Mental Capacity Act & Deprivation of Liberty Safeguards

NORTH EAST LINCOLNSHIRE CLINICAL COMMISSIONING GROUP
MENTAL CAPACITY ACT 2005
DEPRIVATION OF LIBERTY SAFEGUARDS POLICY
Document Reference No:
Lead Director:
Author:
Version 2.3
Julie Taylor-Clarke
Interim Director of Nursing, Quality &
Transformation, NELCCG
Chloe Nicholson
Mental Capacity Act Manager
First Version Issued On:
Latest Version Issued On (date ratified version placed on intranet):
Review Date:
Consultation Process:
1 July 2009
November 2014
November 2015
Safeguarding Adults Operational Group
Completion of Appendices (Checklist and Equality Impact Statement):
Approved By:
Chloe Nicholson, MCA Manager
Safeguarding Adults Operational Group
As above Ratified By:
Target Audience:
Dissemination:
All Health and Social Care staff
NELCCG Intranet
NAViGO Intranet
Care Plus Intranet
Social Work Pilot Intranet
All suitable partnership groups
Any locally held old paper copies must be destroyed. When this document is viewed as a paper copy, the reader is responsible for checking that it is the most current version.
2.3
2
2.1
2.2
Version
CHANGE RECORD
Author
Chloe Warburton,
MCA Manager
Liz Whyman
Nature of Change Date placed on
Intranet
Appendix 4
– 7 added
Chloe Nicholson,
MCA Manager
Chloe Nicholson,
MCA Manager
Minor amendments to format
Minor amendments to format and content
Minor amendments to format and content
October 2013
November 2014
CONTENTS
Section
1.
2.
3.
4.
5.
6.
2.1
2.2
2.3
2.4
2.5
2.6
2.7
2.8
Introduction
Executive Summary
Stage One
Stage Two
Stage Three
Stage Four
Stage Five
Stage Six
Stage Seven
Stage Eight
What is Deprivation of Liberty
6
7
Key Points Regarding the Deprivation of Liberty Safeguards
(DoLS)
9
Who is Covered by the Deprivation of Liberty Safeguards? 10
Mental Capacity
The Diagnostic Test for Capacity
11
11
4
5
5
5
2
3
4
Page
1
2
7.
6.1
6.2
6.3
6.4
6.5
6.6
7.1
7.2
The Functional Test for Capacity
Documenting Capacity Assessments
Best Interests
11
12
12
The Least Restrictive Option
The Mental Health Act 1983 (MHA) or The Mental Capacity
Act 2005 (MCA)?
The Deprivation of Liberty Safeguards Procedure
13
14
14
15 The Role of the Managing Authority
The Role of the Mental Capacity Act Manager –
The Application Process
19
8.
9.
Section
7.3
7.4
7.5
7.6
7.7
10.
11.
9.1
The MCA Manager
The Six Assessments
The Best Interests Assessor
The Authorised Signatory for the Supervisory Body
The Independent Mental Capacity Advocate (IMCA) 26
What if an application for a Deprivation of Liberty is Refused? 27
The Role of the Relevant Person’s Representative
28
Who can be a Relevant Person’s Representative?
Instructing an IMCA to Act During a Standard Authorisation for a Deprivation of Liberty when there is no Relevant
Person’s Representative Available
Instructing an IMCA to Act During a Standard Authorisation for a Deprivation of Liberty to Support the Relevant Person or their Representative
29
30
31
Page
19
20
22
24
12.
13.
14.
Requests from a Third Party for an Application for an
Authorisation for a Deprivation of Liberty
31
Reviews 33
Record Keeping 35
15.
16.
Additional Deprivation of Liberty Safeguarding Forms
Contact Details
35
37
Appendices
Appendix A Overview of the Deprivation of Liberty Safeguards Process 38
Appendix B Supervisory Body Action on Receipt of a Request for a
Standard Deprivation of Liberty Authorisation or to Determine
39 whether there is an Unauthorised Deprivation of Liberty
Appendix C Checklists
Appendix D DoLS – Essential Preparations
Appendix E Checklist for the Review and Approval of Procedural
Documents
41
60
61
NORTH EAST LINCOLNSHIRE CLINICAL COMMISSIONING GROUP
MENTAL CAPACITY ACT 2005
DEPRIVATION OF LIBERTY SAFEGUARDS POLICY
1. INTRODUCTION
This joint guidance document is for staff working within or providers of care to the
North East Lincolnshire Clinical Commissioning Group (hereafter NELCCG) where the person lacks the capacity to consent to care or treatment in circumstances that might be considered a “deprivation of liberty”.
