In vivo mouse microCT - Michigan State University
advertisement

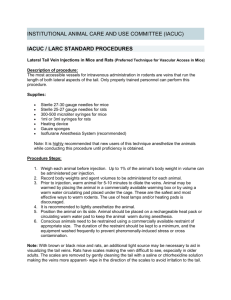
Michigan State University Institutional Animal Care and Use Committee STANDARD OPERATING PROCEDURE FORM THIS SOP MUST BE APPROVED BEFORE SUBMISSION OF ANY RELEVANT AUF Revision date: April 2013 DATE RECEIVED: APPLICATION NUMBER: 11/13-245-99 09/23/2013 DATE APPROVED: 11/03/2013 ROUND: AUF INACTIVE DATE: 1 1ST AMENDMENT DATE: ROUND: AMENDMENT APPROVAL: 3RD AMENDMENT DATE: ROUND: AMENDMENT APPROVAL: 2ND AMENDMENT DATE: ROUND: AMENDMENT APPROVAL: 4TH AMENDMENT DATE: ROUND: AMENDMENT APPROVAL: IMPORTANT -- ALLOW 4-6 WEEKS FOR APPROVAL THIS FORM MUST BE SUBMITTED AS A WORD FILE VIA EMAIL TO: iacuc@msu.edu or bauermo@msu.edu There is no expiration date for SOPs however they will be sent out for any correction/changes and re-reviewed by the IACUC every 3 years GENERAL INFORMATION PRINCIPAL INVESTIGATOR (As designated by Contracts & Grants) LAST NAME: Shapiro FIRST NAME: MIDDLE INITIAL: Erik M ZPID NUMBER: Z41345693 ACADEMIC RANK / TITLE: PRIMARY COLLEGE: Assoc Prof COM DEPARTMENT: CAMPUS TELEPHONE NUMBER: 884-3270 Radiology MAILING ADDRESS: FAX NUMBER: 846 Service Rd, Room 184, East Lansing, MI 48824 432-2849 NET ID: EMERGENCY NUMBER: Shapir86 203-631-1736 Title of Standard Operating Procedure Use of micro Computed Tomography (µCT) Scan for In vivo Studies on Mice Species: Mice Shapiro 11-13-245-99 1 DESCRIPTION OF THE STANDARD OPERATING PROCEDURE Micro CT System The GE eXplore Locus RS80 Micro CT Scanner is a pre-clinical x-ray computed tomography system designed for noninvasive imaging of small laboratory animals in vivo and for imaging in vitro specimens. This scanner is capable of imaging animals and specimens with a diameter of up to 40 mm in the transverse plane.[1] The detector consists of a scintillator linked via fiber optics to an 8-megapixel CCD and is capable of acquiring image volumes with 27, 45, or 90 µm isotropic voxel resolution.[1] The system employs a fixed tungsten anode x-ray source and cone beam scanner geometry to enable acquisition of a 33 mm section in a single rotation. The x-ray source is capable operating continuously at a potential of up to 80 kVp and a current of 500 µA. The scanner is certified by the vendor to be compliant with federal regulations regarding cabinet x-ray systems (21 CFR 1020.40 and FDA Report 0212775) and is designed to emit no more than 0.5 mR/h (equivalent to 4.4 x 10-6 Gy/h air kerma) at a distance of 5 cm from any exposed surface of the device.[1] Thus, incidental radiation exposure is minimal for both human operators and animals in the preparation area. The eXplore Locus Micro CT is located in room 3105 of the Biomedical and Physical Sciences building. Access to this room is restricted through the use of a key card reader door lock. Operators are required to have completed appropriate radiation safety training through EHS before using the device. Radiation Dose The radiation dose received by an animal or specimen in the micro CT is a function of the x-ray tube potential and current and the total time of exposure. When operated at an x-ray tube potential of 80 kVp, the entrance dose for an animal inside the µCT is 205 mR/mA∙s, which is equivalent to 1.80 Gy/mA∙s air kerma or approximately 1.95 Gy/mA∙s for soft tissue.[2] Image quality is dependent upon the photon fluence through each voxel of the imaged volume and, thus, is directly related to absorbed dose and inversely related to voxel size.[3] Accordingly, a variety of scan protocols will be used to achieve a suitable balance between the image quality required to visualize the phenomena of interest, the radiation dose that the animals can reasonably tolerate, the number of scans performed, and the recovery interval between scans. Some example protocols and corresponding dose estimates are shown below. The dose calculations shown do not include the dose for fluoroscopy, which is approximately 0.026 Gy, assuming a duration of 30 s. Potential (kVp) Current (μA) Exposure Time (ms) Isotropic Frames Voxel Size (μm) 80 450 200 92 2 80 450 200 92 2 80 450 400 92 2 80 450 400 92 1 80 450 400 92 1 80 450 400 92 2 80 450 400 92 3 80 450 400 92 4 80 450 200 92 2 80 450 200 92 3 80 450 200 92 4 80 450 800 46 2 80 450 1600 46 1 