Topic Summary - Lewisham`s Joint Strategic Needs Assessment
advertisement

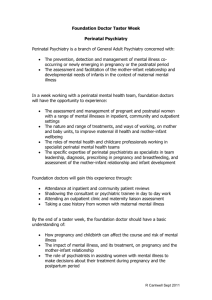
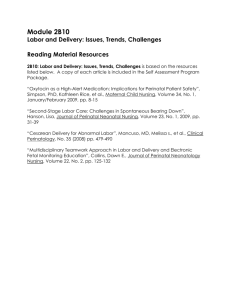
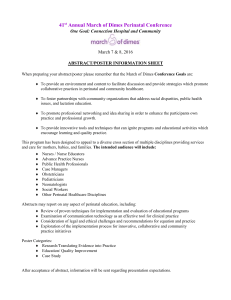
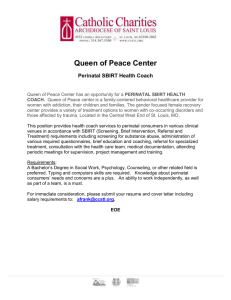
Antenatal and Postnatal Mental Health Services in Lewisham: A Health Care Needs Assessment Maternal mental health problems pose a huge human, social and economic burden to women, their infants, their families and society, and constitute a major public health challenge. This needs assessment explores the mental health needs of women during pregnancy and postnatally, and the services that are currently available to help them in Lewisham. Throughout the document related services will be referred to as perinatal mental health services as used by NICE. Purpose of the Needs Assessment To provide an overview of the epidemiology of perinatal mental illness in Lewisham and nationally. To review the evidence and recommendations for effective management of perinatal mental illness and quality care services. To identify current service provision. To identify gaps in current service and make recommendations for local planning and strategy formulation What do we know? Facts and Figures Lewisham is home to over 266,500 residents from a range of diverse communities, neighborhoods and localities and the local population is forecast to rise to over 290,000 over the next twenty years1. Children and young people (0-19 years) make up 25% of the population, whilst elderly residents (over 75) make up just 5%, with the average age of the population in Lewisham being 34.7 years, young compared to other London boroughs1. The most widely adopted measure of deprivation in England is the Index of Multiple Deprivation (IMD). Using this measure, Lewisham is the 31st most deprived Local Authority in England and relative to the rest of the country Lewisham’s deprivation is increasing. The highest deprivation is particularly found in Evelyn ward in the North and Downham in the South and along the A2 corridor. The map below shows how uneven the distribution of deprivation is across Lewisham. 1 Figure 1 The distribution of IMD 2010 in Lewisham by national quintile. Source: http://www.lewishamjsna.org.uk/health-inequalities/index-of-multiple-deprivation (accessed 04/05/2012) Perinatal mental illness covers a wide range of disorders, and affects one in six mothers during the antenatal and postnatal period2. The chronic illnesses that occur pre-pregnancy such as chronic depression, bipolar disorder and schizoaffective disorders can be exacerbated by pregnancy. There are also those disorders more specific to the antenatal and postnatal period such as antenatal depression and anxiety, postnatal depression and puerperal psychosis. The epidemiology quoted in this document comes from the NICE guidelines and the referenced studies from there. Further detail can be found by going directly to the NICE guidelines. Depression and anxiety are approximately twice as prevalent globally in women as in men, and are at their highest rates in the lifecycle during the childbearing years from puberty to menopause. Of the 2 perinatal mental illnesses, postnatal depression is the most common, with over 11% of mothers experiencing it during the postnatal period3. Depression and anxiety often occur together, making it difficult to find an accurate prevalence for anxiety, although studies have shown that up to 20% of women in the perinatal period can suffer from a combination of anxiety and depressive symptoms. Puerperal psychosis, the most severe of the perinatal disorders is relatively rare and occurs in 0.1-0.2% of postnatal women and approximately 4 women per 10,000 births will require admission to a specialist unit pre or postnatally for severe mental illness3. It has been estimated that 50% of people with depression, not just those in the perinatal period are not identified4. This means that only around half of the pregnant or postnatal women who develop depression may present to primary care mental health services each year. A similar or lower figure might reasonably be expected for anxiety disorders, with fewer disorders being identified than for depression. For the vast majority of these women, professional help will be provided solely by primary healthcare services. However, this is not always the case with around 3% to 5% of women giving birth having moderate or severe depression, and about 1.7% being referred to specialist mental health services5,6. Thus, around 17 women per 1,000 live births would be referred to specialist mental health services with depression postnatally. Again, it is reasonable to expect the figures for anxiety disorders to follow the national trend, with a lower rate of referral through to specialist services. Common mental health problems during the antenatal and postnatal period include depression and anxiety disorders, such as panic disorder, OCD and PTSD. An estimated 10% to 15% of women suffer from depression after the birth of an infant; in England and Wales this is between 64,000 and 94,000 women a year and is equivalent to between two and three women per year on the average GP list and 100 to 150 per 1,000 live births7,8. Prevalence data for anxiety disorders during the perinatal period are not as reliable. The Office for National Statistics estimates that the prevalence of anxiety is around 4% of men and 5% of women9. This would mean that around 30,000 women giving birth per year in England and Wales are also likely to be suffering from anxiety, with two or three women per year on the average GP list; 50 per 1,000 live births. First presentations of severe mental illness, primarily schizophrenia and bipolar disorder, in the perinatal period are rare, with a rate in the region of two per thousand resulting in hospital admissions10. These episodes are associated with a clustering of admissions in the first month after the birth; 1 per 2,000 live births. More common, particularly with bipolar disorder, is the exacerbation of an existing disorder, with some studies reporting relapse rates for bipolar 3 disorder approaching 50% in the antenatal period and 70% in the postnatal period11, 19. These women, along with others suffering from severe depression and other severe disorders such as severe anxiety disorders or personality disorders, will benefit from referral to specialist mental health services. Risk factors for perinatal mental illness include3, 17, 25: Recent migration Exposure to violence (domestic, sexual and gender-based) Emergency and conflict situations such as war and natural disasters Poor social support and being a single mother Past history of mood and anxiety disorders including postnatal depression (30% relapse rate with subsequent births) Family history of perinatal illness Childhood abuse Low income Unplanned pregnancy Large number of existing children Young age of the mother Traumatic delivery Perinatal death Live births in Lewisham residents have risen annually in the last few years, and the majority of the deliveries occur at University Hospital Lewisham. In 2010 there were 723,165 live births in the UK, and 4,982 to Lewisham women. Using the prevalence figures above, it can be estimated that in 2010 approximately 1000 mothers would have been affected by a perinatal mental illness, with 600 of these having symptoms diagnostic of postnatal depression. 