This guidance document is also for staff working within these professional roles outside NELCCG, where the customer or patient (who lacks the capacity to consent to care or treatment in circumstances that might be considered a
“deprivation of liberty”) is likely to be moving to or returning to North East
Lincolnshire.
This guidance should be read in conjunction with the Mental Capacity Act 2005
Code of Practice and the Deprivation of Liberty Code of Practice 2007.
This document provides guidance about the Deprivation of Liberty Safeguards, whilst also providing details regarding how these safeguards link into the Mental
Capacity Act 2005. It provides information about the specific roles in these processes, their responsibilities and how they should be applied when a resident or a patient is situated in, or is due to be situated within a care home or hospital in
North East Lincolnshire in a way that is or may be deemed to be a deprivation of liberty.
The term “deprivation of liberty” is used to describe individuals who lack mental capacity and whose care or treatment involves restrictions being placed upon that person. This may occur where the person fails to meet the provisions of the
Mental Health Act 1983 but still needs additional support, for example because they don’t meet the criteria for detention under the Act or are compliant with a care plan that deprives them of their liberty. In addition, the acronym “DoLS” is used within this guidance document where applicable to represent the “Deprivation of
Liberty Safeguards.”
To ensure consistency the term “relevant person” is used throughout this guidance document wherever possible, as a term of reference for either the customer or patient. In addition the term “managing authority” is used wherever possible to refer to a care home or hospital and “supervisory body” is used wherever possible to refer to North East Lincolnshire Clinical Commissioning Group, on behalf of
North East Lincolnshire Council.
Following implementation of the Health and Social Care Act (2012), responsibility to authorise a detention under the MCADoLS has been transferred to Local
Authorities. North East Lincolnshire Council is now responsible for authorising a detention, in a care home or hospital ward, under the MCADoLS. NELCCG will continue to be responsible for the management of the MCADOLS administration process and overall implementation of the MCA.
2. EXECUTIVE SUMMARY
This Executive Summary provides an overview of the process that needs to be undertaken to meet our statutory requirements under the Mental Capacity Act
2005.
2.1 Stage One
Whenever a hospital or care home identifies that a person who lacks capacity is being, or risks being, deprived of their liberty, they must apply to the supervisory body to seek authorisation for the deprivation of liberty.
North East Lincolnshire Council is the supervisory body for people with a care package that has been commissioned by health and/or social care in a care home or hospital.
NOTE: The Mental Capacity Act 2005 will not permit someone to be deprived of their liberty without a formal authorisation
– unless it is a consequence of following a decision of the Court of Protection on a personal welfare decision.
The Deprivation of Liberty Safeguards do not introduce a new system for determining whether a person who lacks capacity to decide the matter for themselves should receive care or treatment. Nor do they provide any new power to take and convey people to hospitals or care homes. They are solely about ensuring that there are appropriate safeguards in place when it is deemed that a person who lacks the capacity to decide the matter for themselves needs to receive care or treatment, in their best interests in a hospital or care home, in circumstances that deprive them of their liberty.
There are two types of authorisation:
1. standard, and
2. urgent
A managing authority must request a standard authorisation when it appears likely that, at some time during the next 28 days, someone will be accommodated in its hospital or care home in circumstances that amount to a deprivation of liberty. The request must be made to the supervisory body.
Wherever possible, authorisation should be obtained in advance. Where this is not possible, and the managing authority believes it is necessary to deprive someone of their liberty in their best interests before the standard authorisation process can be completed, they can issue themselves an urgent authorisation and then obtain a standard authorisation within seven calendar days. An urgent authorisation can be for a maximum of 7 days but may be extended by the supervisory body for up to a further 7 days in exceptional circumstances.
NOTE: Anyone with a concern, e.g. a family member, can apply to the supervisory body to trigger an assessment of whether a person is deprived of liberty, if they have asked the care home or hospital to apply for authorisation but it has not been done. This would lead on to the full assessment process if the finding is that the person is deprived of their liberty.
