Mozambique_National_Contingency_Plan
advertisement

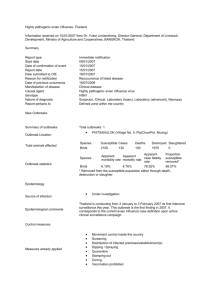
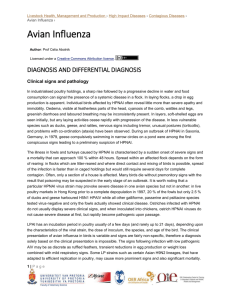
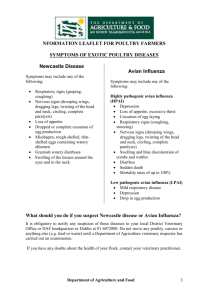
VERSÃO FINAL Draft of the English Version 2/16/2016 REPUBLIC OF MOZAMBIQUE -------------------MINISTRY OF HEALTH & MINISTRY OF AGRICULTURE CONTIGENCY PLAN FOR INFLUENZA PANDEMIC PREPAREDNESS AND RESPONSE: MOZAMBIQUE Mozambique, February 2006 APROVADO PELO CONSELHO DE MINISTROS A 2 DE MAIO DE 2006 [11 SESSÃO] FINAL VERSION FOREWORD The Avian Influenza is being spread throughout the world and the Health and Agriculture Organisations world-wide have already recognised the influenza pandemic as a serious world threat particularly to human health. As such, several countries are making tremendous efforts to prepare national contingency plans for combating the Avian Influenza as a way to minimise the negative impact of this pandemic (outbreak) which has reached our continent. Although Mozambique does not yet have focus of Avian Influenza but similarly to other countries, it intends to be prepared to mitigate all the evils and negative effects in social and economic sectors resulting from an outbreak of this type of disease. With this objective, the Ministries of Health and Agriculture of Mozambique developed the “National Contingency Plan for Combating Avian Influenza” which is being presented. The plan which is being presented includes a number of activities to be developed by different institutions and departments which by their nature play a key role in the prevention of infection or dissemination of virus, virus evolution follow-up activities and treatment (epidemiological surveillance; education and communication for health; research, clinics, laboratories, etc), before and after the pandemics. Therefore, the plan foresees among other objectives, the strengthening of epidemiological surveillance with laboratory determination of virus nature, as well as, daily follow-up of the situation. The prepared plan constitutes the first step for the integration and harmonisation of the country’ s response to the Avian Influenza, but at the same time, is a basis for dialogue and a strong tool for negotiation between the Government of Mozambique and the major co-operating partners which provide direct support to the State Budget or through SWAP. Through this current plan which is intended to be dynamic and should be updated whenever appear new data and elements appear and which could have implications in the scheduled activities, types of medicines/drugs and equipment to be used, vaccines, number of affected people or information which could enable to make an estimate of financial and human resources closer to the reality. APPROVED BY THE COUNCIL OF MINISTERS ON 02 MAY 2006 (11TH SESSION) 2 FINAL VERSION LIST OF ACRONMYS WB – World Bank CGA – Avian Influenza Commission CMAM - Central de Medicamentos e Artigos Médicos DAM – Medical Assistance Department DAG – Department for Administration and Management DDS – District Directorate for Health DEE – Department for Epidemics and Pandemics DNP – National Directorate of Livestock DPS – Provincial Directorate of Health DRH –Directorate of Human Resources DSA – Directorate of Animal Health DNP- National Directorate of Livestock EPI – Equipment for Individual Protection FAO – United Nations Organisation for Agriculture and Food GACOPI – Office for Co-ordinating Projects and Investments GT – Technical Task Force or Technical Working Group HCM – Maputo Central Hospital IEC – Information, Education and Communication INS – National Health Institute LCV – Central Veterinary Laboratory MoH – Ministry of Health MINAG – Ministry of Agriculture Mt - Metical NGO – Non-Government Organisation GSB – General State Budget WHO - World Health Organisation PROSAUDE – General Common Fund RESP – Office for Education in Public Health SIS – System of Health Information USD – American Dollars US – Health Facility ES – Epidemiological Surveillance APPROVED BY THE COUNCIL OF MINISTERS ON 02 MAY 2006 (11TH SESSION) 3 FINAL VERSION TECHNICAL WORKING GROUP – PREPARATION OF NATIONAL CONTIGENCY PLAN FOR PREPAREDENESS Ministry of Health Ana Charles (DSA) Eduardo Samo Gudo (INS) Moisés Wamba (DPC) Félix Malate (DAG) Diogo Paulo (RESP) Carla Silva, MD (DEE) Sandra Mavale (HCM) Aurora Siba-Siba (HCM) Ivo Fuigueredo (HCM) Brana Branquinho (CMAM) Ministry of Agriculture Ventura Macamo (DNP) Fernando Rodrigues (DSA*) Carlos Lopes Pereira (DAS*) Manuel Reis (IIAM) Inocêncio Sigaúque (DSA*) Adolfo Mavale (DSA*) Carlos Lopes Pereira (DAS*) AVIAN INFLUENZA COMMISSION Mouzinho Saíde (DNS) Avertino Barreto (DNS) Florencia Cipriano (DNAV) Ventura Macamo (DNP) Ana Charles (DSA) Ilesh Jani (INS) Rosa Costa (IIAM) Fernando Rodrigues (DSA*) Carlos Lopes Pereira (DAS*) Manuel Reis (IIAM) COLLABORATORS WHO USAID World Bank CDC Tecno Serve UNICEF APPROVED BY THE COUNCIL OF MINISTERS ON 02 MAY 2006 (11TH SESSION) 4 FINAL VERSION STRUCTURE FOR CONTIGENCY PLAN The current plan outlines the activities which should be implemented by several sectors previously defined fulfilling integrally the described chronological sequence. Only with an integral operationalization of all involved sectors and in due time, the defined objectives can be reached. Within this framework, the current plan was structured in order to facilitate and guarantee this integrated approach of the activities. This plan is comprised by 9 sections, namely: Section 1: Introduction - it contains a brief introduction of the problems with description of some important landmarks. Section 2: Objectives of the contingency plan contingency plan for Mozambique - are outlined on the major objectives of the Section 3: Background – there is a description of the phases preceding this plan. Section 4: Risks of Avian Influenza pandemic in Mozambique - Presentation of the real dangers for Mozambique by being affected by H5N1 virus taking into account that the country is located at the migration route of the migratory birds from the affected countries. Section 5: Impact Analysis on avian influenza in the fields of health and agriculture in Mozambique - are reported in-depth the burden of the disease in these two sectors. Section 6: Strategic objectives on the preparedness and response plan – are enlisted and described the major strategic objectives for prevention and response to avian influenza pandemic. Section 7: Annexes - are presented the calculation matrices where are described chronologically all the identified activities by the working group so that the defined objectives are reached. Matrix 1: it contains all identified activities by the sector of agriculture for prevention and erradication of bird diseases. Matrix 2: it contains communication, awareness-building and education activities. Matrix 3: it contains activities of health sector particularly on issues related to co-ordination, logistic and clinical management of the patients suffering from avian influenza. Matrix 4: it contains activities of health sector particularly on issues related to epidemiological surveillance, laboratory, data management and operational research. Each matrix has a header with the following items: Objectives Expected results Main activities – it contains the main activities to be implemented in order to reach the expected result. Sub-activities Pandemic phase - WHO has developed a system of terminology for several phases of a certain pandemic. Based on this, each activity should begin its specific pandemic stage. The passage from one phase to another is announced by the Director of WHO, and following all other corresponding activities related to the concerned phase are put in action. The evolution from one phase to another is guided by biological changes of the virus and through epidemiological characteristics of the disease at the international level. Responsibility – it is assigned to one or more people who should co-ordinate or implement the activity. Date of commencement and termination of the activities – it is necessary to indicate the month of commencement and end of the activity. Monitoring indicators – they are indicated the monitoring tools of the process. Budget for activity sustainability. APPROVED BY THE COUNCIL OF MINISTERS ON 02 MAY 2006 (11TH SESSION) 5 FINAL VERSION Funding Source Comments Section 8: Acknowledgements Section 9: Bibliographical references APPROVED BY THE COUNCIL OF MINISTERS ON 02 MAY 2006 (11TH SESSION) 6 FINAL VERSION TABLE OF CONTENTS 1. INTRODUCTION 2. OBJECTIVES OF THE CONTINGENCY PLAN 3. BACKGROUND INFORMATION 4. RISKS OF AVIAN INFLUENZA PANDEMIC IN MOZAMBIQUE 5. IMPACT ANALYSIS ON AVIAN INFLUENZA IN HEALTH SECTOR IN MOZAMBIQUE 6. STRATEGIC OBJECTIVES OF THE PREPAREDNESS AND RESPONSE PLAN 6.1. To reduce opportunities or risks of human infection by H5N1 6.2. To strengthen the Early Warning Systems 6.3. To create response capacity to the risk of the pandemic 6.4. To keep back or to delay the spreading of the pandemic in the source. 