85 women would have required referral to the Perinatal Mental Health team and approximately two women would have required admission to the mother and baby unit for treatment. Many of the risk factors listed above, including recent migration, poor social support, being a single mother, low income, young age of the mother and perinatal death, are more common in Lewisham than in England and Wales, therefore greater numbers of women may require care in Lewisham. This is particularly evident in that seven Lewisham women were admitted to a mother and baby unit between 2011 and 2012 as apposed to the predicted two, and between 2010 and 2011 there were 193 women from Lewisham referred to the specialist Perinatal Mental Health service as apposed to the predicted 85. 4 Figure 2 A chart to show the number of referrals to the Lewisham Perinatal Mental Health Team, and from where the referrals originated. Sample of Lewisham Referrals to Perinatal Outpatients Service April 2010-March 2011 Lewisham Social Services 4 Other 19 Lewisham Antenatal Clinic 80 GP 55 CMHT 22 KCH Antenatal 13 Consequences of Maternal Mental Illness The overall prevalence of mental disorders is similar in men and women. However, women’s mental health requires special consideration in view of women’s greater likelihood of suffering from depression and anxiety disorders and the impact of the mental health problems on childbearing and childrearing12. Many women with chronic mental illness stop taking their psychotropic medication when they become pregnant due to concerns about potential harm to the developing foetus, and this underlies the high rates of relapse in pregnancy. Women suffering from mental illness who become pregnant are at a high risk of obstetric complications with poorer outcomes for themselves and their babies13. It is therefore clear that women with mental health problems have specific obstetric treatment needs in addition to psychiatric treatment needs during the perinatal period, and this care should be delivered in a structured and cohesive manner. 5 During pregnancy, women with mental illness may be less likely to eat and sleep well, gain adequate weight, not attend antenatal care, fail to seek help for the birth, use harmful substances such as alcohol, cigarettes and drugs, and self harm or commit suicide12. In developed countries suicide causes 10% of maternal deaths in the year following delivery12. The Confidential Enquiry into Maternal Deaths (2001, 2004) showed that over half of the women who commit suicide after childbirth had a previous psychiatric history, but this risk factor was neither identified nor acted upon by involved health professionals14. Stress hormones are also raised during maternal mental illness and may have physical effects on the mother predisposing her to high blood pressure, preeclampsia and an early and difficult labour12. Babies may also be small for age. After the birth mothers may fail to eat, bathe or care for themselves, increasing the risk of infection and anaemia18. Mental illness can hamper the mother-infant attachment, breastfeeding and infant care, and mothers may be less likely to understand their babies cues for hunger, happiness or distress12,15. Studies have shown that infants of chronically depressed mothers show less sociability with strangers, fewer facial expressions, smile less, cry more and are more irritable than infants of well mothers23. Children do not perform as well on thinking and intelligence tests at 18 months, and they are more distractible, less playful and less social up to the age of 522. Effects on older children have been shown to include neglect, abuse, slower social, emotional and cognitive development and higher rates of school and behaviour problems12,21. There is also an increase in the disruption of the marriage and/or spousal abuse by either partner16,24. For women with a mental disorder during pregnancy and postnatally, the clinical context can be complicated by the needs of the foetus and infant, and by the women’s psychological adjustment to pregnancy, motherhood or having an additional child whilst experiencing mental illness. Services also need to take into account the needs of the father/partner, carers and other children in the family. National Guidelines The Royal College of Psychiatrists recommends that health professionals should advise women to talk about their feelings, get support with practical tasks from family and friends and to try and catch up on sleep and get time away from the baby26. 6 However, talking about and confronting the issue of mental illness during pregnancy or the postnatal period still poses challenges for healthcare professionals. Motherhood is loaded with emotive expectations, and not to conform to the idealised image of the ‘blissfully happy, blooming mother-to-be or new mother’ is widely regarded as a taboo. This contributes to a large number of perinatal mental illnesses going undiagnosed. 