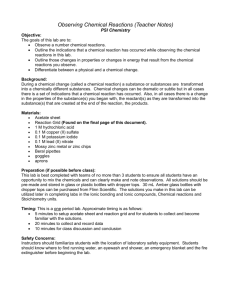
Abstract This study was applied on fifty patients having urinary
advertisement

Role of Oxidative Stress by Lipid Peroxidation in Developing Urinary Bladder Cancer and Correlation between Malondialdehyde and Trace Elements Copper and Zinc Thanaa M. Juda Mufeed J.Ewad Mohammed R.Judy Kadum J.Alhamdani Babylon University,College of Medicine, Hilla- P.O. Box 473, Iraq. MJ B Abstract This study was applied on fifty patients having urinary bladder cancer, proved by histopathological study for the biopsy taken from the bladder by cystoscopy performed under general anesthesia. In this study the type of cancer was transitional cell carcinoma of urinary bladder of different stages. In this study changes in malondieldehyde as biomarker of lipid peroxidationhave been studied the result revealed significant elevation in patient groups compared with control, and glutathione level (GSH) which considered as antioxidant defenses mechanism are significantly reduced in patients groups in comparison to control groups. The changes in level of trace elements copper and zinc are study in this work, the result revealed increase level of copper and reduced level of zinc in patients groups in comparism with control groups لدرا دس ذذتل الخالصة بتذذتللذذنل ذ. عذخلإصذذب عةهلر ذذسابنلدرل. بتذذتخلعذذهلد عذذذبسههلرةذ الدرا دس ذذتل.هذ الدرا دس ذذتلعلذذخلس ذ ل ل ذينللسيضذذبلر ذذسابنلدرل بتتلدر يلعهلإج دسلؤالعحخلدرع ايسلدرعبهلخ ل.لتبظ سلدرل بتتللنل.درت يجذتلر عيتبخلدرعيلعهلأ هبللنلرابتتلدرل بتتلفيللسدحللل ع فتخ ل.لنله الدرا دس تلكبنلت علدر سابنله ل سابنلدرت يجلدرا ئيلدالتعقبريلر ل كبتخلدرتعيجذتلدسعفذبعلل حذ يلفذيلل ذع ىلدرلبر تايةبيذالستذاللسضذ ل,فيله الدرا دس تلعهلقذبسلل ع ىلدرلبر تايةبيالكادرتلألك اةلدراه نل بتتللقبستتللعللجل ستلدرضبراتخ ل.سابنلدرل بتذتللقبستذتلستذال.بي نلدرل عز لدر يلذعع سلكلضبادخلافبسذتلضالدألك اةلفقالكبتخللت فضتلستاللسضذ ل ذسابنلدرل.ألبلل ع ىلدرك عب لجل ستلدرضبراتخ ل لدرعتبص ذ لس هيلحص ذسدلدرتحذذبسل لدر بسصذذينل لكبتذذخلدرتعيجذذتلدسعفذذبعلفذذيلل ذذع ىل فذذيله ذ دلدرعلذذللعذذهلا دس ذذتلدرعسي ذسدخلفذذيلل ذذع ىلرع ذ بتتللقبستتلرلجل ستدرضرط لخ ل.لفيلل ع ىلدر بسصينلستاللسض ل سابنلدرل درتحبسل لدت فب ذذذذذذذذذذذذذذذذذذذذذذذذذذذذذذذذذ ل Introduction U rinary bladder cancer (UBC) is the fifth most common cancer in the United States and western countries where it is a disease of white men over the age of sixty five [1]. The incidence of bladder cancer increases with age ,few cases of occur under the age of forty, the male to female ratio ranges from 2:I -4:1,and the incidence is more common in large urban centers due to the increasing increase exposure to risk factors[2]. Development and progression of bladder cancer is derived by the malfunction of specific gene i.e. due to over expression of oncogen or inactivation of tumor suppressor genes. The oncogen that has been associated with bladder cancer is (ras)gene family mainly, including p21 ras oncogen. The most important suppressor gene isP53 [3]. Nearly all UBC are arise from transitional epithelial lining due to exposure of urothelium to chemical carcinogen, and the bladder is common site of transitional cell tumor (TCT) [4].The other bladder cancer are:1. Adeno carcinoma account for less than 2%of all bladder cancer 2. Sequomous cell carcinoma (SCC) account for 5-10%of all bladder cancer, it is associated with history of chronic infection [5].In under developed nations (SCC) is associated with bladder infection by schistosoma haematoma [6]. Staging is done to obtain prognostic information and to guide treatment selection, stage1 tumor confined to epithelium, stage2 Tumor invasive to muscularis propria, stage3 tumor involvement of perivesical fat, stage4 distal metastasis [7]. Tobacco smoking is the most established modifiable risk factor for bladder cancer [8].Cigarette smoking induced oxidative stress and involved in DNA