers/Medical Home Practices Section below). For children being admitted to the hospital or sent to the ED by their PCP, Northwest Community Care set up a private cell phone line. That phone is carried by an ED staff member so that community physicians can call and let them know when a patient is on the way and for what reason. They also explain what labs/tests have been done and share results (to avoid duplicative tests and expenses). ED staff FAX back a summary of the visit. Urgent Care Issues The Challenge: Outpatient urgent care centers, which typically offer a similar service to the ED visit but at a lower cost, must get prior approval from the PCP before billing. This sometimes results in outpatient urgent care centers refusing to see Medicaid clients without a prior approval. Some hospital-owned urgent care centers bill these services as an ED visit at the same high rate of reimbursement. Even if a hospital owned urgent care center bills using the urgent care revenue code that is appropriate for their facility, the cost is only slightly lower than the ED rate of reimbursement to the hospital. In some counties EDs are more prevalent and conveniently located along bus lines. A parent may not choose to go to an outpatient urgent care center if they will pass an ED on the way there or if mass transit makes the ED more accessible. Some counties don’t have access to an outpatient urgent care center, so if the medical home doesn’t provide 24/7 coverage and/or after-hours care, then the ED may be the only option after-hours. Page 5 of 7 CC4C Best Practices for Reducing Non-Emergent ED Use by Focusing on Local Systems of Care & Improving the Quality of the Touch January 2015 In terms of the medical home quality of care/consistency of care social marketing message, recommending urgent care is counter to the thrust of that message. Check with providers regarding the best after-hours approach. If urgent care centers are used, encourage strong communication with medical homes. The Opportunities: From a practical standpoint, outpatient urgent care centers (those not sponsored by hospitals) are a less expensive option as compared to the ED (in the absence of other options). Primary Care Providers/Medical Home Practices The Challenge: Not all medical homes offer 24/7 coverage; some practices offer no after-hours number & patients are told to go to the ED if the office is closed. Not all medical homes offer open access scheduling or after-hours access. Sometimes the quality of the after-hours call service (triage) is a concern, especially if the call service does not respond to calls quickly and/or if the staff are not clinicians. Triage nurses advise and refer based on physician-approved protocols or algorithms. Some may refer to the ED for non-emergent issues. There is the potential for a conflict of interest if the after-hours phone triage system is sponsored by a hospital that markets their ED or builds multiple EDs throughout a county. Sometimes reception staff at the front desk and/or appointment staff see that the schedule is full & refer patients to the ED without the PCP or the embedded or linked CCNC or CC4C CM knowing that this is happening. The Opportunities: CCNC Network QI Staff works with practices on standards of care and QMAF (Quality Measurement & Feedback) Measures. CC4C staff should work collaboratively with CCNC Network QI Staff to support them (as appropriate) in relation to the following proposed practice-based activities: Care managers need to know the 24/7 coverage and after-hours access policies so that they can share this information with each practice’s patients. Discuss concerns regarding a practice’s 24/7 coverage & after-hours access with appropriate staff at the CCNC Network (CC4C Network Lead or QI/QMAF Staff). CC4C care managers may be able to identify practice patterns related to ED use either from patient report or data. Ask if front desk staff and folks responsible for scheduling appointments are aware of the practice’s policy with respect to 24/7 coverage & after-hours care. Encourage the practice to distribute that policy to all patients in writing or post the policy in a very prominent place in their waiting room. Encourage consistency with respect to the handling of same day appointments for children with acute care needs. Discuss the importance of not referring to the ED because an appointment is not available. Some embedded care managers tell patients to ask for them if they have trouble getting an appointment when child needs to be seen quickly. Ask if the practice has considered open-access scheduling. American Academy of Pediatrics, research suggests that open access scheduling improves continuity of care, increases patient and staff satisfaction, decreases appointment no-shows and improves practice financial Page 6 of 7 CC4C Best Practices for Reducing Non-Emergent ED Use by Focusing on Local Systems of Care & Improving the Quality of the Touch January 2015 viability. [AAP Link: http://www.aap.org/en-us/professional-resources/practicesupport/quality-improvement/Pages/Quality-Improvement-Open-Access-Scheduling.aspx] Collaborate with the practice on educational strategies/patient interventions to reduce inappropriate ED use. For example, the practice could consider proactively educating patients on how to manage the top 3 conditions that result in inappropriate ED use (fever, colds, ear infections) and discuss appropriate use of medical home vs. ED. Provide data to the Network QI staff & their practices to help them identify CC4C patients who are high utilizers of the ED (e.g. “Top 25 ED Over-Utilizers” can be flagged in their EHR or record). Help practices appreciate the costs associated with this misuse of the ED. Learn about your locally-used call center’s physician-approved protocols and/or algorithms that provide families with the information they need to appropriately manage non-emergent acute care issues. Are they directing patients to the ED when other interventions are possible? Advice may include guidance for what the parent can do to manage the acute illness at home; how to know when it is time to call the doctor based on the child’s symptoms and/or illness duration; and, if appropriate, advise families to see the PCP the next day & then fax a referral to the practice. Page 7 of 7