70-80% of women with perinatal mental disorders can be successfully treated and recover12. To a large extent the identification and management of most of these mental disorders can be done at a primary care level. One challenge faced by those involved in the care of these women is the wide range of services that women use at this time. This requires close communication between all the services. Poor communication has often been identified as the reason for poor quality of care. Current specialist provision for women with perinatal mental illness is patchy. Only approximately 25% of Primary Care Trusts have a fully developed and implemented policy for perinatal mental health26. Determining the need for specialist services, including perinatal teams and the number of inpatient facilities, their size and location is difficult. Firstly, the incidence of severe mental illness requiring inpatient care varies across the country, with much higher morbidity in the inner city areas compared with suburban or rural areas. Bed usage by Primary Care Trusts reveals a bed use approximately 1.7 times higher in urban than in rural areas, although this may not simply be the result of higher urban morbidity but due to women living in rural areas being reluctant to travel long distances to the nearest inpatient facility. The presence of crisis and home treatment teams may also impact significantly on the use of inpatient services27. NICE issued clinical guidance in 2007 about the treatment and management of women with perinatal mental illness. It recommends that healthcare professionals ask the Whooley questions at a women’s first contact with primary care, again at her booking visit, and again postnatally, at 4-6 weeks and again at 3-4 months28, 29, 30. These questions are: During the past month have you been bothered by feeling down, depressed or hopeless? During the past month, have you been bothered by little interest or pleasure in doing things? If yes to either question: 7 Is this something you feel you need or want help with? At a women’s first contact with services in both the antenatal and postnatal period, healthcare professionals should also ask questions about past or present severe mental illness, previous treatment by a psychiatrist/specialist mental health team and whether there is a family history of perinatal mental illness. These questions act as a screening tool to try and help identify those women that may be mentally unwell, or may become unwell during or after their pregnancy, which will then allow them to be properly monitored and managed. Studies have shown that continuity of midwifery care throughout the antenatal and early postnatal periods does not have an effect on depression symptoms, even in women with a history of depression. However, continuity in the postnatal period seemed to result in fewer women with depression at 7 weeks postnatally compared with standard care31, 32. According to guidelines, treatment options should depend on the severity of the illness, past psychiatric history, and maternal preference. Due to the possible risks associated with medication during pregnancy and breastfeeding, the threshold for use of psychological treatments is much lower. Women requiring psychological treatment should be seen within one month of initial assessment, and no longer than three months afterwards. Treatment options include3,33,34,35,36: Watchful waiting o For mild depression o For those patients already on antidepressants, they should be withdrawn gradually and monitored. Self-help such as computerised CBT (C-CBT) and exercise o For mild to moderate illness without a previous history of mental illness Interpersonal psychotherapy (IPT) and CBT o For mild illness with episodes of severe illness in the past o The time to response is longer than with medication o Useful in moderate to severe illness in conjunction with medication Psychotropic drugs o For moderate to severe illness o Mild illness with a past history of severe illness ECT o Severe or treatment resistant illness 8 Referral to perinatal psychiatric services o For recurring illness or bipolar disorder at the outset of pregnancy o Where there is a risk of suicide, self harm or self neglect o Where there are psychotic or manic features o Where there is a family history of severe depression, puerperal psychosis, suicide or bipolar illness NICE guidelines also state that clinical networks should be established for perinatal mental health services and these networks should provide: A specialist perinatal service in each locality, able to provide direct services, consultation and advice to maternity services, other mental health services and community services. In areas of high morbidity these services may be provided by separate specialist perinatal teams. Access to specialist advice on the risks and benefits of psychotropic medication during pregnancy and breastfeeding. It is important that women not only understand the risks involved in taking psychotropic medications during pregnancy and breastfeeding, but also the risks of an inadequately or untreated disorder. Clear referral and management to ensure effective transfer of information and continuity of care. Pathways of care for service users, with defined roles and competencies for all professional groups involved. Advantages of these clinical networks include the effective concentration of expertise and the identification of dedicated time and explicit responsibility for the delivery of appropriate care to mentally ill women and their families. This should then lead to a more favourable outcome in terms of reduced mortality and morbidity and increased patient satisfaction. The identification of clear pathways, a threshold for referrals and evidence-based protocols will support healthcare professionals in identifying and managing the most serious disorders. Clarity about treatment thresholds should also improve access to psychological therapies, which are seldom available quick enough. Postnatally, services must be able to respond rapidly to emerging illness and link effectively with obstetricians, midwives and health visitors expressing concern. Clinical networks can also play a key role in training, education and raising awareness. A model of a clinical network is set out below. It shows that women identified by general medical services such as maternity services or through their GP, as having a mental disorder can be referred directly to the part of the network that can give them the most appropriate care, or their GP can source appropriate 9 information and advice from colleagues in other parts of the network to provide adequate care themselves. Figure 2 A model of a perinatal clinical network Source: http://www.nmhdu.org.uk/silo/files/full-nice-guideline-on-antenatal-and-perinatalmental-health.pdf (accessed 10/05/2012) Each managed perinatal mental health network should also have designated specialist inpatient services and cover a