6.5. To reduce the morbi-mortality and social disturbance 6.6. To undertake operational researches on the pandemic 7. CONCLUSION 8. ANNEXES 9. ACKNOWLEDGEMENTS 10. BIBLIOGRAPHIC REFERENCES APPROVED BY THE COUNCIL OF MINISTERS ON 02 MAY 2006 (11TH SESSION) 7 FINAL VERSION 1. INTRODUCTION The highly pathogenic avian influenza was first identified in Italy in 1879, as an infectious disease of birds by Perroncito. Only in 1955, it was an agent characterised by Schafer as type A strains of the influenza virus. The influenza virus is a RNA segmented virus which does not have qualitative mechanisms of control during the replication and they are susceptible to changes. In the past, 3 avian influenza pandemics occurred, in 1918 (Spanish Influenza caused by subtype H1N1), IN 1957 (Asian Influenza caused by subtype H2N2) and in 1968 (Hong Kong influenza, caused by subtype H3N2). Conservative estimates indicate that mortality resulting from the pandemic in 1918 was of 20 to 40 millions, however more recent studies held in Africa and Asia indicate that the number of victims all over the world was of approximately between 50 and 100 millions people. During the last two years, in Southern Africa has been identified certain activity of avian influenza virus of H5N2 subtype which has been affecting only ostriches in South Africa and Zimbabwe. The type A avian influenza are perpetuated in nature in wild birds, predominantly in aquatic birds, on which there are 16 subtypes (which differs in approximately 30% in their structure which co-exist in harmony with its focus). In these natural focuses, the virus remains in evolutionary ecstasies, showing a minimum evolution in amino acids during long periods. After the transfer to new focuses, either birds or mammals, the avian influenza viruses develop rapidly. Although there are strains of the virus of low pathogenity in domestic birds and the disease does manifest in wild birds, the possibility of mutation can turn this virus to be highly pathogenic of H5N1 subtype, which occurred probably before 1997 in the South of China, reaching its enzootic state in domestic birds in South-east Asia and unexpectedly crossed the barrier of the species infecting mammals (cats, pigs and humans). Although, this event had its precedents, the substantial number of cases in humans, associated to a severe disease and various casualties arise serious problems on the pandemic potentialities of H5N1 strains. More evidences indicate that the virus H5N1 acquired major pathogenicity of H5N1 strain for various mammal species. To date (February 2006) 29 countries most of them from Asian continent, but also Europe and 2 from Africa (Nigeria and Egypt) reported sources of highly pathogenic avian influenza (H5N1). The sources in Japan, Malaysia and Republic of Korea were controlled successfully but the virus seems to be endemic in several countries affected. The outbreaks of Avian Influenza in Asian Southeast resulted in destruction of more than 150 millions of birds and had severe consequences for agriculture of the countries, particularly for rural families which depend on poultry of birds for their living and feeding. Recently (February 2006) in Nigeria more than 140000 birds were killed in a outbreak which the death rate reached more than 91% and 95% of the birds in risk respectively. The most recent sources of the same virus in birds in Russia, Kazakhstan, Turkey, Rumania, Croatia, Italy, France, Italy, Germany, Nigeria and Egypt show clearly that the virus spread besides the original source. THE THREAT OF AVIAN INFLUENZA PANDEMIC VIRUS H5N1 The estimates from experts indicate that the next avian influenza pandemic will cause probably more than 130 millions of patients, 2 millions of hospitalised people and 650,000 deaths in a period of 2 years. The impact will probably be more in developing countries. The avian influenza pandemic in 1918, in case being foreseen for nowadays it would have caused between 180 and 360 million deaths all over the world. The confirmed number of cases in humans till today 13 February of current year reached 169 with 91 deaths corresponding a death rate of 53,85% (table 1). APPROVED BY THE COUNCIL OF MINISTERS ON 02 MAY 2006 (11TH SESSION) 8 FINAL VERSION Table 1. Avian Influenza in Human between 2003 and February 2006 The number of cases in humans confirmed to February 13 of the average year reached the 169 with 91 deaths that translates the rate of fatality of 53.85% Accumulated number of cases in human of Avian Influenza 13 February 2006 Coun try Cambodja China Indonesia Irak Thailand Turkey Vietnam Total 2003 2004 2005 cases deaths cases deaths cases deaths 0 0 0 0 0 0 3 3 0 0 0 0 0 0 3 3 0 0 0 0 17 0 29 46 0 0 0 0 12 0 20 32 4 8 17 0 5 0 61 95 4 5 11 0 2 0 19 41 2006 Total cases deaths cases deaths 0 4 8 1 0 12 0 25 0 3 7 1 0 4 0 15 4 12 25 1 22 12 93 169 4 8 18 1 14 4 42 91 2. BACKGROUND INFORMATION This plan is a culmination of all activities that are being carried out by the members of the Preparatory Commission on Avian Influenza, established in 2004. This commission has been holding meetings once per week and defining strategies for combating this epidemics with assistance of foreign consultants (Strategic Plan for Veterinary) and with co-operation from WHO, USAID and World Bank. In January 2006, as it was deemed necessary, the commission started to work with assistance of the technical and operational group. The commission approved this decision, starting to work based on exchange of information, preparation of information of technical scientific nature and material for dissemination of messages as well as preparation of training kits to support the provinces. The participation of one member of the commission and two work group members at the preparatory meeting on avian influenza pandemic organised by WHO-Brazzaville constitutes a great opportunity to increase the level of knowledge and of understanding in regard to the threat that this disease represents. It also contributed for the exchange of information and experiences with experts of other countries which have already their approved plans. 3. OBJECTIVES This documents result from an intensive and joint work carried out by experts from Ministries of Health and Agriculture representing a final phase of consultation and discussion process in preparation for addressing the problem of avian influenza pandemics. It contains the main guidelines and intentions of the Government of Mozambique in regard to prevention and response to this pandemic which is eminent. APPROVED BY THE COUNCIL OF MINISTERS ON 02 MAY 2006 (11TH SESSION) 9 FINAL VERSION WHO has been insisting tirelessly that all countries should prepare a contingency plan for prevention and response to this eminent pandemic, warning that a careful preliminary work and the application of plans for a co-ordinated action are determinant factors for the response capacity to national or international health threat. Within this framework, WHO-AFRO organised from 12 to 13 February of this year, the First Regional Meeting in preparation for addressing avian influenza pandemics. In this meeting, there were defined the main objectives of African Region in relation to the prevention and response. Based on the defined objectives for African region and with some adjustments in accordance with Mozambican panorama, the objectives the current plan were as follow: Overall Objective: To reduce the morbi-mortality in case of emergence of bird flu and avian influenza pandemics and to minimise the social-economic rupture in Mozambique. Specific objectives: At national level, to provide a strategic platform as guide for any activities on prevention and preparation in Mozambican territory. To provide an instrument for discussion and rationale in the fund-raising activities at the local or international levels. To identify national priorities and define immediate activities. To secure that the activities are implemented in due time. To guarantee and facilitate a co-ordinated, integrated and multisectoral