damage, and impaired anti oxidative defense mechanism [9]. Variety of industrial exposure risk for bladder cancer as aromatic amines present in product of dyes and occupational hazard are painter, drivers, hair dresser [10]. The disturbance between prooxidant and antioxidant balance results in oxidative stress which is defined as imbalance between the production of various reactive oxygen species(ROS) and the ability of antioxidant protective mechanism to cope with these ROS and prevent its adverse effect on biological system [11]. These ROS have one or more unpaired electrons in there's outer shells. It is consequently has tendency to accepted an electron from other substance make it highly reactive, these ROS including super oxide anion radical O2.-, Hydroxyl radical HO. , Hydrogen peroxide H2O2, Lipid peroxide radical Roo. Singlet oxygen 1 O2, Hypochlorous HOCL, Ozon O3 [12]. The first sources for ROS are mitochondria through respiratory chain [13]. The second sources are enzymatic action as oxidase, Dioxygynase, xanthenes oxidase, cytochrome P450 Nitric oxide synthase [14]. Third source for ROS are xenobiotics [15]. Interactions between ROS and antioxidant are as follow [16]. Figure 1 The prooxidant and antioxidant network Lipid peroxidation is oxidative degradation of lipid ,by which free radicals steal electron from lipid in cell membrane and resulting in cell damage Poly unsaturated fatty acid (PUFA) serve as excellent substrate for lipid peroxidation [17]. Lipid peroxidation process yields several cytotoxic product including saturated aldehydes e.g. Malondialdehyde (MDA) and unsaturated aldehydes e.g. 4-hydroxy –trans-2-nonenal and 4- hydroxy-2hexenal (4-HHE) and acrolein [18] These aldehyde react with cellular nucleophiles such as glutathione (GSH) and cystiene, histidine, lysine residues of protein which causes destructive functional modification and its effect on DNA resulting in genotoxic effect that promotes cancer [19]. Glutathione (GSH) reduced form is a linear tripeptide of L.glutamate, L-cysteine and glycine. GSH has sulfhydryl (SH) group on cysteinyl portion, which account for its strong electron donating character. As electrons are lost from the GSH the molecule become oxidized and two such molecules becomes linked by disulfide bond to form glutathione disulfide or oxidized glutathione (GSSG) . This linkage is reversible upon rereduction, so GSH is under tight haemostatic control both intra cellular and extra cellular .So a dynamic balance is maintained between GSH synthesis, its recycling The first reaction catalyzed by the from GSSG and metabolism. action of gamma- glutamyl cysteine The synthesis of GSH involves two synthetase as follow:closely linked enzymatic controlled reactions. 1. Glutamate +cysteine +ATP gamma-glutamyl cysteine+ADP+P The second reaction catalyzed by glutathione synthetase 2. Gamma glutamyl cysteine +glycine +ATP glutathione +ADP+P[20]. Zinc is essential trace element for all forms of life. It is absorbed from duodenum, zinc is mostly transported bound to albumen, alpha-2macroglobulin and transferene, zinc sequestration in enterocytes with metalothionein, some of this transfer to the plasma, the rest is lost when the enterocytes are sloughed [21]. Zinc plays important roles in growth and development, the immune response, neurological function, and reproduction [22]. Zinc has antioxidant action [23]. And anticancer action [24]. And has role in vitamine A action Zinc is a component of retinol binding protein, which is necessary for transporting vitamin A in the blood [25]. .Copper in the body shifts between the cuprous (Cu+1) and cupric (Cu+2), the ability of copper to easily accept and donate electron explains it is important role in oxidation- reduction (redox) effect about 90% of copper bound to ceruloplasmen which is copper contains protein the copper containing enzyme, while when copper first absorbed by intestine it is transported to liver bound to albumen. Ceruloplasmen (ferroxidasel) and (ferroxidasell), which have the capacity to oxidize ferrous ion (Fe+2) to ferric ion (Fe+3) the form of iron that can be loaded onto the protein transferrin for transport to the site of red blood cell formation [26]. Aims of the Study 1. Studing the antioxidant defense mechanism of reduced glutathione (GSH) as main non enzymatic antioxidant in patients with urinary bladder cancer and compared with control groups. 