population of between 25-50,000 live births per year depending on the local psychiatric morbidity rate20. Each specialist perinatal inpatient service should: Provide facilities specifically for mothers and infants 10 Be staffed by specialist perinatal mental health staff Be staffed to provide appropriate care for infants Have effective liaison with general medical and mental health services Have available the full range of therapeutic services Be closely integrated with community based mental services to ensure continuity of care on discharge and minimum length of stay Current activities and services in Lewisham Perinatal Mental Health Team Lewisham does currently have a small perinatal mental health team. It consists of one consultant who does one session per week, one full time perinatal psychiatric nurse, one specialist registrar who works for one day and does one clinic session per week, and one full time co-ordinator. Any health professional may refer a woman to the team. This is done by faxing a referral form to Kings College Hospital where it is signposted to the correct boroughs team. Currently any woman who is pregnant or within one year postpartum with moderate to severe mental illness, or a history of moderate to severe mental illness can be referred. If a woman is already under the care of the Community Mental Health Team the Perinatal Mental Health Team will provide advice but will not take over the care. Once a woman has been referred to the service she will either be seen in clinic, or a home visit can be organised by a member of the team. More and more of the patients are now seen at home, as the number of non-attendances at the Ladywell Unit was previously high. The team can organise referrals for psychological therapies if necessary, prescribe and monitor medication, and generally offer support for these vulnerable women. All these women will also have a detailed psychiatric plan in their maternity notes so when they are seen by the midwives, or admitted to the labour ward to deliver, the plan, and contact details for the team are readily available. The team works very closely with the midwifery caseload team, but a weekly joint clinic has been closed because of poor attendence. However, joint home visits do occur. The team also works very closely with GPs, health visitors and social services. Regular letters are sent to the women’s GPs to update them of their patients’ progress and are also sent to named caseworkers where relevant. Currently there is no 24 hour cover for perinatal mental health at Lewisham, and if an emergency develops and a patient needs to be seen urgently, then it falls to liaison psychiatry to review and manage the patient until a member of the 11 perinatal psychiatry team is back on site. This means that there are concerns amongst the obstetric teams that it can be very difficult to identify and contact a consultant psychiatrist when needed. Mother and Baby Unit Approximately four women per 10,000 births will require admission to a specialist unit pre or postnatally for severe mental illness. 75% of trusts do not currently have a specialist MBU or access to one, and 12% of trusts still admit mothers and babies to general psychiatric wards20, although this has never occurred within Lewisham. The most local Mother and Baby Unit to Lewisham is the unit at The Bethlem Royal Hospital in Beckenham, Kent. It is a thirteen bedded unit that accepts referrals from consultant psychiatrists or community mental health teams from across the country. It specialises in the treatment of antenatal and postnatal mental illnesses, predominantly for women who develop or have a relapse of serious mental illness during pregnancy, and women who develop postnatal depression, puerperal psychosis or have had a relapse of serious mental illness following the birth of their baby. They support the mother in developing a relationship with her baby in order to reduce the impact of the mother’s illness on the child. They offer a holistic treatment programme, and encourage the involvement of fathers or partners in the process. Mothers tend to be admitted with their baby where it is the wish of the mother and it is clinically safe to do so. However, they are also able to take mothers without their babies, and offer a programme of gradual reintroduction to the mother on the ward. Some of the interventions that the Mother and Baby Unit provide are: o Psychiatric assessment o Medication, if needed o Specialist psychological assessment, including impact of history of trauma and child abuse, mother-infant relationship and assessment of cognitive functioning o Risk assessments for mother, baby, husband, partner, carers and siblings o Psychological therapies including psychotherapy, CBT, CAT family therapy and couple therapy o Mother-infant relationship support, including baby massage, video feedback, infant’s physical and emotional development, parenting skills, promotion of attachment, play stimulation and development o Occupational therapies for mother and baby include: 12 1. life skills such as shopping, cooking, negotiating public transport, budgeting and assessment of home environment 2. health skills such as diet, physical activities, dancing and swimming 3. work skills including IT skills 4. leisure skills such as art, photography, pottery and woodwork o Pre-conception advice They also provide a parenting assessment service, providing a unique and highly specialised service to local and national authorities across the United Kingdom. They undertake assessments of women or couples and their infant, where there is potential risk or safeguarding issues arising from the parents’ mental health problems. In the last 12 months they have not had to refuse a referral due to a lack of beds. However, on the very rare occasions that this does occur, they will signpost the referrer to the next closest unit, and when a bed becomes available they will then transfer the patient over if they still wish to come to the unit. IAPT (Improving Access to Psychological Therapies) The Improving Access to Psychological Therapies (IAPT) programme supports the frontline NHS in implementing NICE guidelines for people suffering from depression and anxiety disorders. It was created to offer patients a realistic and routine first-line treatment, combined where appropriate with medication which traditionally had been the only treatment available. The programme was first targeted at people of working age, but in 2010 was opened to adults of all ages. It currently does not offer any services specifically designed for women suffering from mental illness during the perinatal period. These women can be seen by IAPT and offered a course of CBT, but specific, targeted treatments are not currently provided. If a woman in the perinatal period is referred to IAPT for psychological therapy she is made a priority and will go to the top of the waiting list. Caseload Team The midwifery caseloading team has been running since 2010 when it received funding from commissioners. It originally received funding for six fulltime midwives, and they currently have five and a half full time midwives. 