implementation in order to maximise the shortage of material and financial resources. To create capacity for prevention or eradication of diseases in birds. To create capacity for prevention or eradication of disease in humans. To create capacity for timely identification of cases in birds and in humans. To help to reduce the fear among the population, including the health care professionals, avoiding this way possible situation of total pandemonium. To guarantee a equality of allocation and distribution of available goods and funds. NB: Additional objectives are presented in the section on the strategic objectives of this plan. 4. RISKS OF AVIAN INFLUENZA IN MOZAMBIQUE There are 22 millions of domestic birds in Mozambique. Most of these birds are raised in small backyard flocks scattered throughout rural or periurban areas. Annually, approximately 7,8 millions birds are sold by commercial sector. Most than 50% of the birds in rural areas are raised in Manica, Zambezia and Gaza provinces, while great part live poultry whose activity is aimed to get profits is located in Maputo. (Picture 1). There is considerable growth of poultry industry (Avian industry) in Manica and Nampula provinces. Figure 1. Distribution of birds (birds and ducks) per province in general and of birds in the commercial sector in Mozambique. APPROVED BY THE COUNCIL OF MINISTERS ON 02 MAY 2006 (11TH SESSION) 10 FINAL VERSION Distribuicao de Galinhas e patos (% ) por provincia em Mocambique Producao de Galinhas no sector comercial (milhoes) 20.9 66.7 18.8 13.6 10.5 7.3 4.2 8.9 7.9 25.6 5.2 2.6 7.7 G az a a bé zia Za m an ic M Na m pu la Te te ba ne In ha m So fa la ss a C. De lg ad o Ni a ap ut o M 5.2 2 0.6 Nampula Manica Nº galinhas Maputo % * dumb duck or moscow duck One of the risk factors to be taken into account is the fact that Mozambique is part the major migratory routes of birds from Europe and Asia. Seventy and five (77) species of migratory birds visit regularly the country and some of them appear in large numbers leaving great quantities of excrements (picture 2). Relatively to other risk factors such as (I) human density (ii) bird density (iii) proportion of birds/humans (iv) presence of humid lands (v) pig density and besides the migratory routes which are into account, it is possible identify 4 regions of major risk (Picture 3) for the occurrence of the first cases of disease in birds and possibly in humans. In relation to domestic bird per inhabitant is variable in Mozambique being the same great, but provinces of Gaza (3,6:1), Manica (3:1) and Inhambane (1,5:1) and small in provinces of Nampula (0,7:1), Cabo Delgado (0,7:1) and Niassa (0.9:1). The areas of great risk identified based on the present factors are as follow: South of Cabo Delgado province and North of Nampula in coastal zone (ii). All Delta of Zambezi river (iii) the region of Urema Lago in Sofala province (iv). The intermediary coastal zones of Inhambane province and (v) Gaza and Maputo. Figure 2. Migratory routes, nº os species and Resting locations of migratory birds. 1 Quirimbas Lago Niassa 2 26 51 Pebane/Angoche 3 Gorongosa Delta do Zambeze Bazaruto 4 Inhambane Maputo/Inhaca/R.Elefantes 5 These areas require permanent visual and serological surveillance to detect the disease as soon as it appears and to undertake a rapid response in order to refrain the potential outbreak and to avoid its spreading. The visual surveillance should concentrate in identification and research of certain suspicion of avian influenza in live and dead domestic birds and in wild birds found dead. The serological surveillance should be concentrated in domestic birds near to the areas near to the areas APPROVED BY THE COUNCIL OF MINISTERS ON 02 MAY 2006 (11TH SESSION) 11 FINAL VERSION where there is probability of contact with wild birds (specially in aquatic and migratory birds) is more probable, i.e. near to humid lands, lakes and lagoons where migratory birds. Figure 3. Area with great potentialities for occurrence of first cases of avian influenza in Mozambique taking into account the most important risk factors. South of C. Delgado and North of Nampula Gorongosa, Urema Provinces of Maputo and Gaza Zambezi delta Bazaruto archipelago and coastal zones of Inhambane Table 2.Breakdown of domestic birds (chickens and ducks) and inhabitants per province in Mozambique Aves Habitantes 4.003.915 1.110.845 MANICA 3.164.998 1.046.448 INHAMBANE 1.730.276 1.159.142 MAPUTO 2.386.379 1.819.210 TETE 1.487.913 1.223.539 ZAMBÉZIA 3.598.650 3.107.146 SOFALA 1.444.698 1.368.432 NIASSA 762.345 804.960 C. DELGADO 1.028.476 1.384.531 NAMPULA 2.241.251 3.074.947 Total 21.848.901 16.099.200 PROVÍNCIA GAZA A/H 3.6 3.0 1.5 1.3 1.2 1.2 1.1 0.9 0.7 0.7 1.5 APPROVED BY THE COUNCIL OF MINISTERS ON 02 MAY 2006 (11TH SESSION) 12 FINAL VERSION RISK OF PANDEMICS IN MOZAMBIQUE It is well known in Mozambique that raising of petty animals particularly hens and birds, is a source for household consumption and income, mainly in rural areas where approximately 80% of the population live. On the other hand, being it an income-generating activity, entails the movement of the owners and their goods (chickens, ducks and birds) travelling from one place to another for selling/or exchanging with other items. Although to import birds being prohibited and therefore, hypothetically scarce the risk, Mozambique is one of important routes of migratory birds and, therefore, a risky zone. In Africa, the unique countries which avian influenza have been reported are Nigeria and Egypt, without identifying any cases of illness in human beings. Meanwhile, the epidemiological features of the virus show that the transmission is very rapid and efficient. The risk of pandemics affecting Mozambique is serious particularly if the occurrence of human cases persists, since the virus H5N1 can improve its capacity of transmission using man as its host. The fact that the respiratory failure on man being a predilect case of virus H5N1, of the rate of attack in other pandemics already described have been higher (25%-35%), of the main symptoms being common to resfriado, the severity of the cases being variable, the possibility of existence of asymptotic bearers and the migratory movement of the populations, are the factors which favour the spreading of the sickness. 5. IMPACT ANALYSIS ON AVIAN INFLUENZA IN THE HEALTH AND AGRICULTURE SECTORS IN MOZAMBIQUE The avian influenza has socio-economic effects highly negative and affects the results of the struggle against poverty. The negative impact of Avian Influenza can take a form of human deaths, bird deaths with a representative rate of casualties for the cases of commercial poultry superior to 90% which results in great economic consequences for the country. At social level, the existence of avian influenza reduces considerably the consumption of birds affecting this way the national economy due to mainly to the absenteeism in large scale and the domestic economy in particular since it is known that is household sector which has major concentration of birds for domestic consumption as well as trade as income-generating activity. The Avian Influenza can have socio-economic negative effects of the phase of evolution of the virus, therefore, all the contributing activities for the limitation of contamination to the humans will contribute for minimising the negative impact on the national economy. It is necessary therefore to concentrate all human, financial and material resources which could contain the spreading of the virus either among the birds or birds to humans and person to person. In case in which the virus become pandemics, the negative effects will be devastating implying losses of productivity, costs related to the acquisition of vaccines, anti-viral, equipment for individual protection in large quantities besides considerable human losses and consequently, a major allocation of resources will be demanded. Taking into account the threat that avian influenza represents at the national level, it is indispensable the involvement of several socio-economic stakeholders but, the Ministries of Health and Agriculture play a key-role as the lead-institutions in issues related to warning, health education, epidemiological surveillance, prevention and treatment. 