Background
advertisement

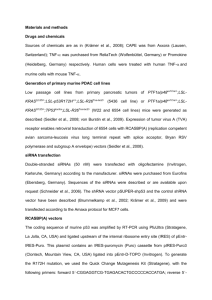
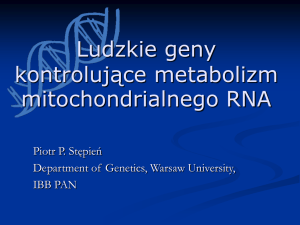
106749598 1 PREDICTIVE ROLE OF EXTRACELLULAR SURVIVIN FOR THE DEVELOPMENT OF JOINT DESTRUCTIONS IN RHEUMATOID ARTHRITIS Maria BOKAREWA, Department of Rheumatology and Inflammation Research, Göteborg University In collaboration with Lennart Bertilsson, Rheumatology Clinics, Sahlgrenska University Hospital Göran Kvist, Rheumatology Unit, Southern Alfsborg Hospital, Borås Christopher Schaufelberger, Rheumatology Unit, Mölndal Hospital, Andrey Shestakov, Department of Rheumatology, Göteborg University Tomas Torstenson, Rheumatology Unit, Uddevalla Hospital Specific aims 1) To prospectively analyse the role of survivin for the development of destructive joint disease in patients with RA 2) To assess the role of survivin in differentiation and phenotypical changes of synovial and bone cells facilitating joint destruction 3) To evaluate an efficient and safe mean of disrupting survivin signalling preventing development of RA Background Chronic inflammation followed by progressive destruction of the joints is a hallmark of RA. It is generally accepted that the inflammatory process in RA synovial tissue is coordinated by cytokines. Uncontrolled, tumour-like growth of synovial tissue followed by invasion and destruction of cartilage is a classical feature of RA. Synovial fibroblasts of RA patients demonstrate features of transformed cells with multiple oncogene mutations and impaired apoptosis, having the ability to proliferate, to invade the surrounding tissues in a tumor-like fashion. Apoptosis is a programmed cell death that may be initiated by disruption of mitochondrial integrity inside the cell or by stimulation with TNF or Fasligand of the cell surface Fas/APO-1. We were first to show that activity of apoptosis inhibitor survivin is dramatically increased in RA patients. Moreover, high levels of extracellular survivin are associated with 16-fold increased frequency of a destructive joint disease (2). In contrast, circulating antibodies against survivin in RA patients are associated with less aggressive, non-erosive course of arthritis. These findings indicate survivin to be an important participant in pathogenesis of RA. Little is known about regulation of survivin expression. Signalling through Wnt glycoproteins followed by nuclear translocation of catenin has been suggested as one of mechanisms upregulating expression of survivin. Members of Wnt family are overexpressed in RA synovium. Transfection of normal synovial fibroblasts with Wnt expressing construct results in RA-like cytokine production pattern and activated invasive cell phenotype. Nuclear hormone receptor, peroxisome proliferator-activated receptor (PPAR)- is shown to antagonise Wnt signalling. We have shown that PPAR- agonists downregulate expression of both resistin and survivin. In turn, incubation of human leukocytes with resistin results in suppression of PPAR- transcription. Agonists of PPAR- (glitazones) are used as anti-diabetic drugs, but other applications as anti-tumour and anti-atherosclerotic agents are being presently tested in clinical trials. In the mouse model of collagen II-induced arthritis, PPAR- agonists are shown to alleviate arthritis. We suggest resistin-survivin axis to be a novel inflammatory pathway in the pathogenesis of RA. Working hypothesis We suggest resistin-survivin axis as a novel pathway in the pathogenesis of RA. Uncontrolled expression of resistin in the inflamed synovial tissues during RA down-regulates PPAR-gamma and facilitates activation of Wnt signalling system followed by intracellular accumulation of survivin. Extracellular survivin regulates cell migration and differentiation facilitating their invasive and 106749598 2 osteoclastic phenotype. This would support destruction of cartilage and subchondral bone. Resistin orchestrates cytokine-driven synovial inflammation while survivin contributes to destructive arthritis. Materials and Methods 1. Extracellular functions of survivin Which cells respond to stimulation with extracellular survivin? How does stimulation with survivin change function of leukocytes? Recombinant human survivin is expressed in E.coli using a pHIS8 expression vector provided by Mark A. Verdecia, The Salk Institute, LaJolla, CA (5). The survivin sequence in the plasmid was verified by DNA sequencing using T7 and SP6 primers. Following expression, bacterial pellet was submitted to lyzosyme