Study Evaluates Fluoride Intake and Risk of Fluorosis

Caries Res.
2006;40(6):494-500.
Links
Fluoride intake levels in relation to fluorosis development in permanent maxillary central incisors and first molars.
Hong L ,
Levy SM ,
Warren JJ ,
Broffitt B ,
Cavanaugh J .
Department of Dental Public Health and Behavioral Science, School of Dentistry,
University of Missouri-Kansas City, Kansas City, Mo., USA.
Gaps remain in our knowledge about the levels of fluoride intake that cause dental fluorosis. The purpose of this study was to report the fluorosis prevalence by levels of estimated fluoride intake in an effort to understand the importance of different levels of daily fluoride intake. As part of the longitudinal Iowa
Fluoride Study, subjects were followed from birth to 36 months with questionnaires every 3-4 months to gather information on fluoride intake from various sources. Daily fluoride intake in mg per kg body weight (BW) was estimated from water, beverages and selected foods, fluoride supplements and dentifrice. Six hundred and twenty-eight subjects were examined for fluorosis on permanent incisors and first molars at about age 9 by two calibrated examiners using the Fluorosis Risk Index categories. Fluorosis prevalence rates were determined separately for maxillary central incisors and first molars by levels of estimated fluoride intake. There were significant positive associations between fluorosis prevalence and levels of fluoride intake. Cumulatively from birth to 36 months, average daily intake of 0.04 mg F/kg BW or less carried relatively low risk for fluorosis (12.9% for maxillary central incisors, 6.8% for first molars).
Average daily intake of 0.04-0.06 mg F/kg BW showed a significantly elevated risk for fluorosis (23.0% for maxillary central incisors, 14.5% for first molars), while fluorosis risk was even higher for average intake above 0.06 mg F/kg BW
(38.0% for maxillary central incisors, 32.4% for first molars). The study suggests that fluorosis prevalence is related to elevated fluoride intake when averaged over the first 3 years of life, but is even more strongly related to fluoride intake that is elevated for all of the first 3 years of life.
http://www.nidcr.nih.gov/NewsAndReports/ScienceNewsInBrief/FluorideIntake.htm
Study Evaluates Fluoride Intake and Risk of
Fluorosis
December 8, 2006
In the early 1930s, several public health dentists wondered whether the fluoride levels of the drinking water in Colorado Springs might account for the unusual discoloration of the tooth enamel of some residents. Dr. Trendley
Dean, one of the dentists who later would serve as the first NIDCR director, called the condition “dental fluorosis.” Dean and his colleagues later confirmed their suspicion and found that children who ingest excessive amounts of fluoride as their teeth develop may decrease the mineral content of their underlying tooth enamel. This change can cause white opacities or, in severe cases, pits and/or brown mottling of the enamel. However, because of the many substantial scientific and logistical challenges of assessing total fluoride intake during the first few years of life, still unclear nearly 75 years later is the specific level of fluoride intake necessary to cause fluorosis. In the October issue of the journal Caries Research , NIDCR grantees and colleagues help to answer the question by analyzing the fluoride intake of 628 children over several years from multiple sources including water, beverages, selected foods, and dentifrices. The scientists found the prevalence of fluorosis (almost all mild) was higher above a cumulative average daily intake during a child’s first three years of 0.04 milligrams fluoride/kilogram of bodyweight, with greater risk above 0.06 mg fluoride/kilogram bodyweight. Below this level, the risk was considered low. The scientists noted that the relationship between total fluoride intake and fluorosis was apparent over time for both the maxillary central incisors and first molars. They also found that the development of fluorosis appears to relate to the duration of cumulative exposure to high amounts of fluoride.
0.04 Cumulative average daily intake X 10 kg = 0.4 mg of fluoride. 2 yr old one glass max.
http://www.fluoridealert.org/health/teeth/fluorosis/mild.html
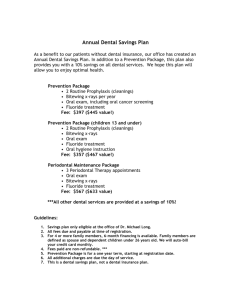
PICTURES - Mild Dental Fluorosis:
"Very Mild"/Mild Fluorosis
Photo by Hardy Limeback, DDS
"Very Mild" Fluorosis
Source of Photo Unknown
Mild Fluorosis
Photo by Hardy Limeback, DDS
Classification Criteria - Mild Dental Fluorosis: ( back to top )
Mild Fluorosis
Photo by Elke Babiuk
Classification Criteria for Mild Dental Fluorosis - Dean's Fluorosis Index
Score Criteria
Normal The enamel represents the usual translucent semivitriform type of structure. The surface is smooth, glossy, and usually of a pale creamy white color.