2. Studing the role of lipid peroxidation through studing the level of MDA as a biomarker of lipid peroxidation in patient with bladder cancer and control groups 3. Study the changes occuring in serum level of trace elements: zinc and copper in bladder cancer patients and control. Materials and Methods 1-Samples Two groups of samples were included in this study ,patients groups fifty patients(forty six males and four females) proved to have urinary bladder cancer admitted to Al-Hilla Teaching Hospital, and twenty five healthy persons considered as control groups. Five ml of blood was obtained from each subject , and was pushed slowly into plain disposable tubes with out anticoagulant. Serum was obtained by centrifuging 2500 rpm for approximately 10-15 minutes. 2-Methods . Determination of the serum reduced glutathione according to the Burtis and Ashwood method [27]. . Determination serum level of Malondialdehyde as biomarker of lipid peroxidation by reaction with thiobarbituric acid [28]. .Determination of serum level of zinc and copper through reaction of zinc and copper with chromagen reagent and the color intensity is proportion with zinc and copper concentration which determination by spectrophotometer [29]. Results and Discussion In this work the mean serum level of MDA among urinary bladder patients is 11.07 μmol/l and control is 3.048 μmol/ l and the results are as follows:- Table 1 The mean serum level of MDA in urinary bladder cancer patients and control groups groups MDA μmol/l SD P value patient 11.07 2.27 significant control 3.048 0.65 Concentration of MDA (umol/L) The differences between mean of serum level of MDA among patients and control groups as follows:12 10 8 Patients 6 Control 4 2 0 Patients Control Figure 2 Mean serum level of MDA between urinary bladder patients and control The mean of serum MDA according to the stages of bladder cancer are represented in table 2: Table 2 Mean of serum level of MDA according to different stages of bladder cancer group Stage l Stage ll Stage lll In this work there is significant difference in the level of MDA between urinary bladder cancer patients and control group. The serum level of MDA in UBC patients is 3.6 times more than that of the control, and there is increase of level of MDA with increase stage of cancer, the greatest MDA level are in stage lll MDA μmol/l 8.5 11.3 13.9 MDA has a mutagenic and carcinogenic role and causes mutation in DNA ,and when its level increases due to oxidative stress; this will lead to mutagenic and carcinogenic effects[30]. The mean serum level of GSH among patients is 4 μmol/l and control is 16 μmol/l ,and the results are as follows:- Table 3 The mean serum GSH in UBC patients and control Group Mean serum GSH μmol/L SD Patients 4 1.08 control 16 2.12 P value significant Concetration of GSH (umol/L) The difference in mean of serum GSH between UBC patients and control is represented in the bellow figure:20 16 15 Patients 10 5 Control 4 0 Patients Control Figure 3 The mean serum level of GSH in UBC patients and control. The mean of serum level of GSH according to the stage of bladder cancer are as follow. Table 4 Mean serum GSH in UBC patients according to the stage of cancer. Stage of cancer Stage I Stage II Stage III Mean of GSH μmol/l 6.5 3.9 2.4 In this study there