5.1. ANALYSIS OF THE AVIAN INFLUENZA IMPACT IN THE HEALTH SECTOR In Mozambique, the lack of information on the quantity of drugs, equipment and necessary specialised technicians to contain the avian influenza moreover in its pandemics phase make it difficult to determine the financial resources to combating avian flu in case of occurring. APPROVED BY THE COUNCIL OF MINISTERS ON 02 MAY 2006 (11TH SESSION) 13 FINAL VERSION Being an emergency plan which is being drafted in 2006 to be response to possible situation which could happen perhaps during this year, there is a need to mobilise a set of resources which are not foreseen in on-going plans but which are necessary to give response to this situation. Additional funds will be requested either to the Government of Mozambique or to other co-operating partners which are working in the health sector in Mozambique. In the worst, in a very unpredictable hypothesis, the available funds and scheduled in plans of health sector in the implementation in detriment of several activities of routine but also extremely important and indispensable in the struggle against the burden of illnesses which affect our economy. That could be a significant setback in the struggle against extreme poverty defined by the Government of the Republic of Mozambique. The table below shows that for the current year, the total of funds foreseen for the health sector is totalling an amount of 248,056,679 millions American dollars corresponding an increase rate of 15% compared with previous year. In case there is outbreak of this pandemics during this year and supplementary financial resources are not allocated, the Ministry of Health will have to allocate the unique funds on which it has a control which are of approximately 200 millions American dollars (Common Funds + State Budget) once the Vertical Funds are not controlled by the Ministry. But, in case the pandemics does not happen during this year, the necessary funds to fund this contingency plan could be scheduled for the plan of 2007 to be prepared in the planning cycle 200607 starting in May of this year. Thus, if this is like this and assuming that an a growth of funding of the sector will maintain (from 2005 to 2006 was of 2%), given the trend of the co-operating partners of the country providing direct support to the State Budget, the Ministry of Health will have to in its exercise of planning allocate the necessary funds to combating against the flu. Table 3: Total of Funds for Health Sector in 2005 and 2006 Moeda: US$ Fonte Orçamento do Estado Fundos Comuns Fundos Verticais Total 2005 104,117,714 112,866,835 122,808,546 339,793,095 2006 108,200,514 98,400,944 141,455,221 348,056,679 Evol. 4% -13% 15% 2% 5.2 IMPACT ANALYSIS OF AVIAN INFLUENZA IN THE AGRICULTURE SECTOR More than 2 millions of people are by certain or other ways linked to production of chickens in rural areas (medium size = 10 birds). There are 1,000 aviaries of medium size=600 birds) and 12 aviaries of great dimensions (medium size = 200000 birds). The medium value of one chicken is of 67,000 Mt (US$ 2.68). The total amount of the poultry industry is of approximately US$ 75 millions (picture 2). Figure 4. Number of poultry producers, number of birds and value of poultry industry in Mozambique Produtores de Galinhas e No. de galinhas por sector Valor da industria avicola em Mocambique 73.2 Preço médio 68,300=US$2 19.3 Total=0.3 PIB 52.7 Preço médio 65,900=US$2 .6 2 2 0.6 0.1 Familiar Pequena escala Produtores 27.1 20.5 19.3 7.8 0.00012 Comercial Familiar Pequena Escala Total Galinhas nº galinhas Valor APPROVED BY THE COUNCIL OF MINISTERS ON 02 MAY 2006 (11TH SESSION) 14 FINAL VERSION An outbreak of great proportions could cause damages of approximately US$ 50 millions and with great probability of occurrence of illnesses in humans. Once there is no other method besides killing of the infected birds and in risk to refrain the dissemination of the disease, it would be necessary more than 750 people/per month and an investment of approximately US$ 300,000 to undertake the work. The destruction of more than 8000000 millions of birds would be nightmare from logistical point of view being necessary to compensate with more than US$ 20 millions to the poultry producers affected. Figure 5. Economic losses in the worst scenario (3 affected provinces with emerging commercial aviculture and rural aviculture). Perdas economicas (no pior cenario) aprox. US$ 50 milhoes 47.3 21.8 17.8 5.7 2 Perdas em animais Perdas em lucro (familiar) Perdas em lucros Perdas nas (comercial) industrias de racao Total With the evolution of events with other sectors like Education, Culture, Finance, Industry and Commerce, Tourism, Women and Social Affairs, Home Affairs, Defence, Labour, Foreign Affairs, Transports and Communication as well as associations, institutes and NGOs will be called upon to provide their contributions in relation to the impact of this disease in their sectors in order to enable us to have the real impact on the country’s economy, which is foreseen to be of catastrophic proportions. 6. STRATEGIC OBJECTIVES OF THE PREPAREDNESS AND RESPONSE PLAN 6.1 REDUCE THE OPPORTUNITIES OF HUMAN INFECTION BY H5N1 VIRUS The probability of avian influenza transmission to human can be reversed in case that the control of occurrence of the disease in birds is effective. In this way, a National Strategy for Prevention, Control and Eradication of Avian Influenza (ENPCEIA) which guides the preparation and the response to (I) avoid the entrance of virus of IA in Mozambique through animals and animal-made products, (ii) stop, refrain ou limitate the dissemination of the disease from birds to human beings. The pillars of this strategy are as follow: 1. Prevention 2. Detectation, communication and early reaction. APPROVED BY THE COUNCIL OF MINISTERS ON 02 MAY 2006 (11TH SESSION) 15 FINAL VERSION 3. Vigilance and diagnostic. 4. Containment and eradication. 1. Prevention – Application of the legal procedures of import and fiscalization in borders. Prohibition, import of alive birds ou their products of infected regions or countries. – Improvement of the bio-safety of aviaries through the application of Standardised Operational Procedures (SOPs) in the industry and the home-made of raising birds. – Review and if necessary to change the methods of raising which increase the risk of introduction and/or dissemination of Avian Influenza (AI). – Prohibition of simultaneous raising of pigs and birds at the same establishment/place. – Education of population in order to avoid accidental contact with sick or dead birds and to increase the distance between them and the birds in the home-made systems of raising animals. 2. Communication Detection and rapid reaction – Dissemination of information to the public in general in urban and suburban areas in relation to safe practices to deal with sick or dead birds, communication of suspicious occurrences and on elimination of the carcasses. This will be carried out through the intense use of media, extension networks, non-government organisations, leaflets and pamphlets in national languages. – Dissemination of information to industry (Aviaries of medium and big size and ration producers) on bio-safety in the aviaries in form of SOPs for production and safe handling of birds, communication of the occurrences and safe elimination of the carcasses. – Creation of Standardised Operational Procedures (SOPs) for reaction in case of suspicion of disease case/focus. – Creation of 11 teams (1 national and one per province) to undertake a research of suspicious cases, situational evaluation and containment of the focus. – To develop Awareness-Building Programme of the Community with the objective to reach the capacity of early detection and sustainable state of warning in rural areas. – To develop a control mechanism of the process through the creation of an Operational Centre. 3. Surveillance and Diagnostic - - Visual and serological surveillance in 4 identified areas as of greater risk (I) active serological surveillance in relation to domestic birds and improvement of the diagnosis of bird diseases, through the increase of samples sent to laboratory including wild birds found dead. Improvement of the laboratory diagnosis, through the refinement of diagnosis methods and techniques and improvement of bio-safety at the Central Veterinary Laboratory. Establishment of the co-ordination with the reference laboratory and with regional laboratories (Kenya and South Africa) para virulogical diagnosis of Avian Influenza and appropriate mechanisms for shipping samples to those laboratories. To develop a community-based-programme of surveillance based on training extension workers and community-based workers with the objective to create a proactive attitude in the detection and communication of suspicious cases of diseases to be Avian Influenza. To train all veterinary staff in Avian Influenza, detection, collection, handling and shipping of samples and safe handling of birds and carcasses. 