Very
Mild
Small opaque, paper white areas scattered irregularly over the tooth but not involving as much as 25% of the tooth surface. Frequently included in this classification are teeth showing no more than about 1-2 mm of white opacity at the tip of the summit of the cusps of the bicuspids or second molars.
Mild
The white opaque areas in the enamel of the teeth are more extensive but do not involve as much as 50% of the tooth.
To see Dean's complete index , with descriptions of moderate to severe fluorosis, click here )
Current Prevalence - Mild Dental Fluorosis: ( back to top )
"The prevalence of fluorosis at a water fluoride level of 1.0 ppm was estimated to be 48% and for fluorosis of aesthetic concern it was predicted to be 12.5%."
SOURCE: McDonagh, M. et al. (2000).
A Systematic Review of Public Water Fluoridation . NHS Center for
Reviews and Dissemination, University of York.
"[S]everal reports of prevalence for mostly mild fluorosis are in the 20 percent to 80 percent range."
SOURCE: Levy SM, Guha-Chowdhury N. (1999). Total fluoride intake and implications for dietary fluoride supplementation. Journal of Public Health Dentistry 59: 211-23.
"Current studies support the view that dental fluorosis has increased in both fluoridated and non-fluoridated communities. North American studies suggest rates of 20 to 75% in the former and 12 to 45% in the latter."
SOURCE: Locker, D. (1999). Benefits and Risks of Water Fluoridation. An Update of the 1996 Federal-
Provincial Sub-committee Report . Prepared for Ontario Ministry of Health and Long Term Care.
Impact on Tooth Quality - Mild Dental Fluorosis: ( back to top )
Note: For more information on the biology of dental fluorosis, click here
"Dental fluorosis is defined as a permanent hypomineralization of enamel, characterized by greater surface and subsurface porosity than in normal enamel, that results from excess fluoride (F) reaching the developing tooth during developmental stages.
"
SOURCE: Burt BA ; Eklund SA. (1999). Dentistry, Dental Practice, and the Community (5th Ed). WB
Saunders Co; Philadelphia.
"Any use of fluorides, whether systemic or topical, in caries prevention and treatment in children results in ingestion and absorption of fluoride into the blood circulation. The mineralization of teeth under formation may be affected so that dental fluorosis may occur. Dental fluorosis reflects an increasing porosity of the surface and subsurface enamel, causing the enamel to appear opaque. The clinical features represent a continuum of changes ranging from fine white opaque lines running across the tooth on all parts of the enamel to entirely chalky white teeth. In the latter cases , the enamel may be so porous (or hypomineralized) that the outer enamel breaks apart posteruptively and the exposed porous subsurface enamel becomes discolored."
SOURCE: Fejerskov O, et al. (1990). The nature and mechanisms of dental fluorosis in man.
Journal of
Dental Research 69(Spec Iss): 692-700.
Impact on Bone Quality? - Mild Dental Fluorosis: ( back to top )
Bone fractures vs
Dean dental fluorosis index
SOURCE:
Alarcon-Herrera MT, et al. (2001). Well Water Fluoride, Dental fluorosis, Bone
Fractures in the Guadiana Valley of Mexico. Fluoride 34(2): 139-149. ( See paper )
"A linear correlation between the Dean index of dental fluorosis and the frequency of bone fractures was observed among both children and adults."
SOURCE: Alarcon-Herrera MT, et al. (2001). Well Water Fluoride, Dental fluorosis, Bone Fractures in the
Guadiana Valley of Mexico. Fluoride 34(2): 139-149.
"it is illogical to assume that tooth enamel is the only tissue affected by low daily doses of fluoride ingestion."
SOURCE: Dr. Hardy Limeback, Head of Preventive Dentistry, University of Toronto. (2000). Why I am now
Officially Opposed to Adding Fluoride to Drinking Water .
"Common sense should tell us that if a poison circulating in a child's body can damage the tooth-forming cells, then other harm also is likely."
SOURCE: Colquhoun J. (1997). Why I changed my mind about Fluoridation. Perspectives in Biology and
Medicine 41:29-44.
"The safety of the use of fluorides ultimately rests on the assumption that the developing enamel organ is most sensitive to the toxic effects of fluoride. The results from this study suggest that the pinealocytes may be as susceptible to fluoride as the developing enamel organ."