2
2.2 Stage Two
When a supervisory body receives a request for authorisation of deprivation of liberty they must obtain 6 assessments. These assessments must usually be completed within 21 days of the supervisory body receiving the request for the authorisation but, if an urgent authorisation has been given by the care home or hospital, the assessments must be completed before the expiry of the urgent authorisation.
The assessments are:
1. Age Assessment
– to clarify that the person is 18 or over.
2. No Refusals Assessment – to clarify that the authorisation does not conflict with a valid decision by a done of a Lasting Power of Attorney
(an Attorney) or by a deputy appointed for the person by the Court of
Protection (a Deputy) and is not for the purpose of giving treatment that would conflict with a valid and applicable advance decision to refuse treatment made by the person, when they had the capacity to make the advance decision. The person undertaking the No Refusals
Assessment can access details regarding Attorneys and Deputies through the Office of the Public Guardian (OPG).
3. Mental Capacity Assessment – to clarify whether the person lacks the mental capacity to decide whether to be admitted to, or remain in, the hospital or care home.
4. Mental Health Assessment – to clarify whether the person is suffering from a mental disorder within the meaning of the Mental Health Act
1983.
5. Eligibility Assessment
– to clarify if the person is eligible. A person is eligible unless they are:
(i) Detained under the Mental Health Act 1983;
(ii) Subject to a requirement under the Mental Health Act 1983 that conflicts with the authorisation sought e.g. subject to guardianship requiring them to live somewhere else;
(iii) Subject to powers of recall under the Mental Health Act 1983;
OR unless the application is to enable mental health treatment in hospital and they object to being in hospital or to the treatment in question. In deciding whether a person objects, their past and present behaviour, wishes, feelings, views, beliefs, and values should be considered where relevant.
3
6. Best Interests Assessment – to clarify whether the proposed course of action would constitute a deprivation of liberty and it is:
(i) In the best interests of the person to be subject to the authorisation and
(ii) Necessary in order to prevent harm to them and
(iii) A proportionate response to the likelihood of suffering harm and the seriousness of that harm.
In line with the provisions of the Mental Capacity Act 2005, anyone who does not have family or friends who can be consulted will require an
Independent Mental Capacity Advocate (IMCA) instructed to support and represent them during the assessment process.
2.3 Stage Three
If any of the assessments conclude that the person does not meet the criteria for an authorisation to be issued, the supervisory body must refuse the request for authorisation. If this happens, the supervisory body must inform the managing authority, the relevant person, any IMCA instructed and all persons consulted by the best interest’s assessor of the decision and the reasons for it.
Where it is decided that it is not in the relevant person’s best interests to be deprived of liberty in a particular home or hospital, steps will need to be taken by the care home or the hospital to find an alternative way of providing the care that they require, which is lawful.
If the authorisation is for detention to enable life sustaining treatment or treatment believed necessary to prevent a serious deterioration in the pe rson’s condition, and there is a question about whether it may be lawfully granted, it will not be lawful to detain the person while a decision is sought from the Court of Protection.
2.4 Stage Four
The duration of any authorisation will be assessed on a case-by-case basis, taking account of the individual’s circumstances. If the best interest’s assessor concludes that a deprivation of liberty is necessary in a person’s best interests to protect them from harm, they will be required to recommend the time period of the authorisation, taking account of the possibility of circumstances changing. The maximum period for an authorisation would be 12 months but it is expected that authorisations would be for shorter periods in many cases.
4
2.5 Stage Five
If the best interest’s assessor concludes that deprivation of liberty is necessary in a person’s best interests to protect them from harm, they will be required to recommend who will be the best person to be appointed as the Relevant Person’s Representative in order to represent the person’s interests. The relevant person may choose their own representative if they have the capacity to do so. Alternatively, if there is an attorney or deputy appointed with the appropriate authority, they may select a person to be the representative. Should the relevant person be unable to choose their own representative or an attorney / donee or deputy with the appropriate authority is unavailable, then the best interest’s assessor will consider whether there is someone among those they have consulted who would be suitable.