4. Containment and eradication In case of confirmation of Avian Influenza, the subsequent activities will be under the responsibility and command of the Head of Department of Animal Health and the Government of Mozambique will make every effort to carry out the activities for immediate containment and eradication of the focus at the place of occurrence. This activity will comprise the slaughtering of birds in a radium of 3.5 km APPROVED BY THE COUNCIL OF MINISTERS ON 02 MAY 2006 (11TH SESSION) 16 FINAL VERSION and the establishment of surveillance zone of 10 km in relation to the focus epicentre, in which foreseen measures in the law will be applied. This will be carried out by trained teams and with the appropriate equipment for protection of personnel. The elimination of carcasses and decontamination will follow slaughtering of birds by human and it will be carried out in a safe manner and in environmentally acceptable conditions. The containment measures will include the temporary suspension activities in markets where the birds are sold or their products in authorised locations or informal markets after the detection of the first case of bird flu. This measure will be lifted after 21 days if all bio-safety measures have been carried out. The Government of Mozambique will compensate all individuals affected in kind (replacement of birds) or financially based on the price practised for each bird at the local market. In this moment, a group is working in a proposal of regulation for compensation mechanisms. Prohibiting measures for exporting birds and its by-products from affected countries by bird flu are being implemented in our countries. Institutional and legal framework for the establishment of a national strategy for prevention of Avian Influenza, in birds in Mozambique The State Veterinary Services currently represented by the National Directorate of Livestock (DINAP) is a Veterinary Authority responsible for epidemiological surveillance and for controlling diseases affecting animals. The response capacity of this institution and of representatives of Veterinary Authority in provinces (The Provincial Services of Livestock and District Services for Agriculture) will play a determinant role in control prevention and eradication of Avian Influenza. To face a contagious and epidemics disease of economic importance and in public health is necessary that the Veterinary Authority should have a chain with clear leadership, scientific capacity and infra-structures (material and human resources) to carry out their diagnostic activities, epidemiological surveillance, control and eradication in animals. This responsibility was established by the Council of Ministers´Decree nº8/2004 dated 01 April. The global strategy of prevention of Avian Influenza established by World Health Organisation (WHO) and by its counterpart World Organisation of Animal Health (OIE) as well as by the United Nations for Food and Agriculture Organisation (FAO) is aimed to avoid the occurrence of diseases in animals and this way, preventing the possibility for transmission to the man. The Veterinary Authority at the different levels need to work in close co-operation with the Ministry of Health, partners in Industry, private sector, private veterinarians and other professionals involved in animal production and with producers in general towards reaching the success in their interventions and as the control measures will have great impact in poultry industry, in producers and consumers of poultry products. It is extremely important to recognise that the Veterinary Authority in Mozambique is presently fragmented and has weak chain of leadership being very far of reaching the internationally minimum standards established by OIE and FAO. In this context, the on-going reforms in the country should take into consideration the need to safeguard the non-fragmentation of the veterinary authority competencies Scenario for the implementation of the Mozambique Contingency Plan for Influenza Pandemic Preparedness and Response (ENPCEIA) To refrain/contain a such harmful disease for the human health and with great economic impact, the Veterinary Authority at the national and provincial level, has to be organised, well equipped with human and material means, and under unified and capable leadership to decide, co-ordinate and implement the measures of control prevention and eradication under ENPCEIA in accordance to the law. For such effect, it is necessary and urgent: APPROVED BY THE COUNCIL OF MINISTERS ON 02 MAY 2006 (11TH SESSION) 17 FINAL VERSION a) To implement the principles and dispositions foreseen in the Regulation of Animal Health/Sanity (Decree 8/2004, 1 April) which confer power for application of the established norms in the same diploma. b) To strengthen the vertical command of the Veterinary Authority making that all Heads of Provincial Services of Livestock (representatives of Veterinary Authority) so that they can be responsible for addressing issues related to ENPCEIA and other diseases of compulsory declaration and of national and regional importance, are directly under the National Director in accordance with the national interests and international standards. c) To guarantee that the Provincial and District Governments provide all necessary collaboration and support for the fulfilment of the Regulation of Animal Sanity and implementation of the ENPCEIA. d) To secure that Central Laboratory of Veterinary (IAAM) undertakes the diagnostic work in birds in accordance to the priorities and locations established by Veterinary Authority. e) To secure that the National Directorate of Agrarian Services, is reinforced through human an material means to implement ENPCEIA and the programmes of Prevention and Control of Diseases of Compulsory Declaration. f) To guarantee the availability of funds for the implementation of activities related to the proposed strategy and its desimbursement is made very rapidly. 6.2 TO STRENGTHEN THE EARLY WARNING SYSTEMS AND CREATE THE RESPONSE CAPACITY TO THE PANDEMICS In case of outbreak of pandemics, the country should be prepared to: - Detection of the case Surveillance and Notification/Reporting Epidemiological Research Operational Research Strengthen the evaluation of risk Strengthening of capacity building Advocacy and international partnership Creation of a Multisectoral Forum Establishment of a multisectoral team with the participation of the following Ministries and sectors: - Ministry of Health - Ministry of Agriculture and Fisheries - Health National Institute - National Institute for Veterinary Research - Ministry of Science and Technology - Bio-Technology Centre - Faculty of Medicine - Faculty of Veterinary - Ministry of Finance - Ministry of Industry and Trade - Ministry of Foreign Affairs and Co-operation - Ministry of Tourism - National Institute for Disaster Management (INGC) - Mozambique Association of Avicultors APPROVED BY THE COUNCIL OF MINISTERS ON 02 MAY 2006 (11TH SESSION) 18 FINAL VERSION - Association of the Poultry keepers from Mozambique - Association of Consumers - Mozambique Red Cross Relevant activities To improve the detection of the case in man - To activate provincial and district nucleus of response to the epidemics (already existing) - To provide in due time financial resources - To create conditions for isolation of patients - To create conditions for collection, reception and shipping of samples to the laboratory of reference - To create conditions for registration, reporting, minimum analysis of data and feed back - To implement clinic surveillance of the cases (clinic and laboratory diagnostic) - Recruitment of human resources - Necessary equipment (cirurgical medical material, laboratory, equipment for bio-safety, drugs, etc.) including prophylactics for clinical staff. - Necessary equipment (surgical medical material, laboratory, biossegurança equipment, medications, etc.), including prophylactics for personal clinical - Take into account the Cholera Treatment Centre (CTC), tents, etc. - Prepare logistical conditions - Create conditions for notification of the cases “rapid cases” (telephone, fax-e.mail, radio) - Training of all staff involved in