60 450 800 92 2 *Radiation dose measurements have not been performed at 60 dosimetry calculations. Views 720 720 400 360 720 360 360 360 720 360 360 200 200 360 kVp. FOV (mm) Bed Positions Dose Per Total Bed Position Dose (Gy) (Gy) 32.8 1 0.25 0.25 98.4 3 0.25 0.76 65.6 2 0.28 0.56 98.4 3 0.13 0.38 98.4 3 0.25 0.76 98.4 3 0.25 0.76 98.4 2 0.38 0.76 98.4 1 0.50 0.50 98.4 3 0.25 0.76 98.4 3 0.19 0.57 98.4 3 0.25 0.76 98.4 3 0.28 0.84 98.4 3 0.28 0.84 98.4 1 0.50* 0.50* The measurement at 80 kVp was used for these We will limit the total cumulative amount of radiation an individual mouse can receive over the duration of the experiments to 6.0 Gy with the caveat that this has the potential to affect biology in unexpected ways. Investigators, not Radiology staff, are expected to quantify and keep track of the total cumulative exposure, guided by the calculated doses in this SOP. Preparation of Mice for CT Mice will be brought to the CT preparation area in room 3105 of the Biomedical and Physical Science (BPS) building. There is a dedicated animal preparation area adjacent to the microCT. For some experiments, prior to scanning the mice, animals will be injected either retro-orbitally or via the tail vein with a contrast agent (see protocols below). The duration of time between the injection and scan is dependent on the type of contrast agent (4) and the structure of interest (5). After a Shapiro 11-13-245-99 2 determined time, dependent on the experiment and agent, mice will be placed into an induction chamber and anesthetized with 5%isoflurane in oxygen. Once anesthetized, mice will be moved to a nose cone and secured to a CT bed equipped with a respiratory monitoring apparatus in a prone position tail-first. The scavenging system has a local charcoal filter while the animal is on the bench and while the animal is in the µCT, the scavenging system is duct hose connected to a dedicated exhaust outlet. Protocol for Micro CT Scanning Operation of the micro CT scanner consists of a warm-up phase, positioning, and scanning. After powering on the system or after a period of inactivity, the operator must perform a warm-up of the x-ray tube. X-rays are emitted during warm-up. Therefore, the animal is not placed in the scanner until after the warm-up is complete to avoid unnecessary irradiation. After warm-up, the anesthetized animal is placed on top of a reference phantom on the scanner bed, a nose cone is placed on the animal to deliver an anesthetic and oxygen mixture, respiratory monitoring equipment is placed under the chest of the animal, and the animal is secured with a harness designed for this purpose. The operator will select the desired scan protocol. Fluoroscopy is used to adjust the bed position so the animal is located within the scanner’s field of view. Then the scan is performed. Finally, the animal is removed from the scanner, returned to a clean cage, and monitored during recovery. Protocol for Monitoring Anesthesia Anesthetic state is determined by monitoring respiratory rate on a monitor. Respiration rate is maintained between 30 and 60 breaths per minute and can be modulated by either increasing or decreasing the percent of Isoflurane in the mixture. Total cumulative amount of radiation an individual mouse can receive over the duration of the experiments The total cumulative amount of radiation an individual mouse can receive over the duration of the experiments is 6.0 Gy. Please be aware that this dose and even smaller doses, has the potential to affect biology in unexpected ways. Investigators, not Radiology staff, are expected to quantify and keep track of the total cumulative exposure, guided by the calculated doses in this SOP. Protocol for Tail Vein Injection (i.v.) in the Mouse [9]. A Mouse Tail Illuminator restraining device (Braintree Scientific Cat # MTI, see diagram A) is used to help warm the tail (allows for dilation of the blood vessels) as well as to illuminate the lateral tail veins (see diagram B, for location of the lateral tail veins). Select the mouse to be injected and place it in the tail illuminator restraining device with its tail in the illumination slot. Fill the 28-30 gauge needle and syringe with the agent to be injected. Rotate the tail to illuminate the lateral tail vein. Inject