13 Women are referred to the caseloading team from the booking visit or by their GP if it is felt that they will benefit from more continuity of care throughout their pregnancy. These women are those that tend to have chronic mental illness, or had severe mental illness in the past, or in previous pregnancies, or are vulnerable for another reason such as domestic violence. When the caseloading team was first set up commissioners suggested that 50% of their caseload should be normal low risk pregnancies, and 50% should be vulnerable women. However, this has not proved possible, and the team currently have a caseload of approximately 90% vulnerable women and 10% low risk pregnancies. They see these women up to 28 days postpartum. The team meet once a month to discuss the caseload, and they also hold a meet and greet once a month where all the women on the caseload can attend and meet all the midwives on the team and other expecting mothers. This ensures that the women get to know and feel comfortable with all the midwives who may be looking after them during their pregnancy. Antenatal appointments can either happen in the woman’s home or at the hospital, depending on what is preferable for the woman. There is no set schedule for appointments unlike in normal midwifery care, and the women are seen as often as necessary, whether it be a couple of times a week, or once every couple of weeks. The midwives are also on call for Labour Ward 24 hours a day, so when one of their women goes into labour they can attend and be there to support throughout the labour and delivery. The midwives will also attend scans with the women if they would like, and if they require admission, they will see them in the Mother and Baby Unit. The team works very closely with the perinatal mental health nurse, who can then signpost the women to further services and the perinatal mental health team if required. They also have close links with social services, health visitors and GPs, and liaise with them if appropriate. Pregnancy Support Team The pregnancy support team is a new team that was developed at Lewisham in May 2012 by the Safeguarding midwife, with the aim to link in with the NICE Complex Social Care guidelines. It is a multidisciplinary team that meets fortnightly to discuss all women with vulnerabilities at around the 28th week of their pregnancy. The aims of the group are to assess any risk to the pregnant woman, her unborn child and any existing children, to formulate a care plan to address vulnerabilities and reduce risk factors, to communicate effectively with other agencies as required and to identify instances and areas where action should be taken in order to ensure that children are safeguarded. 14 Members of the team include: Lead Midwife Safeguarding Advisor Perinatal Mental Health Nurse Social Worker Family Support Team Lands Team Midwives from various teams including the antenatal clinic, the caseload team and the teenage pregnancy team Midwifery Manager Women can be referred to the team by GPs and community midwives by filling in the referral form. Criteria for referral include: Currently/Previously known to Social Care Substance misuse Known mental health concern that is not severe enough to require referral to the caseload team Domestic Violence Alcohol abuse Older child with Special Needs Young Woman under age of 20 Disability Previous postnatal depression Female genital mutilation Previous late miscarriage or stillbirth Once referred the woman will be discussed around her 28th week of pregnancy at the multidisciplinary meeting and a plan will be made regarding her care. If necessary she will be signposted to other services that may be able to offer help and support. A letter is written to her GP detailing what the plan has been. The woman will then be re-discussed at 34 weeks to see how she is progressing, and to see whether she requires any further input. Again, a letter will be sent to the GP outlining the plan. Prior to this pregnancy support team, many women who did not fulfil the criteria to be referred to the caseload team, but would have required some extra support throughout their pregnancy and after, may have fallen through the cracks. This team has now filled the gap, so far more women will get the support and help they need. 15 Figure 4 The referral pathway for the Pregnancy Support Team Provided by the Pregnancy Support Team, Lewisham Healthcare Trust First disclosure: Client discloses current events or a history which could put her or her unborn child at risk. Consider severity of risk. Act promptly! www.nice.org.uk/guidance/CG110 RISK IDENTIFICATION History or current Serious mental illness Domestic Abuse Young Woman under the age of 20 Learning Disability Physical Disability (impact on parenting) Previous involvement with social services Previous children & not currently caring for them PND/Depression FGM Alcohol or Substance misuse Previous late miscarriage or stillbirth Referrals from other agencies GP’s (check letter/email/fax) Social Services –Child or adult A&E / NBC/other hospital ward Police ‘Other’ –voluntary agencies CONSIDER REFERRAL Get maximum information – main notes /GP/HV Unsure? Discuss with Lead Midwife Safeguarding/Perinatal Psychiatry Team/Senior staff REFERRAL CAF form to Lewisham Assessment & Referral Team at Lawrence House – email: Referral&AssessmentTeam@lewisham.gov.uk, fax:02083143447. CC or hardcopy to aine.gallagher@nhs.net If it is an urgent Child Protection issue, please call a Duty Social Worker on 020 8314 6660 or 020 8314 8018 or 020 8314 6294 Follow up referral response from Children’s Social Care within ONE week Refer to appropriate team or clinics to ensure all midwifery needs are met. Send a referral to the Pregnancy Support Team asap so the case can be discussed by 28/40 Woman’s named midwife/representative attend Pregnancy Support Team meeting with updated plan of care Ensure Safeguarding Plan is in main notes / Safeguarding Folders in departments/teams Ensure a flag is put on Terra Nova and PIMS if appropriate. 