2.6 Stage Six
If all the assessments conclude that the relevant person meets the criteria for an authorisation to be issued, the supervisory body must grant the request for a standard authorisation of deprivation of liberty. The time period of a standard authorisation may not be longer than recommended by the best interest’s assessor although it could be reduced by the supervisory body and it may not be issued for a period exceeding 12 months.
Authorisation must be in writing and include the purpose of the deprivation of liberty, the time period, any conditions attached and the reasons that each of the qualifying conditions are met. The supervisory body must give a copy of the authorisation to the managing authority, the relevant person, any IMCA instructed and all interested persons consulted by the best interest’s assessor.
The role of the Relevant Person’s Representative is to keep in touch with the person, to support them in all matters concerning the authorisation and to request a review or to make an application to the Court of Protection if necessary. If there is no one available among friends or family, then the supervisory body will appoint a person, who may be paid, to act as the representative for the duration of the authorisation.
2.7 Stage Seven
Managing authorities have a duty to:
Take all practical steps to ensure that the relevant person and their representative understand what the authorisation means for them and how they can apply to the Court of Protection or request a review
Ensure that any conditions attached to the authorisation are met; and
Monitor the individual’s circumstances as any change may require them to request that the authorisation is reviewed.
The managing authority can apply for a further authorisation when the authorisation expires. It is good practice for managing authorities to reassess the relevant person 28 days prior to the authorisation expiring and reapply for a standard authorisation if appropriate.
5
2.8 Stage Eight
A review may be carried out while an authorisation is in place for the following reasons:
The managing authority requests a review because the person’s circumstances have changed.
The relevant person or their representative requests a review.
The supervisory body must conduct a review if asked to do so as above.
Assessments would be carried out for any of the criteria for authorisation affected by any change of circumstances. The outcome of the review may be to terminate the authorisation, vary the conditions attached or change the reason recorded that the person meets the criteria for authorisation. The managing authority, the relevant person and their representative must be informed of the outcome of a review.
The relevant person, or the person appointed as their representative, or an attorney or deputy, can at any time request that an authorisation be reviewed by the supervisory body and also has the right to make an application to the Court of Protection to challenge the decision to authorise deprivation of liberty at any time.
Where an IMCA is instructed, they can provide support with a review or with an application to the Court of Protection. Any other person may apply to the
Court of Protection for permission to challenge a decision to deprive someone of their liberty. Legal Aid is available for challenges by the person deprived of liberty or their representative to the Court of Protection.
6
3. WHAT IS A DEPRIVATION OF LIBERTY?
On 19 th March 2014, the Supreme Court handed down its judgement in the
Cheshire West case [Cheshire West [2014] UKSC 19]. Through this judgement, the Supreme Court sought to define a deprivation of liberty under the MCADoLS.
The Supreme Court has now confirmed that there are two key questions to ask, these questions are termed the ‘acid test’:
1. Is the person subject to continuous supervision and control? (all three aspects are necessary) AND
2. Is the person free to leave? (The person may not be saying this or acting on it but the issue is about how staff would react if the person did try to leave).
So this now means that if a person is subject both to continuous supervision and control and not free to leave they are deprived of their liberty.
The following factors are no longer relevant to this:
(1) the person’s compliance or lack of objection;
(2) the relative normality of the placement and
(3) the reason or purpose behind a particular placement.
For the full judgement, please see:
P (by his litigation friend the Official Solicitor) (Appellant) v Cheshire West and
Chester Council and another (Respondents); P and Q (by their litigation friend, the
Official Solicitor) (Appellants) v Surrey County Council (Respondent) [2014] UKSC
19 On appeal from [2011] EWCA Civ 1257; [2011] EWCA Civ 190
When considering if a person is being detained, bear in mind the following key points:
Assess the degree of “control” by reference to factors such as nature, frequency, intensity, duration of intervention
Disregard the purpose, compliance / happiness, “normality”, (absence of alternatives, appropriateness / quality of care)
Err on the side of caution
Consider whether the restrictions can be reduced via amendment to the care plan.
In addition to the above, staff are advised to read the Deprivation of Liberty Code of Practice 2007. The Code includes further consideration regarding what is permissible under the Mental Capacity act 2005 in relation to restraint or restriction.