the activities of prevention and control of the disease. - To guarantee water and light - Treatment of corpses - Garbage Handling - Treatment of the garbage - Transport Advocacy and international collaboration The search for external support is fundamental in this phase. We must promote and take part in meetings which will enable us to increase our knowledge in this matter and to exchange information and experiences and to find potential partners. Clinical Treatment of the patients The avian flu can be described as an epidemic event characterised by world circulation of a new influenza virus for which the population has less or none immunity, resulting in higher morbimortality. When the epidemic happens is extremely important to have the capacity to evaluate its extension and possible progression/evolution to the epidemics. APPROVED BY THE COUNCIL OF MINISTERS ON 02 MAY 2006 (11TH SESSION) 19 FINAL VERSION The basic cares consist on individual or collective work, located at the primary level in the National Health System (NHS), with the objective to promote health, intensify the prevention, treatment and the rehabilitation/recovery. To face an epidemic, it is necessary to: 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. Prepare a functional fluxogramme for the patients in health units. To acquire EPI for the Service Staff Provider of medical cares and medicines; Training of trainers in issues related to the treatment of patients and bio-safety Training of clinic staff in the whole country in issues related to the treatment of patients and bio-safety. Identification of infra-structures for the isolation of cases. Provision of EPI, hospital equipment and diagnostic methods for rapid distribution in Health Centres in case of need. To prepare attendance norms to the patient suspicious of being affected by H5N1. Purchase in due time of Tamiflu or Relenza for high risk groups. Purchase in due time of seasonal vaccine for high risk groups. To acquire other supportive medications for combating the pandemics. To prepare a distribution plan of equipment, anti-viral and vaccines. To acquire vaccines against pandemics virus for high risk groups. To vaccinate the high risk groups. Institution of appropriate treatment to all suspicious cases and its contacts. For the successful control of pandemics, surveillance activities in humans, complemented with information and education for health (health promotion and disease prevention) should be intensified targeting to the population in general and to high risk groups. Early warning System In case the country is affected, the epidemiological surveillance should be based in rural zone, since most of the cases occur in this zone. On the other hand, the early detection of cases will be complicated due to higher prevalence in population (the same which is occurring in other countries) of other respiratory diseases presenting the same symptoms particularly, where the prevalence of HIV/AIDS associated with lung tuberculosis or pneumonia is higher. 5 sentry posts should be established, namely: (1) Pemba Provincial Hospital, (2) Provincial Hospital of Quelimane, (3) District/Rural Hospital of Manica, (4) District/Rural Hospital of Vilanculos, (5) Maputo Central Hospital (reference). The ideal is to treat the patients on the site. The reporting system should be set up so that the surveillance is done at the same time in animals and in humans. The use of “rapid way” is fundamental. All the available means of communication should be used for the exchange of information. It is important to establish a programme of weekly report on the evolution of the bird flu with the support of information organs. Experiences of the affected countries show that many activities defined in the plans of response to pandemics are activated due to the changes. The detection of these changes and the interpretation of its meaning depends if the clinical-epidemiological and virulogical data are opportune and safe. To every human case, it will be necessary to undertake an evaluation of risks. The public health laboratory has a central role in the early warning system. It is a strong assistance for active and passive surveillance of the disease in humans whose role é to secure the confirmation and early identification of the subtype and viral race from clinical samples. Active search of cases in humans - Identification of focal points (They do exist for epidemiological Surveillance) - Definition of the CASE APPROVED BY THE COUNCIL OF MINISTERS ON 02 MAY 2006 (11TH SESSION) 20 FINAL VERSION - Identification of high risk population groups - Preparation of reporting form for research based on the CASE - Preparation of registration book - Computer processing of all information (collection, analysis, interpretation, report) - Mapping - Establishment of a system for rapid and safe transport of samples - Control of borders, contact with authorities of neighbouring countries - Training of joint team (for active and search and research of the case) - Recruitment of activists and identification of focal points in the community (active search in the community) - Definition of the periodicity of active search - Search and identification of contacts - Prophylactics of the contacts - House Desinfection - Information, education and communication to the populations (IEC) - Training Strenghtening of the national centre for Avian Influenza in prone-risk areas (regions) A surveillance system for avian influenza virus was set up at the HCM paediatrics services and the laboratory of microbiology of the Faculty of Medicine. - To evaluate the activities, existing material and human resources; - To create conditions for the submission of request of support to WHO for what could be deemed as necessary, especially in equipment, training of personnel and reagents for diagnosis. Laboratory In spite the fact that the country has certain experience in giving prompt response to the emergency situations, in terms of epidemiological surveillance, treatment of cases, etc., although, with scarce resources, the difficulties are enormous relatively to the laboratory capacity in replying rapidly in case of emerging of new diseases. Tests of diagnosis for detection of H5N1 virus are technically difficult and very costly. They require very sophisticated equipment associated to the needs of material and special precautions of bio-safety in collection, handling, shipping and laboratories processing of the samples. Every laboratory activity for handling and testing of samples will be done exclusively by the Unit of Virology Laboratory of Immunology of the INS which must have the capacity for such purpose. The collected samples of suspicious individuals must be sent to the INS Immunology Laboratory fulfilling the required bio-safety requirements. For such purpose, it is necessary to update the budget to upgrade the level of bio-safety of veterinary and health laboratories in order to be at the level to provide response to the complexity required for the detection and handling of the avian influenza. The other useful measure would be the establishment of co-operation relations with other laboratories of the world (Vietnam, Cuba, Brazil and France) which have experience in handling samples of avian influenza virus. Creation of the capacity for detection of H5N1 Virus APPROVED BY THE COUNCIL OF MINISTERS ON 02 MAY 2006 (11TH SESSION) 21 FINAL VERSION The capacity of the laboratories to secure the detection and early confirmation of the pandemics virus constitutes the key-factor for surveillance activity. Now, Mozambique does not possess the laboratory capacity for the identification of H5N1 virus. The development of the capacity for laboratorial confirmation of suspicious cases is comprised by 2 phases, namely: Phase 1 – Upgrading the capacity of the Unit of INS Immunology Laboratory in bio-safety for the manipulation of clinical samples for the shipping to the CDC Reference Laboratory-in Atlanta In the first phase, the identification of H5N1 virus will be made in CDC-Atlanta. The samples received by the Immunology Laboratory will be later sent to the CDC Reference Laboratory-in Atlanta. For such purpose, capacity and conditions should be created, including: Physical reforms of the Virology unit of the INS Immunology Laboratory Purchase of equipment Creation of an effective and safe system for sending the samples to Atlanta through the circulation with companies carriers. Training of 2 researchers in Atlanta in bio-safety procedures