16 Strategies provided elsewhere St George’s NHS Trust At St George’s the perinatal psychiatry service works closely with the midwives and obstetricians to try to screen and identify mothers who are at risk of mental illness. The specialist midwife post was created to provide focused care to pregnant women with mental illness. The midwife is an important point of liaison between the other midwives, health visitors, child and family social services, obstetricians and mental health services. The mental health midwife is also a vital link to the local mother and baby unit. A member of the perinatal psychiatric team attends the weekly midwifery team meeting, where all community and labour ward teams meet to discuss the caseload, providing a valuable opportunity for potential referrals to be discussed. Understandable, many women will prefer and only require additional support and advice from a specialist midwife or their GP, rather than see a psychiatrist. However, some pregnant women will need to see a psychiatrist for expert input. To reduce the stigma, and make it a more integral part of routine antenatal care, the perinatal psychiatric clinic at St George’s has been relocated to the Foetal Medicine Unit where pregnant women go routinely for antenatal ultrasounds and booking appointments. Kings College Hospital Kings College Hospital has a dedicated Perinatal Mental Health team, and a clear referral pathway. In 2009 5,900 women booked for maternity care and 708 (12%) of them disclosed that they had a history of, or current mental disorder. Of these women 254 met the criteria for referral to the Perinatal Psychiatric Team. These included those with psychotic illness, severe depression, eating disorders, attempted suicides and serious self harm. Women who present with a history of depression or psychiatric problems; this can be past or present, are offered psychiatric referral by the midwife at the booking appointment. The midwife then completes a CAF form, SLAM form (Kings Perinatal Psychiatry Form) or GP assessment letter depending on the severity of the psychiatric problem. If a referral is being made to SLAM, a CAF referral to children’s social care in the borough of the mother’s residence should also be completed. Parental mental illness does not always have an adverse impact on a child’s development but it is essential to always assess it’s implications for each child in the family. 17 The Perinatal Psychiatry team should then respond directly to the referring midwife within 7 days and the referring midwife has the responsibility to ensure that any referral is followed up, information is shared with colleagues and actions documented. Women are then reviewed in the Department of Psychological Medicine Clinic at King’s or at The Maudsley Hospital. If a woman does not attend a planned appointment, the Perinatal Psychiatry Liaison Team are responsible for informing the named midwife for this woman and the relevant midwifery team. Those women for whom Perinatal Psychiatry Liaison Team and/or CAF referrals have been completed are booked to be discussed at the weekly Safeguarding Meeting. This is a multiagency meeting where women are discussed and actions resulting from the meeting are documented in the mother’s main hospital notes and a copy emailed to the relevant midwifery team. Each month a list of women who will need review following birth is also generated by the Safeguarding Meeting. These are women who are recognised at being high risk of exacerbating a pre-existing mental illness in the postnatal period. The list is emailed to all clinical areas within the maternity service, and it identifies the woman’s details and the recommended action plan. If admission to the Mother and Baby Unit at The Maudsley is planned, the Perinatal Psychiatrist will liaise directly with them during the pregnancy. Those women who have no previous mental illness and will therefore have no contact with the psychiatric team during their pregnancy may later require a referral to be made. This is especially applicable in the case of acute postpartum mental illness. 18 Figure 3 The referral pathway for referring to perinatal mental health at Kings College Hospital. Provided by Kings College Hospital Perinatal Team First disclosure of history of or current mental illness at booking/first contact at any time during maternity care Complete Referral Form Decide which referral Option – Perinatal or GP Gain consent. If refused and Option 1 discuss with Perinatal Team / Named Midwife /Consultant Midwife or Consultant Obstetrician Option 1 SLAM Perinatal Psychiatry Team Complete & Fax Unsure – Discuss with Team Member Ext 0203 299 3277 Option 2 GP Letter request mental health assessment Follow up referral in ONE MONTH Consider CAF referral if safeguarding concerns re unborn or previous children Discuss with Named Midwife or Perinatal Team if unsure Referring midwife/doctor Follow up referral in ONE WEEK Document plan of care *communicate plan to new lead professional/named midwife if care transferred Referring midwife/doctor Follow up referral in ONE month Document plan of care *communicate plan to new lead professional/named midwife if care transferred What is this telling us? What are the key gaps in knowledge and/or services? It was important to get the views and opinions about the service from the service providers and from the women using it. 19 GPs were asked about how they link in with the perinatal mental health service. Although the opinions expressed are probably personal reflections of the GPs themselves and can’t necessarily be broadened to all GPs, it gives a snapshot of how they feel about the service. GPs currently feel that they do not become hugely involved with the perinatal mental health service. Most referrals to the service of women suffering from mental illness during their pregnancy come from the midwives, and those women suffering from postnatal illness tend to get looked after by the GPs, or get referred to IAPT (Improving Access to Psychological Therapies) services. If they do refer to the service they feel that