is a significant difference in mean of serum GSH between UBC patients and control , p<0.01 , in bladder cancer the level of GSH is significantly reduced compared to control , the level of GSH is approximately 25% in bladder cancer patients compared to control and decrease more with the increasing stage of cancer. Decrease in GSH in UBC patients is due to continuous consumption of GSH by tumor cell , because in cancer state there is oxidative stress and accumulation of reactive species occuring and because GSH is concede red a master of antioxidant in the body through[31] . The serum level of zinc in UBC patients and control is as follows Table 5 The mean serum level of zinc in UBC patients and control groups groups Mean of zn μg/dl Patients 64.14 control 99.6 The mean of serum level of copper in UBC patients and control is as follow:- SD 4.2 8.6 P value 0.01 significant Table 6 The mean serum level of copper in UBC patients and control. groups CU μg/dl Patients 167 control 101 In this study there is a significant defference in zinc level between patients and control groups in UBC patients the serum level of zinc is significantly lowered than that in the control , p value < 0.01 , in contrasted to this result the serum level of copper is significantly elevated in UBC patients in relation to control, p value < 0.01 . The result of this study has indicated that the zinc is reduced and copper is elevated in bladder cancer state compared to control. SD 20 10.4 P value <0.01 significant Copper is one of the metal which has the ability to catalyzed formation of OH. And other radicals from H2O2 and O2.through Fenton reaction [32]. Zinc has antioxidant property through antagonism of redox active transition metal such as copper [33]. Zinc and copper are antagonized each other by competition between these metals in intestinal mucosal cell[34]. The correlation between MDA versus zinc and copper is as follows: Table 7 The correlation between the level of lipid peroxidation MDA via zinc and copper level in bladder cancer patients The correlation of MDA Correlation coefficient (r) μmol/L vs. Copper Cu μg/dl 0.775 Zinc Zn μg/dl -0.720 The correlation between MDA and copper in bladder cancer patients is positive significant (r = 0.775 ,p < 0.05 ),while the correlation between MDA and zinc level in bladder cancer patients is negative significant (r = 0.720 ,p <0.05 ) which means according to this statistical correlation in bladder cancer patients there is an increase level of copper which has oxidative power and cause an increase P value Positive significant Negative significant in lipid peroxidation with increase the level of MDA end product of lipid peroxidation , zinc level decrease in bladder cancer patients ,and because zinc has an antioxidant action this lead to accumulation of free radical which enhance the process of lipid peroxidation. The correlation between GSH versus zinc and copper as follow Table 8 The correlation between GSH via zinc and copper level in bladder cancer patients The correlation of Correlation coefficient (r) P value GSHμmol/L vs. Copper Cu μg/dl -0.681 significant Zinc Zn μg/dl 0.700 significant The correlation between GSH and negative significant (r =-0.681,p < 0.05 copper in bladder cancer patients is ),while the correlation between GSH and zinc level in bladder cancer patients is positive significant (r = 0.700,p <0.05 ) Conclusion 1.There is a role for lipid peroxidation in bladder cancer state due to oxidative state , so the level of malondialdehyde the biomarker of lipid peroxidation is significantly elevated 2.There is decrease in antioxidant defenses mechanism in bladder cancer state mainly glutathione. 3. Copper and zinc levels are disturbed in bladder cancer state copper level has oxidative property is elevated in cancer state while zinc level is decrease in bladder cancer . References 1. Boring C , Squires T 1994. cancer statistics . J clin. Cancer,44: 7-26. 