7
The European Court of Human Rights (ECHR) has made it clear that the question of whether someone has been deprived of liberty depends on the particular circumstances of the case in question. Specifically, the ECHR said in its October
2004 judgment in HL v UK:
“to determine whether there has been a deprivation of liberty, the starting point must be the specific situation of the individual concerned and account must be taken of a whole range of factors in a particular case such as type, duration, effects and manner of implementation of the measure in question. The distinction between a deprivation of, and restriction upon, liberty is merely one of degree or intensity and not one of nature or substance.”
Although the guidance within this document details findings from past decisions of the courts, which can be useful when attempting to evaluate whether a deprivation of liberty is occurring, each individual case must be assessed on its own circumstances.
It is important to remember that this list is not exclusive and other factors may determine the outcome of a case. Likewise whilst one incident in itself is unlikely to equate to a deprivation of liberty, the cumulative effect of two or more incidents may highlight the existence of a deprivation of liberty rather than that of remissible restraint.
Section 6 (4) of the Mental Capacity Act 2005 (Paragraph 6.40 of the MCA Code of
Practice) states that someone is using restraint if they:
Use force – or threaten to use force – to make someone do something that they are resisting, or
Restrict a person’s freedom of movement, whether they are resisting or not.
Paragraphs 6.40 to 6.48 of the Mental Capacity Act Code of Practice contain guidance about the appropriate use of restraint. Restraint is appropriate when it is used to prevent harm to the person who lacks capacity and it is a proportionate response to the likelihood and seriousness of harm. Appropriate use of restraint falls short of deprivation of liberty.
Preventing a person from leaving a care home or hospital unaccompanied because there is a risk, for example that they would try to cross a road in a dangerous way, is likely to be seen as proportionate restraint to prevent the person from coming to harm. That would be unlikely, in itself, to constitute a deprivation of liberty. Similarly, locking a door to guard against immediate harm is unlikely, in itself to amount to a deprivation of liberty.
The ECHR has also indicated that the duration of any restrictions is a relevant factor when considering whether or not a person is deprived of their liberty. This suggests that actions that are immediately necessary to prevent harm, may not, in themselves, constitute a deprivation of liberty.
8
However, where the restriction or restraint is frequent, cumulative and ongoing, or if there are any other factors present , care providers should consider whether this has gone beyond permissible restraint, as defined within the
Mental Capacity Act. If so, they must apply for authorisation under the DoLS deprivation of liberty safeguards or change their care provision to reduce the level of restraint to a less restrictive option.
In order to fall within the scope of a deprivation of liberty authorisation, a person must be detained in a hospital or care home, for the purpose of being given care or treatment in circumstances that amount to a deprivation of liberty. As part of the care planning process, consideration should be given to the potential of a deprivation of liberty arising in instances of respite care and the taking of the necessary steps to prevent the deprivation arising.
4. KEY POINTS REGARDING THE DEPRIVATION OF LIBERTY SAFEGUARDS
(DoLS)
People who suffer from a disorder or disability of the mind, such as dementia or a profound learning disability, and who lack the mental capacity to consent to the care or treatment they need, should be cared for in a way that does not limit their rights or freedom of action. In some cases members of this vulnerable group need to be deprived of their liberty for treatment or care because this is necessary in their best interests to protect them from harm.
The aim of the DoLS is to provide legal protection for those vulnerable people who are deprived of their liberty otherwise than under the Mental Health Act 1983, to prevent arbitrary decisions to deprive a person of liberty and to give rights to challenge deprivation of liberty authorisations.
The safeguards apply to people who lack capacity to consent to treatment, and who have a disorder of the mind. It is anticipated that through the implementation of the
DoLS the number of people deprived of their liberty in care homes and hospital will be reduced.
The five statutory principles underpinning the Mental Capacity Act 2005 will apply to the operation of these safeguards, principally the requirement to act in the best interests of the person lacking capacity to consent to the care or treatment and to locate the less restrictive option.
9
5. WHO IS COVERED BY THE DEPRIVATION OF LIBERTY SAFEGUARDS?
The deprivation of liberty safeguards cover patients in hospital, and people in care homes registered under the Care Standard Act 2000 , whether placed under public or private arrangements.