communication back is very poor, with few updates on their patient’s progress. Interestingly, the GPs also said that they tend not to assess a woman for psychiatric illness, domestic violence or any other vulnerability at her first presentation during her pregnancy, as they tend to leave this to the midwives at the booking visit. There is also concern from the women using the service and the perinatal mental health team that GPs are not confident in their knowledge about the use of psychotropic drugs during pregnancy. Because of this, when a woman sees her GP at the start of her pregnancy and is currently on medication for a mental illness, a large number of GPs stop the medication immediately. This can then lead to relapse, and the woman becoming more unwell very quickly. A further problem with the service that was mentioned by both the perinatal mental health team and the caseloading team is the difficulty with caring for women who are out of area, or live just across the border, but have still booked at Lewisham to have their baby. At the moment these women cannot be looked after by the caseloading team, or the Lewisham perinatal mental health team even if they fit the referral criteria. These women are therefore not necessarily getting the best possible care and support that they may need through their pregnancy. Psychological treatments have been shown in numerous studies to help reduce the impact and severity of perinatal mental illness, and aid recovery. In Lewisham, and elsewhere throughout the country, there is a huge problem with accessing these services, due to long waiting lists, or not being available in a certain area. The introduction of IAPT was meant to improve this, and in some instances it has. However, in Lewisham there is no specific psychological treatment service for perinatal mental illness, so women are referred to IAPT. The opinion of the perinatal mental health team is that IAPT does not have the experience or the expertise to deal with these women, particularly those with 20 severe mental illness. However, the opinion of many at IAPT is that they do have the skill set to help these women, but that they do not have the funding or the time to offer a specialised service. They would be keen to become more involved in standard antenatal care, and perhaps attend antenatal classes to speak to women and assess whether any may benefit from input antenatally. There have also been problems with getting women reviewed on the maternity or postnatal wards urgently, either out of hours or not. This is because the perinatal team at Lewisham is so small, and are often not on site. On these occasions it falls to the liaison psychiatry team to review the woman and to come up with an initial management plan. Problems have occurred with this when the liaison psychiatry state they are too busy, or do not deal with perinatal mental health, and the women can be left on the ward with no review for a few days. What should we be doing next? Recommendation More formal training for midwives, health visitors and obstetricians regarding mental illness, so that they are more likely to recognise the signs, and are aware of the services and referral pathways available for these women. Further education for GPs regarding psychotropic medication during pregnancy. This could include mandatory training. Improve counselling given to women prescribed psychotropic medication about when to seek advice about stopping or changing medication if they plan on becoming pregnant, or when they do become pregnant. Encourage GPs to use the Whoolley questions when a woman presents to them when pregnant. Consider employment of a single named midwife with an interest in mental illness to work closely alongside the perinatal mental health team. Improve access and quality of To discuss with Lewisham Healthcare Trust Primary Care Team Lewisham Healthcare Trust, SLAM and Primary Care Team Primary Care Team Lewisham Healthcare Trust Mental Health Commissioners 21 psychological therapies for women with perinatal mental illness, in particular, to consider in some depth how IAPT might be used for this purpose. Develop a pathway for the care of SLAM and SEL Maternity Network women who have booked at Lewisham for their maternity care, but are from out of area so can not be looked after by the caseloading team, or the perinatal mental health team. Develop a formal agreement between SLAM and Lewisham Healthcare Trust perinatal mental health and liaison psychiatry so that in the case of an urgent referral when the perinatal team are not available, the liaison psychiatry team review the patient urgently and initiate management if necessary. Increase the number of sessions SLAM provided at Lewisham by the consultant psychiatrist and specialist registrar. Conclusion It would appear that the services for women suffering from perinatal mental illness in Lewisham are currently meeting demand, and although some improvements need to be made the provision for these women is adequate and provides a vital and necessary service. Ideally, the perinatal mental health service would be a service with a full time consultant psychiatrist and at least one full time specialist registrar within Lewisham. However, this is currently impossible, and the staff are providing an overall efficient service with limited resources. As with any service there are going to be shortcomings and the perinatal mental health service is no different, as documented by the recommendations above. However Lewisham Healthcare Trust is already trying to bridge some of the gaps, such as the limited provision for those women with mild to moderate mental illness, by the introduction of the pregnancy support group, and this will go a long way to improving the quality of care this vulnerable group of women receive. 