Asthma Action Plan
advertisement

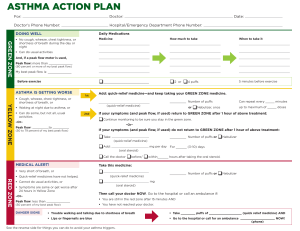
Asthma Action Plan Name Date of birth Green means GO! Use preventive asthma medicine. Parent Parent’s number Yellow means CAUTION. Add Yellow Zone medicine. Doctor Doctor’s number Other emergency contact Contact’s number Red means DANGER! Use Red Zone medicine & call Dr. Date created: __ / __ / __ Reviewed: __ / __ / __ __ / __ / __ __ / __ / __ Student is able to self-medicate? □ Yes □ No Green (GO!) No cough, Peak flow wheeze, above: chest _________ tightness, or shortness of breath Can do usual activities Use preventive medicines every day: Medicine Continue with preventive medicine and add Yellow Zone medicines: Medicine How much to take How often/how long to take it First, take quick-relief medicine> Then > Additional instructions: If symptoms are the same after 24 hours or get worse, call your child’s doctor. If your child needs Yellow Zone medicines over 2-3 times per week, call his/her doctor. Take these medicines and call your child’s doctor: RED (DANGER!) Very short Peak flow of breath below: _________ Trouble talking or walking Working hard to breathe Breathing faster than usual Noisy breathing even at rest Very fussy Grey or blue skin color How often to take it For asthma with exercise, take: Yellow (CAUTION) Cough, Peak flow: wheeze, _______ to chest ______ tightness, or _ shortness of breath Feels tired or restless Waking at night due to asthma Can’t do all of usual activities How much to take Medicine How much to take How often/how long to take it First, take quick-relief medicine> Then > Additional instructions: Call your child’s doctor NOW! Go to the emergency room or call 911 if: Your child is still in the Red Zone after 15 minutes and you cannot reach your doctor Your child has trouble walking or talking or lips or fingernails are blue Please bring this plan to all doctor visits.