SOURCE: Luke J. (1997). The Effect of Fluoride on the Physiology of the Pineal Gland . Ph.D. Thesis.
University of Surrey, Guildford. p. 176.
"It seems prudent at present to assume that the ameloblasts are not the only cells in the body whose function may be disturbed by the physiological concentrations of fluoride which result from drinking water containing 1 ppm"
SOURCE: Groth, E. (1973), Two Issues of Science and Public Policy: Air Pollution Control in the San
Francisco Bay Area, and Fluoridation of Community Water Supplies. Ph.D. Dissertation, Department of
Biological Sciences, Stanford University, May 1973.
Perception/Psychological Effects - Mild Dental Fluorosis: ( back to top )
Note: For information on the psychological impact of moderate to severe fluorosis, click here
"Many participants reported that they were at least occasionally distressed or worried over the appearance of the children's teeth, that it hindered children from smiling freely, and that it was an unsatisfactory appearance."
SOURCE: Martinez-Mier EA, et al. (2004). Development of a questionnaire to measure perceptions of, and concerns derived from, dental fluorosis.
Community Dental Health 21:299-305.
"Mildly fluorosed enamel is fully functional, but may be cosmetically objectionable."
SOURCE: Agency for Toxic Substances & Disease Registry [ATSDR]. (2003). Toxicological profile for
Fluorides, Hydrogen Fluoride, and Fluorine . Atlanta, GA: U.S. Department of Health and Human Services,
Public Health Service.
"There is some evidence that members of the public can be aware of even mild changes due to fluorosis and may display a preference for 'normal' over mildly fluorotic teeth. Our studies of esthetic perceptions of dental fluorosis found that members of the public had strong preferences about variations from normal tooth appearance. For example, all respondents had a preference for teeth with normal colour over teeth with mild fluorosis, whereas about two-thirds preferred the appearance of an open bite to that of moderate fluorosis.."
SOURCE: Levy SM. (2003). An update on fluorides and fluorosis. Journal of the Canadian Dental
Association 69: 286-91.
"Mild fluorosis was assessed less favorably than normal/control, midline diastema was less favorable than mild fluorosis, and mild fluorosis was less favorable than isolated opacity."
SOURCE: McKnight CB, et al. (1999). A pilot study of dental students' esthetic perceptions of computergenerated mild dental fluorosis compared to other conditions. Journal of Public Health Dentistry 59: 18-23.
"Although many dental professionals often state that very mild fluorosis is not a cosmetic problem, these results suggest that it is perceived otherwise. Even parents of children suffering from very mild fluorosis showed an increase in dissatisfaction with their child's apperance."
SOURCE: Lalumandier JA, Rozier RG. (1998). Parents' satisfaction with children's tooth color: fluorosis as a contributing factor. Journal of the American Dental Association 129: 1000-6 .
"South Australian children 10- to 17-years-old were able to recognize very mild and mild fluorosis and register changes in satisfaction with the colour and appearance of teeth. Even mild changes were associated with psycho-behavioural impacts. Hoskin and Spencer asked eight questions on psychobehavioural impact, such as embarrassment of teeth or self consciousness because of the appearance of the teeth... The most dramatic finding was the strength of the association of TISF score with psychobehavioural impact was similar to that of crowding and overbite, both considered key occlusal traits driving the demand for orthodontic care. "
SOURCE: Spencer AJ, et al. (1996). Water fluoridation in Australia. Community Dental Health 13(Suppl 2):
27-37.
"Not unexpectedly, children with fluorosis on anterior teeth ranging between TSIF scores of "2" to "6" appear to have increased concerns about tooth color."
SOURCE: Clark DC, et al. (1994). Aesthetic concerns of children and parents in relation to different classifications of the Tooth Surface Index of Fluorosis. Community Dentistry and Oral Epidemiology 22: 461-
4.
"The results, based on just over 3000 responses, showed that lay and dental observers could distinguish between different fluorosis levels. In response to a statement that the teeth appeared pleasing, a large
majority agreed when the TF (fluorosis) score was 0, but agreement declined as the TF score increased; when the TF score was 3, most people disagreed. Similarly, observers felt that the appearance would increasingly embarrass the child as the TF score increased. Observers, except the dentists, tended to feel that higher TF scores indicated neglect on the part of the child."
SOURCE: Riordan PJ. (1993). Perceptions of dental fluorosis. Journal of Dental Research 72: 1268-74.
Back to top