The safeguards apply to people aged 18 and over whom:
1. Suffer from a disorder or disability of mind and
2. Lack the capacity to give consent to the arrangements made for their care or
treatment and
3. For whom such care (in circumstances that amount to a deprivation of liberty within the meaning of Article 5 of the European Convention of Human Rights) is considered, after an independent assessment, to be a necessary and proportionate response in their best interests to protect them from harm.
NOTE: These safeguards cannot be used to detain people in hospital for the treatment for a mental disorder in situations where the Mental Health Act 1983 could be used if they are thought to object to being in hospital or to receiving treatment.
This will mean that people who object will be treated in broadly the same way as people with capacity who are refusing treatment for mental disorders and who need to be detained as a result.
People who need to be covered by the deprivation of liberty safeguards are anticipated to be mainly those with significant learning disabilities or people suffering from dementia but will include a minority of others who have suffered physical injury, such as acquired brain injury.
The deprivation of liberty safeguards do not apply to people other than those identified within the above categories, for example; those living within their own home, a sheltered housing scheme. Should a person in such a setting currently be, or at risk of being, deprived of their liberty then an application should be made to the Court of Protection.
10
6. MENTAL CAPACITY
For clarification of capacity issues, staff should see chapter 4 of the MCA Code of
Practice in relation to the Mental Capacity Act (MCA) 2005
In accordance with the five statutory principles in the MCA 2005, the initial assumption must always be that a person has the capacity to make a decision, unless it can be established that they lack capacity.
Capacity is assessed in rela tion to an individual’s capacity to make a particular decision at the time it needs to be made and is judged on objective criteria, rather than on the basis of assumptions regarding age, appearance, condition or behaviour.
There is a two-stage test for capacity:-
1. Does the person have an impairment of the mind of brain, or is there some sort of disturbance affecting the way their mind or brain works? (This may be temporary or permanent)?
See ‘6.1 - The Diagnostic Test for Capacity’ below for more detail
2. If so, does the impairment or disturbance mean that the person is unable to make the decision in question – in this case, whether they should receive care or treatment that involves depriving them of their liberty – at the time it needs to be made?
See
‘6.2 - The Functional Test for Capacity’ below for more details
6.1 The Diagnostic Test for Capacity
It is first necessary to ask: does the person have an impairment of, or a disturbance in the functioning of, their mind or brain?
If the answer to this question is “no” the person does not lack capacity as defined by the MCA 2005 and this guidance does not apply to their situation.
6.2 The Functional Test for Capacity
If the answer to the question above is “yes”, it is then necessary for the
Decision Maker (within the DoLS this could be the best interest’s assessor, mental health assessor, managing authority and others), to ask:-
(i) Do they have an understanding of what decision they need to make and why they need to make it?
(ii) Do they have an understanding of the likely consequences of making, or not making the decision?
(iii) Are they able to understand, retain, use and weigh up the information relevant to the decision?
(iv) Can they communicate their decision by any means, including via an interpreter or with the help of a speech and language therapist or communication aids?
11
The decision as to whether somebody has capacity is made “on the balance of probabilities”. This means that, in order to determine that a person lacks capacity to make a decision at the time it needs to be made, it is necessary to be able to demonstrate that it is more likely than not that the person lacks capacity.
6.3 Documenting Capacity Assessments
The first statutory principle of the MCA 2005 is that there is an assumption of capacity. It is therefore important for staff to record any reasons for considering that a person does not have capacity in relation to a specific decision.
Where there is evidence of impaired decision-making capacity, this evidence should be recorded.
The MCA Code of Practice states that “where assessments of capacity relate to day to day decisions and caring actions, no formal assessment procedures or recorded documentation will be required.” However, it goes on to state that the more important a decision is, the greater the need for clear recordings and that it is
“good practice that a proper assessment of capacity is made and the findings of that assessment are recorded in the relevant professional records.”
It is important to note that the diagnostic test for capacity does not always involve the assessment of a patient/resident by a doctor. An informal carer, paid carer, social worker or other decision maker may have available to them sufficient information to determine that a person suffers from a condition or a disability that affects their decision making ability.
All attempts to assist a person to make the decision themselves should be recorded.
6.4 Best Interests
The fourth statutory principle of the MCA 2005 is that any act done for, or any decision made on behalf of a person who lacks capacity must be done, or made, in that person’s “best interests.”