of level III, including collection, handling and sending of samples. Phase 2 – Upgrading the capacity of Virology Unit of the INS Immunology Laboratory for identification of H5N1 virus through the PCR technology in real time. At the second phase, capacities for identification of H5N1 in Mozambique should be created at the Virology Unit of the INS Immunology Laboratory. With the area of virology previously created at the phase 1 of development of capacity, all the resources must be mobilised for installing PCR technology in real time. The require prerequisites for this phase are: Purchase of equipment which includes PCR machine in real time “open” Purchase of reagents for the PCR reaction and kits for extraction of genetic viral material (RNA). Purchase of material for isolation of sequence specific viral. Training of 2 researchers of the Virology Unit of the INS Immunology Laboratory in specific issues of PCR in real time and bio-safety. In parallel to this activity, the training of laboratory technicians throughout the country in the field of collection, handling and shipping of samples to the laboratory is fundamental. Meanwhile, even after installing the capacity for laboratory diagnosis in Mozambique, the periodical and systematic shipping of samples to the WHO reference laboratory in Atlanta, it is important due to following reasons: To undertake more specialised tests for surveillance of recombination ou mutations. Extraction of antigens which could be included in “pool” for the manufacturing of vaccines so that the produced vaccines are effective against circulating virus in the region. A system of management, analysis and sharing of laboratory data will be set up in order to enable a rapid exchange of information and laboratory data with WHO and the affected countries. 6.3 TO REFRAIN OR DELAY THE SPREADING OF THE PANDEMICS IN THE SOURCE While the world still waits for the appearance of effective vaccine against viral gene responsible for the next pandemics, countries like Mozambique should be more aggressive in preventive measures APPROVED BY THE COUNCIL OF MINISTERS ON 02 MAY 2006 (11TH SESSION) 22 FINAL VERSION for refraining ou delaying the spreading of the pandemics. The prophylactics with anti-viral drugs seem till now fundamental measure in the medical field. However, it is necessary to pay attention to the fact of being necessary to vaccinate 80% of the population within three weeks from the first clinical case of infection by pandemics virus till reaching a protective immunity. To enable that such measure is successful, it should be combined the massive administration of supportive medications as well as through the implementation of an adequate quarantine service. Therefore, the great limitation of this strategy is the lack to date of vaccines and anti-viral drugs in enough stocks. The pillars of this strategy are as follow: – – Establish a National Stock of Anti-Viral Drugs To develop a distribution plan for rapid and effective distribution of drugs Establish a National Stock of Anti-viral Drugs The Ministry of Health through the CMAM should make a prevision of necessary drugs to challenge the pandemics and to make the identification of potential suppliers, acquisition and purchase of the medications in enough quantities. In addition to this, the logistic capacity should be installed or strengthened to guarantee that the first group of people affected have access to medication in first hand. To develop a rapid and effective plan of distribution of drugs Mozambique is a country with long experience in massive distribution of medications and medicalcirurgical equipment in emergency situation as well as vaccines in vaccination campaigns, (Smallpox, Measles, Poliomyelitis,). However, in case of pandemics, this experience should be adapted to meet the needs to address duly with the distribution of anti-viral drugs whose transportation and administration should comply with more complex criteria and standards. 6.4. TO REDUCE A MORBI-MORTALITY AND SOCIAL DISTURBANCE The administration of vaccines (first line of defence) and anti-viral drugs constitute the most important medical interventions to reduce the morbi-mortability during of an eventual outbreak of pandemics. As the availability of vaccines will be null or limited, the anti-viral drugs have the critical role in the inception of the pandemics. On the other hand, the role of the government institutions in the introduction of non-medical interventions to reduce the morbi-mortality and social disturbances is very important, taking into account the inappropriate destruction of vaccines and lack of equity of its access. Notwithstanding the fact that the scientists not being capable to determine with exactness the time horizon and the gravity of the next pandemics, the history shows that it appears in explosive manner causing a large number of patients, dead, stoppage of public services and lost of productivity and of economy. The health services must be prepared to give response to great demand of intensive care services and to accommodate great number of deaths resulting from this pandemics. The ever increasing rate of absenteeism in all sectors of labour force will have disastrous consequences in the provision of health, security, transport, social and telecommunication services. For the experience acquired in past pandemics, the demand for installing services of rapid response to pandemics will not be throughout the whole country at the same time which will enable to the stakeholders to act in order to refrain the spreading of the disease from one region to another. An APPROVED BY THE COUNCIL OF MINISTERS ON 02 MAY 2006 (11TH SESSION) 23 FINAL VERSION important measure to minimise the devastating impact of pandemics of the pandemics, it will necessary to guarantee an adequate nutritional support, measures of hygiene and medications to treat the opportunistic infections. This strategy is based in: Monitoring Introduction of non-pharmaceutical interventions Use of anti-viral drugs for high risk population groups Supply of vaccines Equity in the access of vaccines Communication of the risks to the public Monitoring With the technical assistance of WHO, the national team of experts will undertake monitoring activities to detect early the epidemiological and clinical behaviour of the new viral focus in real time. This activity will enable to obtain the information on the main target population groups, virulence, severity of the disease, rate of attacks, the risk for the health workers and the mortality rate. The monitoring allows also to determine if the sintomatology is caused by the primary viral pneumonia ou secondary bacterial pneumonia which answer to the antibiotics. A monitoring enables to forecast the trend of disease in a most realistic way. Introduction of non-pharmaceutical interventions Some measures such as closing of schools, quarantine, banning concentrations of people or to impose restrictive measures of travels which could be useful to avoid that the virus is rapidly and uncontrolled disseminated. Use of anti-viral drugs for high-risk population groups WHO recommends that the countries which have financial and logistic means to invest towards having an enough stock of anti-viral drugs particularly to face the pandemics. Supply of vaccines In this moment the vaccine is not available in enough quantities for the whole world. This causes limitations on the development of activities of the countries in terms of logistical organisation, storage so that they can be prepared in time to face the eventual pandemics. Equity in the access of vaccines As a country, we need to think in a balanced distribution of vaccines to avoid arguments of ethical and humanitarian nature. Communication of the risks to the public As soon as the pandemic is declared, the communication of the real risk should be communicated to the public. Therefore, it is useful to have a communication strategy which is practical and effective. All and any type of typical difficulties of this nature of situation should also be communicated to the public. Therefore, it is important to have a communication strategy which is practical and effective. 