individualized epinephrine emergency action plan
advertisement

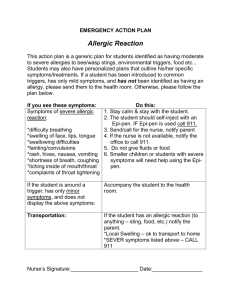
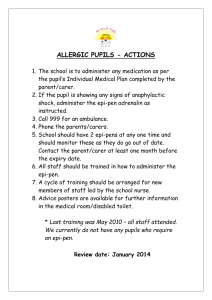
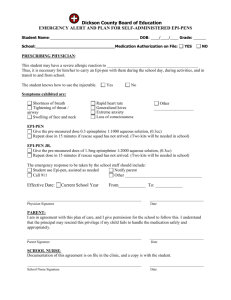
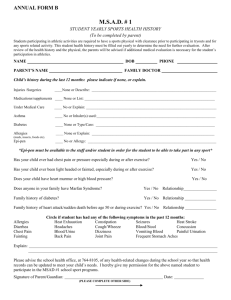
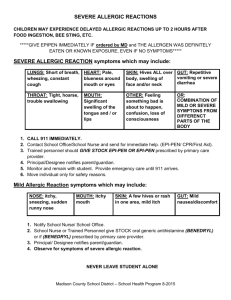
INDIVIDUALIZED EPINEPHRINE EMERGENCY ACTION PLAN Student’s Name:__________________________DOB:_________GRADE:________ ALLERGY TO:________________________________________________________ ASTHMATIC Yes *_____ NO_____ *High risk for severe reaction SIGNS OF AN ALLERGIC REACTION (Highlight or circle symptoms appropriate to child) Systems: Mouth Throat Skin Gut Lung * Heart * Place Child’s Picture Here Symptoms: Itching and swelling of the lips, tongue, or mouth Itching and/or a sense of tightness in the throat, hoarseness, and hacking cough Hives, itchy rash and/or swelling about the face or extremities Nausea, vomiting, abdominal cramps and/or diarrhea Shortness of breath, repetitive coughing and/or wheezing Thready pulse, passing out The severity of symptoms can quickly change. *All above symptoms can potentially progress to a life threatening situation. 1. If an allergic reaction is suspected, give: _____0.3mg Epi-Pen IM or _____0.15mg Epi-pen Junior IM and Benadryl __________PO immediately. dosage 2. Call Emergency Medical Services: 9-1-1 3. Call School Nurse if not present. 4. Call: Mother______________________________________________________________________ (home) (work) (cell) Call: Father_______________________________________________________________________ (home) (work) (cell) or emergency contacts (listed on other side) 5. Possible side effects of Epi-Pen: Palpitations, tachycardia (rapid heart beat), sweating, nausea, vomiting, breathing difficulties, pale skin color, dizziness, weakness, tremor, headache, anxiety apprehension, and nervousness. 6. Stay with child until emergency help arrives – position child on left side. DO NOT HESITATE TO ADMINISTER MEDICATION OR CALL EMERGENCY MEDICAL SERVICES, EVEN IF PARENTS CANNOT BE REACHED! Physician Signature:____________________________________________Date:_______________________ All students must be transported to the hospital by Emergency Medical Services (EMS) after receiving Epi-pen. Page 1 I give permission for the school nurse (or appropriately trained school personnel) to administer Epi-Pen and share information as deemed necessary for my child’s health and safety. I give permission for my son/daughter to self-administer their Epi-Pen as prescribed by his/her physician. ______Yes ______No Parent Signautre:______________________________Date:_____________________________ Nurse Signature:______________________________Date:_____________________________ Epi-Pen Location(s): Expiration Date(s): __________________________________________________________________________________________ __________________________________________________________________________________________ Page 2