Chapter 5 of the MCA Code of Practice states that a person who is trying to determine the best interests of a person who lacks capacity to make a specific decision should:- a) Encourage participation b) Identify all relevant circumstances c) Find out the person’s views, where possible d) Avoid discrimination e) Assess whether the person might regain capacity f) Ensure that decisions regarding life-sustaining treatment are not motivated by a desire to bring about the person’s death. g) Consult others h) Avoid restricting the person’s rights.
12
It is the decision maker’s decision as to what is in the best interests of a person who lacks capacity. The identity of the Decision Maker will vary with the type of decision being made. For most day to day care decisions this will be the family carer or paid carer, with regard to medical treatment it will be the responsible health care professional and where an attorney or deputy has been appointed under a Lasting Power of Attorney or by the Court of
Protection, it will be the Attorney or Deputy if the decision falls within the scope of their authority.
It is possible for a decision to be made by joint decision makers, for example when putting together a care plan for a customer who lacks capacity which involves input from different Health and Social Care staff. It is essential that clear recording identifies who is or are the Decision Makers with regard to specific decisions and the reasons for reaching the decision that the best interests of the customer who lacks capacity are met.
6.5
The Least Restrictive Option
The fifth key principle of the Mental Capacity Act 2005 states that; “before an act is done or a decision is made (which has been assessed to be in the person’s best interests) regard must be had to whether the purpose for which it is needed can be as effectively achieved in a way that is less restrictive of the person’s rights and freedom of action.
”
Section 5 of the Mental Capacity Act provides legal protection for people who care for or treat someone who lacks capacity provided that the Act’s principles are followed and that action is taken in the incapacitated person’s best interests.
However the Mental Capacity Act can only be used to restrain people to the extent that the restraint is:- a) necessary to protect the person who lacks a capacity from harm and b) in proportion to the likelihood and seriousness of that harm.
Section 5 of the Act does not give protection to decision makers for actions that deprive a person of their liberty, unless a standard and/or an urgent authorisation is obtained.
13
6.6
The Mental Health Act 1983 (MHA) or The Mental Capacity Act 2005
(MCA)?
Because the Mental Capacity Act does not authorise people who lack capacity to be provided with care or treatment that deprives them of their liberty , it may be necessary to think about using the MHA to detain and treat somebody who lacks capacity to consent to treatment in circumstances where:-
(i) it is not possible to give the person the care or treatment they need without doing something that might deprive them of their liberty.
(ii) the person needs treatment that cannot be given under the Mental
Capacity Act (for example because they have made a valid advance decision to refuse an essential part of the treatment).
(iii) the person may need to be restrained in a way that is not allowed under the Mental Capacity Act.
(iv) it is not possible to assess or treat the person safely or effectively without treatment being compulsory, e.g. because the person is expected to regain capacity to consent, but might then refuse to consent.
(v) the person lacks capacity to decide on some elements of the treatment but has capacity to refuse a vital part of it, and they have done so or
(vi) there is some other reason why the person might not get treatment, and they or somebody else might suffer harm as a result.
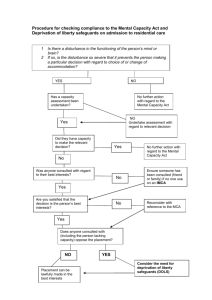
7. THE DoLS PROCEDURE FOR NORTH EAST LINCOLNSHIRE
There are some circumstances in which depriving a person, who lacks capacity to consent to the arrangements made for their care or treatment, of their liberty is necessary to protect them from harm and is in their best interests . In such instances and in order to ensure that no individual who may lack capacity to consent to the arrangements made for their care or treatment is unlawfully deprived of their liberty, the following procedure should be followed;
To obtain authorisation to deprive someone of their liberty, managing authorities
(care homes or hospitals) must apply for authorisation following the processes set out in this chapter. Once an application has been received, the supervisory body
(focus independent adult social care on behalf of North East Lincolnshire Council) must follow the assessment processes before it can authorise deprivation of liberty.
It should be borne in mind that an authorisation for deprivation of liberty does not, it itself, give authority to treat people, nor do anything else that would normally require their consent.