the needle bevel side up at the distal end of the tail i.e. furthest from the body. The full body of the needle does not have to be inserted into the vein just past the bevel of the needle is sufficient. Correct placement of the needle can be confirmed by feel i.e. the needle should advance smoothly into the vein. Once the needle is inserted, slowly inject. If the needle is correctly placed in the vein then it will become clear as the fluid progresses up the vein. If there is resistance and/or a blister/bubble appears on the tail then you are not in the vein. Remove the needle and re-insert it above the first site. Apply gentle compression to the tail to stop any bleeding. Once the bleeding has stopped return the mouse to a clean cage. The mice are monitored for tissue necrosis of the tail due to peri-vascular injection. The plan of care will be to contact ULAR for guidance. Acutely, animals will be monitored for inflammation and irritation, with anti-inflammatories given. However, once animals leave the µCT room, animal care is not the responsibility of the Radiology Staff, but rather the investigators themselves. Shapiro 11-13-245-99 3 Source: Hedrich H and Bullock G, eds; The Laboratory Mouse; Elsevier Limited, Amsterdam; 2004 Fig. A Fig. B Protocol for Retro-orbital Injection in Mice [9]. Retro-orbital injection is an acceptable alternative to the tail vein injection as a route for intravenous administration of material i.e. drugs, cells etc. Anesthesia is required for retro-orbital injection in mice. The injection volume should not exceed 100µl per eye. Although there is a 200µl maximum limit per eye. There is a limit of only one injection per eye per day. When more than one injection is required alternate between eyes, allow 1-2 days between injection sites. Do not exceed 2 injections per eye in a mouse. Procedure: Anesthetize the mouse using Isoflurane. Once anesthetizes place the mouse in lateral recumbancy (on its side) with the eye to be injected facing up. Retract the skin towards the body with the thumb and middle finger of the non-dominant hand. Use the index finger of the non-dominant hand to draw back the skin above the eye and the thumb to draw back the skin below the eye. The eye will protrude slightly. Insert the needle (27-30 gauge ½”) bevel up into the medial cantus of the eye at a 45 degree angle to the nose into the vessels behind the eye ball. There is a degree of resistance until the needle pierces the conjunctiva. The needle must be positioned behind the globe of the eye in the retrobulbar sinus not intraoccularly. There should be a flash of blood into the syringe when slight backpressure is applied to the plunger of the syringe. If the needle is placed too deeply or too aggressively the thin bone of the skull behind the eye can be pierced and the agent will be injected into the skull. There must be minimal movement of the needle once it is inserted into the retro-orbital plexus or the vessels will be ruptured causing bleeding and loss of the agent into the tissues behind the eye. Gently inject the agent into the retrobulbar sinus. Remove the needle gently to prevent injury to the eye. Close the eyelid and apply mild pressure to the injection site with a sterile gauze sponge. Monitor the mouse during recovery from anesthesia. Examine the injection site for swelling or other visible trauma. If no adverse effects are observed return the mouse to a clean cage. This will be performed except in the case of cell injections, in which case the anesthetic can potentially impact cell viability. This is guidance from Sandra O’Reilly and her experience with cell injections following whole body irradiation. We will do one injection per animal. Both Dr. Dorela Shuboni and Dr. Christiane Mallett, Research Associates in Radiology have been trained to perform retro-orbital injections. Shapiro 11-13-245-99 4 Carefully monitor the animal within the first 24 hours following injection and in the days following for any adverse health effects particularly swelling around the injection site, proptosis (bulging or forward displacement of the eye out of the orbit) of the eye or eye trauma, excessive grooming of the injection site or guarding of the injection site. Also monitor the general appearance of the mouse, note any changes in grooming habits, appearance of the skin/coat, or changes in the animals level of activity. Images adapted from www.iacuc.ucsf.edu section on retro-orbital injection in mice Adverse Health Effects of CT: Mice can readily recover from whole body exposures of 0.25 to 0.5 Gy per day.