cleavage and sonication. Survivin was purified through His-tag on a Ni2+-NTA column. His-tag was removed by thrombin cleavage. Survivin was depleted from endotoxin (using Detoxy gel) and dialysed. The presence of survivin in the eluate was tested by Western blot and its concentration was detected by anti-survivin ELISA. Mouse monoclonal antibodies to human survivin are raised in collaboration with Prof.Pietro Speziale, University of Pavia, Italy. Peripheral blood granulocytes and mononuclear cells (lymphocytes and monocytes) from healthy controls and patients with RA will be stimulated with recombinant survivin. The effects of extracellular survivin will be assessed with respect to phenotypical and functional changes – expression of adhesion molecules (integrins, selectins, immunoglobulin superfamily), co-stimulatory molecules (CD25, CD28, CD40, CD80), and cytokine production (IL1, IL2, IL4, IL6, IL10, IFN-). To evaluate the capacity of survivin to induce apoptosis, leukocytes from healthy subjects and RA patients treated with recombinant survivin will be assessed for the expression of annexin V (FACS), TUNEL assay, activation state of mitochondrial membrane (ApoAlert), and cytochrome c release (ELISA). Cell cycle response to survivin treatment will be assessed using FACS and employing bromodeoxyuridine incorporation for the assessment of S-phase cells and propidium iodide incorporation for the assessment of total DNA content. To assess the role of survivin in lymphocyte response, PBMC will be stimulated with tetanus toxoid (antigen specific response), phytohaemagglutinin (mitogen-induced response), TSST-1 (superantigen induced response), or submitted to mixed leukocyte response (allogenic response). Binding of survivin to different types of leukocytes will be visualised by FACS. Samples of rheumatoid synovia will be cultured in survivin-rich medium. Additionally, explants of synovial tissues will be treated with antibodies against survivin. Synovial tissues will be assessed for a) the invasive growth and proliferation capacity, b) expression of adhesion molecules and apoptosis markers, c) expression of proteases and their specific inhibitors (uPA/PAI, cathepsin K/cystatin c, metalloproteinases/TIMPs). 2. Role of extracellular survivin in cell differentiation What is the role of survivin in maturation and differentiation of mononuclear cells? What is the role of extracellular survivin in osteogenesis and bone remodelling? Which intracellular mechanisms are activated by survivin? In a cross-sectional study of RA patients we observed high correlation between the presence of extracellular circulating survivin and joint destructions (2). However, survivin had no direct correlation to the markers of inflammation, as serum amyloid A protein or IL-6 in vivo (6) and induced no cytokine expression in vitro. In contrast, stimulation of human leukocytes with survivin resulted in significant activation of p38 MAP-kinase (5), a potent regulator of osteogenesis. We aim to assess the role of survivin in differentiation of osteoclasts/osteoblasts. Mononuclear cell lines THP-1 and HL60 will be used to assess further differentiation of monocytes mediated by survivin. THP-1 will be driven to a macrophage and fibroblast differentiation using PMA and all-trans retinoic acid (7). HL60 will be differentiated to osteoclasts using DMSO and 1, 25(OH)2dihydroxyvitamin D3 (8). Cells will be cultured in M-CSF/RANKL rich medium in the presence and absence of survivin. The development of osteoclasts will be followed by the formation of multinuclear 106749598 3 TRAP-positive cells. The osteoblastic differentiation will be followed by mineralization (cresolphthalein) and alkaline phosphatase (ALP) activity. Expression of RANK and osteoprotegrin will be assessed immunohistologically. Additionally, cells will be cultured in the presence of constant levels of anti-survivin antibodies. Alternatively, intracellular survivin will be blocked using siRNA. The role of p38 MAPK in osteoclast differentiation will be tested using synthetic inhibitor of p38 (SB203580). For monitoring the effect of p38 deficiency, the resorbtion capacity of differentiated osteoclasts will be employed. PPAR-gamma is known as a potent regulator of both PI3-kinase and Wnt signalling pathways. Role of PPAR-gamma in survivin-induced cell differentiation will be assessed using PPAR-gamma agonist (rosiglitazone) and PPAR-gamma antagonist (T0070907) supplementation in PBMC cultures. To study the role of Wnt signalling, human wnt5a cDNA will be subcloned into the expression vector pcDNA3 (Invitrogen), and synovial fibroblasts will be transfected with wnt5a expressing DNA plasmid. Expression of wnt protein (wnt2 and wnt3a) will be assessed by Western blot. Intracellular expression of p38, PI3-kinase and PPAR-gamma will be assessed at different phases of cell differentiation by Fast Activated Cell-based ELISA (FACE, Active Motif). 