2. Lars D , Torben F 2006. cancer epidemiology and prevention Cancer res . 66(3): 1851-1858. 3. Shuya H , Kelsey D , Carmen 2005 . Alteration p53 in human bladder cancer .J cancer. 104 (9):1918-1923 . 4. Roderick NM , Macsween K , Whaley A 1996. Muris textbook of pathology . 13th ed . oxford university press , new York. p 942-945 5 . Emil A , Jack W . smith's general urology 2000. 15th ed . Lebanon . p 357-358 . 6. Montiel j , Smith DL , Sandler H 2004. clinical oncology, 3rd ed,p 20592084 . 7. Robert W,Schrier MD, Carl W,Goottschalk MD1996.disease of kidney.6th ed..p.810-813. 8. Zeegers NP , Keller E , Buntex F 2004. Association between smoking consumption , diet and bladder cancer . World J . Urol . 21: 392-401 . 9. Sinko I , Monika M , Istevan R 2005. effect of smoking on DNA Damage .J Reproductive Toxicology . 20(1):65-71 . 10.Zeegers m , Swean G , Goldbohm P 2001. Occupational risk factors for bladder cancer .J. occup. Environ. Med.;58(9):590 596 . 11.Ripple M , Ray R , wilding G 1997. prooxidant and antioxidant Shift in human cancer j. Natl. cancer Inst.;89,10;40-8 12.Droge W 2001 . free radical and physiological condition of cell. J Physiol. Rev.;82:74-95 . 13. Han D , William E2001 . mitochondrial respiratory chain Generating super oxide anion . biochem .J .;353: 411-416 . 14. Yokoyama Y , Becham j 1990. xanthine oxidase potentiated ischemic injury . Am.J.physiol.;258:564-570 . 15. Amie k , Steven l , Petrson G 2005. Redox modulation and Xenobiotics action of ROS formation . toxicological,Science .;88(1):265-273 . 16. Peter G , Winnie j , Gorden P 2005. Molecular and biochemical Mechanism of reactive oxygen species . toxicology and Applied pharmacology.;207:354-366 . 17.Alexander n , spector A . 1994poly unsaturated fatty acid increase lipid radical .J lipid res.;35:1773-1785 . 18. Niederhofer j , Daniel S , Green R 2003. MDA a product of lipid Peroxidation mutagen to human cell . J.biological chemistry;278933:314330. 19. Nimet V , Rucken T 2004. Effect of stress indused lipid Peroxidation on cell function . International cell biology;28(7):517-521 . 20- Ulrike L , Terrance J , Kavanagh C 2001. gonadotrophine and Regulation of glutathione synthesis . reproductive, Toxicology .;15(5):495-504 . 21.Smith AF , Beckett GJ , Walker SW , Rae P, 1998. lecture notes On clinical biochemistry .6thed .Blackwell science ;p140. 22.Trung-tran AQ , Chai F , Z alewski PD 2000. role of zinc and cellular function . J.Nutr.;130:1432-1436 . 23.Bray TM , better WJ . 1990the physiological role of zinc 24.Emily H 2004. zinc deficiency , DNA damage and cancer risk .J of nutri. Biochem .;15(10):572-578 . as an Antioxidant Free radic Biol.Med.;8:281-291. 25. Christian P , West KP 1998;. interaction between zinc and Vitamin A .Am. J. clin. Nutr. 68:435-441 . 26.Caballereo b , Cousins RJ , Turnland JR 2006. copper .modern Nutrition in health and disease .10thed.philadelphia. lippincotts Williams&wilkins.;p.289-299 27.Burtis CA , Ashwood ER 1999. Tietz text book of clinical Biochemistery 3rded.Saunders company , Tokyo.; p.1034-1054 . 28.Burtis CA , Ashwood ER1999..Tetz text book of clinical biochemistry 3rd ed. Saunders company , Tokyo, 29.colorimetric determination of zinc and copper (kit) 30.Saad M , Nashed W , Husen M, Giebry M 2006. urinary telomere activity and MDA as marker of bladder cancer .Turkish J. of Biochem .;31(4):164-168 . 31. Guogao W , Sheng Y , Nancy D , Joan R 2004.glutathione and it is implication for health . J. of nutrition .;134:489-492 32. MichealD , Jonathan H. 2004. Copper and oxidative state .Am.J.physiol.cell.;286:293-301 . 33.BrayTM , B etter WJ 1990. zinc az antioxidant .free radic.Biol.Med.;8:281-291 34- KimikoH.Akria Y 1998.frre radical and trace elements.j. of trace element in experm.med.;11(20;209-217