[3] The recovery rate is greater for partial body exposure and may be as much as 33% of the LD50/30 per day when only the lower body is exposed.[3] However, continued exposure may damage the recovery process. The rate of life shortening has been estimated at 7.2%/Gy.[6] The LD50/30, the threshold at which 50% of the population die within 30 days after exposure, for mice is 5.0 to 7.6 Gy, depending on age and on the resilience of the mouse strain to radiation exposure.[3] C57BL/6 mice have been shown to endure 3 scans per week with an average dose of 0.28 Gy per scan over the course of 6 weeks for a total dose of 5.04 Gy without any significant effect on pulmonary or myocardial tissue.[7] Another study demonstrated that C57BL/6 mice could endure 3 scans of the hindlimb with a dose of 0.434 Gy per scan with an interval of 2 weeks between scans without significant changes in bone structure, but 3 scans at 2 week intervals with a dose of 0.776 per scan induced some trabecular bone loss.[8] Doses ranging from 2.5 to 8.0 Gy have been shown to disrupt the activity of osteoblasts and osteoclasts.[8] Radiation exposure may cause cell death, DNA damage, cardiac hypertrophy, decreased LV systolic function, retarded growth, hematological abnormalities, bone loss, opportunistic infections.[7][8][9] The damage disproportionately affects the gastrointestinal tract and the hematopoietic system due to the mitotic activity of these systems.[9] In practice, due to the variability in the tolerance of different strains and individual mice to the effects of radiation, efforts to predict and prevent radiation-induced morbidity and mortality are imperfect. Therefore, daily monitoring is essential to ensuring humane treatment of the animals. Mice exhibiting at least two of the following external signs of radiation sickness or having a body condition score < 2 will be euthanized promptly:[9] scuffed coat (initially this is typically noticed around the neck/shoulder area i.e. the fur does not smooth down it appears to stand up/appear spiked, in more severe cases the whole fur coat is spiked as if the mouse was having an adverse reaction), closed eyes or eyes showing signs of discharge, hunched posture, lethargic/inactive i.e. doesn’t move when the cage is opened or try to get away when the researcher reaches in to pick up the mouse, moves slowly compared to a normal mouse labored breathing, diarrhea i.e signs of loose stool around the anus/base of the tail facial oedema i.e. swelling around the snout/cheeks anemia i.e. paleness of the tail or pads of the paws signs of weight loss (>20%) i.e. appear thinner than normal or compared to cage mates. Mice must be weighed 2-3 times per week. graying of hair coat. Black mice such as C57BL6 have been reported to turn gray after irradiation. Shapiro 11-13-245-99 5 References 1. eXplore Locus user guide (3rd ed.). (2006). London, ON: GE Healthcare. 2. Turner, J.E. (1995). Atoms, radiation, and radiation protection (2nd ed.). New York: Wiley-Interscience. 3. Ford, N. L., Thornton, M. M., & Holdsworth, D. W. (2003). Fundamental image quality limits for microcomputed tomography in small animals. Med Phys, 30(11), 2869-2877. 4. Willekens, I., Buls, N., Lahoutte, T., Baeyens, L., Vanhove, C., Caveliers, V., et al. Evaluation of the radiation dose in micro-CT with optimization of the scan protocol. Contrast Media Mol Imaging, 5(4), 201-207. 5. Ford, N.L., Graham, K.C., Groom, A.C., MacDonald, I.C., Chambers, A.F., & Holdsworth, D.W. (2006). Timecourse characterization of computed tomography contrast enhancement of an iodinated blood-pool contrast agent in mice using a volumetric flat-panel equipped computed tomography scanner.Invest Radiol, 41: 384-390. 6. Willekens, I., Lahoutte, T., Buls, N., Vanhove, C., Deklerck, R., Bossuyt, A., de Mey, J. (2009). Time-course of contrast enhancement in the spleen and liver with exia 160, Festra LC, and VC. Molecular Imaging, 11: 128-135. 