3. Predictive role of survivin for the development of destructive rheumatoid arthritis What is the frequency of patients with early RA displaying high circulating survivin levels? May survivin level be used to identify patients with unfavourable course of RA and to predict the development of joint destruction? To assess the frequency and prognostic significance of circulating survivin in early RA, patients with RA duration below 3 years attending Rheumatology Units at the hospitals of the Western region of Sweden (Västra Götaland) will be studied. At inclusion, RA patients will be clinically assessed, perform radiological examination of hand and foot skeleton, and leave blood samples. Clinical characteristics of disease activity (Disease Activity Score, DAS28) and functional disability (Health Assessment Questionarie, HAQ) will be registered. Blood samples will be used for the measurement of survivin level (ELISA) and determination of established predictive factors of RA including rheumatoid factors and antibodies against citrullinated peptides will be performed. Three years later the same cohort of patients will be evaluated clinically, radiologically and for the presence of circulating survivin. To assess the predictive value of survivin on the course of RA, the patients will be stratified according to the presence of circulating survivin and other predictive markers in the first sample. The outcome will be evaluated with respect to joint destruction (radiologically evaluated as erosivity, Larsen score (4)), and the requirement of treatment intensity. Biochemical markers of cartilage and bone metabolism in the patients with high and low levels of extracellular survivin will be compared including the levels of bone sialoprotein, C-terminal telopeptide of type I collagen (ICTP), type II collagen C-telopeptide (CTX-II), cartilage oligometric matrix protein (COMP). We expect to include 400 patients during a three-year period with a drop out from the study between 25-30% before the second examination. At present about 150 RA patients with the disease duration less than 3 years are enrolled in the study and they left their first blood sample. In the preliminary assessment of these 150 samples, circulating survivin is found in more than 40% of these patiens. Significance The recognition of survivin as an important prognostic factor for the development of joint destructions helps identification of patients with poor prognosis of RA and monitoring of therapeutic efficacy. Clinical relevance Rheumatoid arthritis (RA) is a common disease with the prevalence of 0.5-1% in the entire population. Pathogenetic mechanisms and prognostic features of RA are not completely understood. My research group suggests a novel set of molecular events initiating inflammation in the joints and leading to joint destruction. We demonstrated that anti-apoptotic molecule, survivin, may be used as a potential predictive marker of destructive course of arthritis. Our hypothesis is based on the results obtained in 4 106749598 patient material and is supported by studies on cell level and in animal models. We plan to expand our observations preparing a prospective clinical study including a cohort of patients from Västra Götaland region. We will also continue our studies on the molecular events initiated by survivin on the cell surface and inside the cells. We believe that better understanding of survivin-mediated processes is an important part of joint inflammation. Targeting these processes may become a new efficient treatment modality of patients with RA. Ethical considerations Synovial fluid and blood samples will be obtained after the patient is informed and gives an agreement to participate in the study. Patient identity will be protected by an immediate coding of all the samples. Analyses of the samples are performed using coded tubes. Study is approved by the Ethic Commettee of Sahlgrenska University Hospital (S-441-01, 385-04). Animal studies will be performed with an agreement and according to