6.5 TO CONDUCT OPERATIONAL RESEARCHS ON THE PANDEMICS With an outbreak of an avian influenza pandemic, new drugs and vaccines whose efficiency and safety in Mozambican population are not known should be administrated in mass. In addition to this, it is not possible to determine what will be the virulence potential, the characteristics of transmission of the virus and much less what are the most affected population groups by the pandemics virus. In this term, in the eventuality of an avian influenza pandemics become a reality, these important issues should be addressed in real time to enable that the opportune adjustments of the strategies and activities are made to redefine the activities and priorities. APPROVED BY THE COUNCIL OF MINISTERS ON 02 MAY 2006 (11TH SESSION) 24 FINAL VERSION In this base, the main objectives of the operational research in time for pandemics are as follow: To guarantee that the vaccines and anti-viral administrated are effective and safe. To identify early the lost of anti-viral effectiveness of the drugs ou of anti-virus pandemics vaccines. To identify early the adverse effects non-tolerable of drugs or of anti-virus pandemics vaccines. To identify in time the relevant virus mutations and recombination. To identify the most risk population groups and to evaluate the aspects related with viral biology. To share with other countries in the region the results and experiences relatively the relevant research and to secure the rapid information sharing on the transmission characteristics, the virulence and the most affected groups. For the materialisation of these objectives, an integrated approach with the intervention of the sector of public health laboratory and of epidemiological surveillance is required. The identification of sentry posts of epidemiological surveillance and the systematic collection of samples and the relevant information constitute very crucial activities. This component will be coordinated by INS, with strong support of the DEE. Thus, the list of proposed operational researches comprises among the other activities the following: Virus surveillance to evaluate susceptibility of the virus to the anti-viral. Clinical Surveillance of the adverse effects related to the administration of the anti-viral in humans. Evaluation of the vaccine effectiveness of the anti-virus pandemics vaccine administrated. Identification of the most affected population groups by the disease caused by the pandemics virus. Evaluation of the standard of virulence attributed to the pandemics. Identifications of virus mutations and recombination of H5N1 virus and evaluation of its relevance in the therapy, in the anti-viral diagnosis. As an example, the study on close contacts of patients, closed communities where some cases occurred, especially in risk population groups, for example, health workers provide us a panorama of behaviour change of the virus. Information on clinical evolution of the cases provide important information, level of severity of the disease associated to the diminution of the lethal effects indicate some or nome improvements of the transmissibility. For the materialisation of many of these activities, it will be necessary to establish partnerships with WHO reference laboratories for the execution of more specialised testages which are not possible to be undertaken in Mozambique. For example, the analysis to the virus collected during surveillance activities, enable to the WHO laboratory to discover the changes occurred in the virus and to determine if these indicate improvement in the transmissibility assisted by epidmiologic clinical observations. Support to epidemiological research GOARN is presently developing a specific manual for epidemiological research of H5N1 pandemics based on the results in different countries. The viable evaluation of risk depend on research of sporadic human cases which occurred in certain settlements. - Translation and adaptation of the manual - Reproduction and distribution - Training of health personnel Co-ordination of clinical research with other countries APPROVED BY THE COUNCIL OF MINISTERS ON 02 MAY 2006 (11TH SESSION) 25 FINAL VERSION Data obtained in the clinic need to be compiled and compared in order to elucidate the transmission ways of the disease, identification of risk population groups and seek for better ways for treatment. The country possesses a Telemedicine Centre in Maputo (Radiology service, never used) with contract with Nampula and Beira (Central Hospitals). - To know the operational state of the equipment - To know if there is trained staff capable to use - To explore the capacity of contact with overseas - To seek other ways of contacts (e-mails) The use of this type of technology enables the rapid exchange of information and experience incentivating the standardisation of protocols for treatment and of research procedures. The impact of the measures of prevention and of treatment of patients and in the last stage of the current plan depends of the effectiveness and speed in the implementation of these researches. In addition to these, visits for the exchange of experiences with countries already affected by avian influenza will be of great usefulness to the country as it will enable it to become better prepared to face the epidemics. 7. CONCLUSION This plan seeks to provide a more realistically possible picture of the activities that are necessary to undertake an effective struggle against an eminent catastrophe, in case that it happens in Mozambique. It is clear that joint efforts should be carried out not only by the Mozambique Government and group of experts in various social fields, but moreover with direct and active involvement of civil society and the population in general will be determinant for a successful struggle against this disease. It is obvious that all efforts should be made in an exercise of full conscience in all levels meaning that the information should be available to all stakeholders in particular civil society and population in general. The information, besides facilitating the decision-taking with the consent of the population, it can, de per si, be a great gun of struggle against this disease. In the struggle against this disease, we should place priority to epidemiological surveillance at the level of birds and in humans, at the same time. A WHO old slogan says “it is better to prevent than curing” is gaining perfect echo if we look for the budget of the present budget. From a total amount of 13,289,072,288.33 billions of Meticais (531,562,891.53 USD) approximately 12,907,775,070.45 billions of Meticais (516,311,002.82 USD, cerca de 97%) will be used in the field of co-ordination, logistics and maintenance and from this amount, more than 60% (8,061,848,437.50 billions of Meticais) only to guarantee the activities in the curative field (anti-viral treatment for 25% of the population) in the case the disease being declared as reality in Mozambique. And therefore, it is mandatory since all our efforts are being invested to guarantee the implementation of the activities of prevention, reinforced by a good information, communication and education of the whole civil society and of the public in general, otherwise all efforts that are being made towards reducing absolute poverty will be reduced to zero. APPROVED BY THE COUNCIL OF MINISTERS ON 02 MAY 2006 (11TH SESSION) 26 FINAL VERSION ACKNOWLEDGEMENTS WHO, USAID, World Bank, SADC, administrative staff and assistant of the DAS, DNP and DNS. REFERENCES 1. WHO, Preparing Influenza Pandemic Preparedness Plans: A step-by-step Approach, WHO, Sep-2005 2. WHO/CDC/CRS/GIP, Checklist for Influenza Pandemic Preparedness Planning, Apr-2005 3. WHO/CDC/CRS/GIP, Responding to the Avian Influenza Pandemic Threat, Recommended Strategic Actions, Ago-2005 4. WHO, Strategic Action Plan for Pandemic Influenza 2006-2007(Draft) 5. WHO, Pandemic Influenza Draft Protocol for Rapid response and Containment, Jan-2006 6. WHO, Report on a Regional Ad hoc Expert Panel Meeting, Harare, Zimbabwe, 12-13 Oct-2005 7. WHO AFRO, Influenza Pandemic Risk Assessment and Preparedness in Africa, WHO-AFRO, Brazzaville, 2005, 8. , WHO AFRO, Regional Pandemic Influenza Preparedness and Response Plan, 2006-2007, WHO AFRO, Dez-2005 9. Tanuri A., Relatório sobre o desenvolvimento da capacidade de diagnóstico laboratorial do vírus H5N1 em Humanos em Moçambique, CDC/GAP ATLANTA 10. 11. 12. 13. www.who.int www.medscape.com www.destinationrx.com www.rxalpharmacy.com APPROVED BY THE COUNCIL OF MINISTERS ON 02 MAY 2006 (11TH SESSION) 27 FINAL VERSION ANNEXES 1. Orçamento para o combate a Gripe das aves e possível pandemia. CAREÇE DE TRADUÇÃO 2. Panfleto com informações sobre a gripe aviaria CAREÇE DE TRADUÇÃO APPROVED BY THE COUNCIL OF MINISTERS ON 02 MAY 2006 (11TH SESSION) 28