7. Detombe, S. A., Dunmore-Buyze, J., Petrov, I. E., & Drangova, M. X-ray dose delivered during a longitudinal micro-CT study has no adverse effect on cardiac and pulmonary tissue in C57BL/6 mice. Acta Radiol, 54, 435441. 8. Laperre, K., Depypere, M., van Gastel, N., Torrekens, S., Moermans, K., Bogaerts, R., et al. Development of micro-CT protocols for in vivo follow-up of mouse bone architecture without major radiation side effects. Bone, 49(4), 613-622. 9. O’Reilly, S. A. (2012). Use of the X-RAD320 for studies involving whole body irradiation (WBI) of rodents with bone marrow/fetal liver cell transplant. Institutional Animal Care and Use Committee application 06/12-099-99, Michigan State University, East Lansing. Shapiro 11-13-245-99 6 DRUGS AND/OR AGENTS The drugs that are listed below MUST also be listed in the relevant AUF Drugs that are not pharmaceutical grade should be identified as such. The use of non-pharmaceutical grade compounds must be scientifically justified. In addition, if non-pharmaceutical grade compounds are to be used the PI should take precautions to maintain aseptic conditions and the drugs should be: • of the highest purity available • adjusted to ensure a pH level as close to neutrality as possible • constituted in a sterile solution for administration to the animal • kept in a sterile, sealed container after constitution for a limited period of time • administered with sterile syringes A1. List all drugs and/or agents that will be given to animals that will be used for this SOP. A permanent record of drug names, dosages, routes of administration, dates (times where appropriate) of administration, and initials of the person administering the drug must be maintained See “Surgical / Anesthetic Recordkeeping for Animals Used in Research and/or Teaching” at http://www.iacuc.msu.edu/policies_and_guidelines/IG007.pdf Anesthetics, Analgesics: Pre-operative and post-operative analgesia is required. Post-surgical analgesia is required for: 24 hours for minor surgical procedures such as placement of subcutaneous pumps, surgical implantation of catheters or castration; 48 hours for major surgery such as opening an abdominal cavity; 72 hours for potentially very painful procedures such as extensive orthopedic surgery, burns, thoracic surgery. If providing this will adversely affect your study, or if analgesia cannot be given at all, please give a scientific justification below. √ if not pharmaceutical grade Fill in both columns drug name(s) (generic only) Non-pharma grade route of administration frequency of administration duration of treatment (# of days or hours) volume dosages Isoflurane 1-5% In oxygen inhale constant 1 hour AuroVist (15nm) 100 μL /25 g 200 mg iodine/mL Retro-Orbital and Tail Vein Once per Scan Once ExiTron nano 1200 100 μL/25g 1200 mg iodine/kg Retro-Orbital and Tail Vein Once per Scan Once ExiTron nano 6000 100 μL/25g 640 mg iodine/kg Tail Vein Once per Scan Once Visipaque 320 500 μL/25g 83–105 mg iodine/mL Retro-Orbital and Tail Vein Once per Scan Once Omnipaque 300 300 μL/25g 300 mg iodine/mL Tail Vein Once per Scan Once Isovue® 370 100 μL/1hr 370 mg iodine /mL Tail Vein Once per Scan Once eXIA 160XL 150 μL/25g 160 mg iodine/mL Tail Vein Once per Scan Once Fenestra™ VC 125 μL/25g 50 mg iodine/mL, Tail Vein Once per Scan Once Fenestra™ LC 500 μL/25g 50 mg iodine/mL, Tail Vein Once per Scan Once Polymer encapsulated Bismuth nanoparticles 500 μL/25g 50 mg Bi/mL Retro-Orbital and Tail Vein Once per Scan Once Justify use of Non-pharmaceutical grade compounds: Polymer encapsulated Bismuth nanoparticles are being fabricated in the Shapiro laboratory and have the potential for clinical utility in CT. These will be made available to the research community at MSU but are non-pharma grade. They are reconstituted in sterile media and will be administered using sterile syringes. Please indicate any non-pharmacologic agents to be used to alleviate pain and distress X Warming Pad Fluid replacement X Other (Please specify): A2. Paralytics associated with this SOP Shapiro 11-13-245-99 7 Hiding places X Nesting materials Blankets drug name(s) (generic only) Dosages (range) Scientifically justify why you need to use a paralytic: Shapiro 11-13-245-99 8 route of administration frequency of dosages duration of treatment (# of days or hours)