the guidelines of Helsinki Convention. Animal models of collageninduced arthritis (332-2003), staphylococcal arthritis (326-2003), and resistin-induced arthritis (2712003) are all approved by the Committee for Animal Experiments, Göteborg University. Preliminary results 1. Extracellular expression of survivin during rheumatoid arthritis We have shown that high extracellular levels of survivin may be detected in about 30% of RA patients. Moreover, survivin expression has been found to be an independent prognostic marker of erosive disease increasing risk of joint destructions in RA 16-folds. In contrast, antibodies against survivin were associated with less aggressive non-erosive course of joint disease (2). P<0.0019 P<0.05 600 P<0.035 Plasma Synovial fluid 450 300 150 0 RA, erosive n=88 RA, non-erosive n=43 Healthy controls n=34 Increased frequency of circulating survivin was also observed in patients with juvenile chronic arthritis (about 20%). Circulating survivin was associated with systemic and oligoarticular type of JCA and the presence of RF. Indicating a possible predictive value of circulating survivin for identification of patients with unfavourable course of JCA (6). 2. Recombinant survivin and monoclonal antibodies For the evaluation of extracellular properties of survivin we a) successfully expressed recombinant human survivin, b) obtained significant amount of monoclonal antibodies to survivin for our further studies. 3. Properties of extracellular survivin We have identified two leukocyte populations sensitive to survivin. Survivin binds to lymphocytes and neutrophils. Stimulation with extracellular survivin leads to the expression of 2-integrins on the surface of human neutrophils. Survivin-dependent upregulation of 2-integrins was independent on NF-kappaB pathway and was mediated by p38 MAP-kinase and PI3-kinase/Akt signalling. The clinical relevance of this observation is supported by studies of RA patients showing that the neutrophils of patients with high extracellular survivin levels express higher proportion of 2-integrins (5). In human lymphocyte survivin prevented CD3-dependent proliferation and production of IL2 and INF-gamma cytokines. 5 106749598 200 Pr oli fer ati on , % P<0.05 P<0.05 n.s. 150 survivin, 0 microg/ml survivin, 0.05 microg/ml survivin, 5 microg/ml survivin, 25 microg/ml 100 50 0 TSST-1 n=6 anti-CD3 ConA n=4 n=6 4. Intracellular signalling initiated by survivin Our recent in vitro experiments revealed that intracellular effects of survivin are mediated by PI3kinase and p38 MAP-kinase, potent regulators of osteogenesis. The effects are abrogated by specific inhibitors of transcription factors (SB203580 for p38, and LY294002 for PI3-kinase). These two findings support our version of survivin being an important participant of bone remodelling during arthritis. References 1. Bokarewa MI, Nagaev I, Dahlberg L, Smith U, Tarkowski A. Resistin, an adipokine with potent proinflammatory properties. J Immunology 2005, 173:5789-95. 2. Bokarewa MI, Lindblad S, Bokarew D, Tarkowski A. Balance between survivin, a key member of apoptosis inhibitor family, and its specific antibodies determines erosivity in rheumatoid arthritis. Arth Res&Ther 2005, 7:R349-R358. 3. Pullerits R, Jonsson IM, Verdrengh M, Bokarewa MI, Andersson U, Erlandssson-Harris H, et al. High mobility group box chromosomal protein (HMGB-1) is a proinflammatory molecule inducing arthritis. Arthritis Reum 2003, 48:1693-700. 4. Larsen A. How to apply Larsen score in evaluating radiographs of rheumatoid arthritis in long-term studies? J Rheumatol 1995, 22:1974–5. 5. Mera, S., Levshin, N., Magnusson, M., Tarkowski, A., and Bokarewa, M.I. Extracellular survivin activates adhesion molecules on the surface of human granulocytes supporting leukocyte interactions. 2006, submitted. 6. Galeotti, L., Adrian, K., Berg, S., Tarkowski, A., and Bokarewa, M.I. Circulating survivin is a marker of severe juvenile chronic arthritis. 2006, submitted. 7. Jakob F, Siggelkow H, Homann D, Kohrle J, Adamski J, Schutze N. Local estradiol metabolism in osteoblast- and osteoclast-like cells. J Steroid Biochem Mol Biol 1997, 61:167-74. 8. Zhou Z, Immel D, Xi CX, Bierhaus A, Feng X, Mei L, Nawroth P, Stern DM, Xiong WC. Regulation of osteoclast function and bone mass by RAGE. J Exp Med 2006, 203:1067-80. 9. Shestakov A, Fu H, Dahlgren C, Tarkowski A, and Bokarewa MI. Regulatory mechanisms of resistin release from specific granules of neutrophils. Manuscript.