22 It is also this group of women with mild to moderate mental illness that often most benefit from psychological treatment, as the impact of the illness on the woman, baby and her family can be just as devastating as those suffering with severe mental illness. Further improvement to the service targeted to this group could also be made if greater use of specific IAPT services were agreed. Acknowledgements Dr Donal O’Sullivan, Public Health Consultant Pauline Cross, Consultant midwife in Public Health The Public Health Team at Lewisham Miss Billett, perinatal mental health obstetric lead Jessica Ormerod, NCT volunteer who spoke to me at length about the service provision and put me in touch with some service users Jill Demilew, consultant midwife at Kings College Hospital Dr Judy Chen, Principal GP and Safeguarding Children Lead Eleanor Davies, Associate Director of Joint Mental Health Commissioning Shirley Petersen, Community Services Manager for Maternity Services Sarah Buck, Lead Midwife on the Caseloading Team Vita Shrinarine, Perinatal Mental Health Nurse Dr Trudi Seneviratne, Consultant Psychiatrist, Perinatal Mental Health Team Jackie Ganley, Consultant Clinical Psychologist at IAPT Ailsa Ward, Mental Health Nurse, Mother and Baby Unit, The Bethlem Royal Hospital References 1. Lewisham Strategic Partnership Website http://www.lewishamstrategicpartnership.org.uk/borough.asp 2. Out of the blue? Motherhood and depression (2006) 3. NICE (2007) Antenatal and postnatal mental health. London: National Institute for Health and Clinical Excellence. 4. Williams JW Jr, Kerber CA, Mulrow CD, et al. Depressive disorders in primary care: prevalence, functional disability, and identification. Journal of General Internal Medicine. 1995;10:7–12. 5. Cox JL, Murray D, Chapman G. A controlled study of the onset, duration and prevalence of postnatal depression. The British Journal of Psychiatry. 1993;163:27–31. 23 6. O’Hara MW, Swain AM. Rates and risk of postpartum depression – a metaanalysis. International Review of Psychiatry. 1996;8:37–54. 7. Brockington IF. Motherhood and Mental Health. Oxford; Oxford University Press; 1996. 8. Nonacs R, Cohen LS. Postpartum mood disorders: diagnosis and treatment guidelines. The Journal of Clinical Psychiatry. 1998;59:34–40. 9. Office for National Statistics. 2006. http://www.statistics.gov.uk. 10. Kendell RE, Chalmers JC, Platz C. Epidemiology of puerperal psychoses. The British Journal of Psychiatry. 1987;150:662–673. 11. Viguera AC, Nonacs R, Cohen LS, et al. Risk of recurrence of bipolar disorder in pregnant and nonpregnant women after discontinuing lithium maintenance. The American Journal of Psychiatry. 2000;157:179–184. 12. Maternal Mental Health and Child Health and Development http://www.who.int/mental_health/prevention/suicide/MaternalMH/en/index.html 13. Louise Howard, Katherine Hunt, Mike Slade, Veronica O’Keane, Trudi Seneviratne, Morven Leese, Graham Thornicroft and Malcolm Wiseman (2008) CAN-M: Camberwell Assessment of Need for Mothers 14. The Confidential Enquiry into Maternal Deaths (2001, 2004) 15. Ammaniti, M., Speranza, A. M., Tambelli, R., et al. (2006) A prevention and promotion intervention program in the field of mother-infant relationship. Infant Mental Health Journal, 27, 70–90. 16. Boath, E. H., Pryce, A. J. & Cox, J. L. (1998) Postnatal depression: the impact on the family. Journal of Reproductive and Infant Psychology, 16, 199–203. 17. Beck, C. T. (2001) Predictors of postpartum depression: an update. Nursing Research, 50, 275–285. 18. Bonari, L., Pinto, N., Ahn, E., et al. (2004) Perinatal risks of untreated depression during pregnancy. Canadian Journal of Psychiatry, 49, 726–735. 19. Gavin, N. I., Gaynes, B. N., Lohr, K. N., et al. (2005) Perinatal depression: a systematic review of prevalence and incidence. Obstetrics and Gynecology, 106, 1071–1083. 24 20. Harlow, B. L., Vitonis, A. F., Sparen, P., et al. (2007) Incidence of hospitalization for postpartum psychotic and bipolar episodes in women with and without prior prepregnancy or prenatal psychiatric hospitalizations. Archives of General Psychiatry, 64, 42–48. 21. Hay, D. F., Pawlby, S., Sharp, D., et al. (2001) Intellectual problems shown by 11-year-old children whose mothers had postnatal depression. Journal of Child Psychology and Psychiatry, 42, 871–889. 22. Horowitz, J. A., Bell, M., Trybulski, J., et al. (2001) Promoting responsiveness between mothers with depressive symptoms and their infants. Journal of Nursing Scholarship, 33, 323–329. 23. Jablensky, A. V., Morgan, V., Zubrick, S. R., et al. (2005) Pregnancy, delivery, and neonatal complications in a population cohort of women with schizophrenia and major affective disorders. The American Journal of Psychiatry, 162, 79–91. 24. Lovestone, S. & Kumar, R. (1993) Postnatal psychiatric illness: the impact on partners. The British Journal of Psychiatry, 163, 210–216. 25. Robertson, E., Grace, S., Wallington, T., et al. (2004) Antenatal risk factors for postpartum depression: a synthesis of recent literature. General Hospital Psychiatry, 26, 289–295. 26. Oates, M. (2000) Perinatal Maternal Mental Health Services. Council Report CR88 London: Royal College of Psychiatrists. 27. Killaspy H, Bebbington P, Blizard R, et al. The REACT study: randomised evaluation of assertive community treatment in north London. British Medical Journal. 2006;332:815–820. 28. Whooley, M. A., Avins, A. L., Miranda, J., et al. (1997) Case-finding instruments for depression. Two questions are as good as many. Journal of General Internal Medicine, 12, 439–445. 29. Arroll, B., Goodyear-Smith, F., Kerse, N., et al. (2005) Effect of the addition of a ‘help’ question to two screening questions on specificity for diagnosis of depression in general practice: diagnostic validity study. British Medical Journal, 331, 884. 30. Austin, M. P. & Lumley, J. (2003) Antenatal screening for postnatal depression: a systematic review. Acta Psychiatrica Scandinavica, 107, 10–17. 25 31. Elliott, S. A., Leverton, T. J., Sanjack, M., et al. (2000) Promoting mental health after childbirth: a controlled trial of primary prevention of postnatal depression. The British Journal of Clinical Psychology, 39, 223–241. 32. Evans, J., Heron, J., Francomb, H., et al. (2001) Cohort study of depressed mood during pregnancy and after childbirth. British Medical Journal, 323, 257– 260. 33. Altshuler, L. L., Cohen, L., Szuba, M. P., et al. (1996) Pharmacologic management of psychiatric illness during pregnancy: dilemmas and guidelines. The AmericanJournal of Psychiatry, 153, 592–606. 34. Appleby, L., Warner, R., Whitton, A., et al. (1997) A controlled study of fluoxetine and cognitive-behavioural counselling in the treatment of postnatal depression. British Medical Journal, 314, 932–936. 35. Miller, L. J. (1995) Use of electroconvulsive therapy during pregnancy. Obstetrical and Gynecological Survey, 50, 10–11. 36. Spencer, J. P., Gonzalez, L. S., III & Barnhart, D. J. (2001) Medications in the breastfeeding mother. American Family Physician, 64, 119–126. 26