14
In the vast majority of cases, it should be possible to plan in advance (up to 28 days) so that a standard authorisation can be obtained before the deprivation of liberty begins. There may, however, be some exceptional cases where the need for the deprivation of liberty is so urgent that it is in the best interests of the person for it to begin while the application is being considered. In that case, the managing authority may give an urgent authorisation for up to seven days.
A managing authority has responsibility for applying for authorisation of deprivation of liberty for any person who may come within the scope of the deprivation of liberty safeguards.
If a healthcare or social care professional thinks that an authorisation is needed, they should inform the managing authority. This might be as a result of a review or needs assessment.
A supervisory body is responsible for considering requests, for commissioning the required assessments, and where all the six assessments agree, for authorising the deprivation of liberty.
7.1 The Role of the Managing Authority
A managing authority has responsibility for applying for authorisation of deprivation of liberty for any persons who may come within the scope of the deprivation of liberty safeguards:
In the case of an NHS hospital, the managing authority is the NHS body responsible for the running of the hospital in which the relevant person is, or is to be a resident.
In the case of a care home or a private hospital, the managing authority will be the person registered, or required to be registered, under Part 2 of the Care Standards Act 2000 in respect of the hospital or care home.
Relevant staff employed by managing authorities should have undertaken appropriate training in the Mental Capacity Act and the Deprivation of
Liberty Safeguards in order to prepare them for the implementation of the
DoLS in April 2009.
In addition they should have their own procedure in place that identifies:
Whether deprivation of liberty is or may be necessary in a particular case.
What steps they should take to assess whether to seek authorisation.
Whether they have taken all practical and reasonable steps to avoid a deprivation of liberty from occurring
What action they should take if they do need to request an authorisation.
How they should review cases where authorisation is or may be necessary
15
Who should take the necessary action
Having followed the process outlined within the DoLS Process Flowchart, should the managing authority feel that an application for deprivation of liberty is necessary they must do the following:
For a standard application - complete DoLS Form 4
For an urgent application – complete DoLS Forms 1 & 4
The form should be submitted via email to: focus.mcadols@nhs.net
The application must be made in writing, using the standard DoLS forms.
Wherever possible, applications for deprivation of liberty authorisations should be made before the deprivation of liberty commences. However, where a deprivation of liberty unavoidably needs to commence before a standard authorisation can be obtained, an Urgent Authorisation can be given by the managing authority, which will make the deprivation of liberty lawful for seven days provided a Standard Authorisation has been applied for.
Should this situation arise the managing authority must notify the supervisory body on the Standard Authorisation that an Urgent
Authorisation has been given. This seven day period of Urgent
Authorisation can not be extended unless exceptional circumstances exist.
A managing authority can give itself an Urgent Authorisation for deprivation where:
It is required to make a request to the supervisory body for a standard authorisation, but believes that the need for the person to be deprived of their liberty is so urgent that the deprivation needs to begin before the request is made, or
It has made a request for a Standard Authorisation, but believes that the need for a person to be deprived of liberty has now become so urgent that deprivation of liberty needs to begin before the request is dealt with by the supervisory body.
This means that an Urgent Authorisation can never be given without a request for Standard Authorisation being made simultaneously. Therefore, before giving an Urgent Authorisation, a managing authority will need to have a reasonable expectation that the six qualifying requirements for a standard authorisation are likely to be met.
16
Urgent Authorisations should normally only be used in response to sudden unforeseen needs. However they can also be used in care planning; for example, to avoid delays in transfer for rehabilitation, where delay would reduce the likely benefit of the rehabilitation.
The managing authority must keep a written record of any Urgent
Authorisations given, including details of why it decided to give an Urgent
Authorisation and give a copy to the individual and any other involved persons.
The managing authority will need to be able to show that they have made a reasonable decision based on their professional judgement and after taking into account all the relevant factors. For this process DoLS Form 1: The
Urgent Authorisation is to be used.
If there are exceptional reasons why the request for a Standard
Authorisation cannot be dealt with within the seven period day of the Urgent
Authorisation, the managing authority may ask the supervisory body to extend the duration of the urgent authorisation for a maximum of a further seven days .
For this purpose DoLS Form 2: Request for Extension to Authorisation is to be used.
Completed forms are forwarded, via the MCA Manager, to the nominated
Best Interests Assessor who forwards the request to the Authorised
Signatory (A deputy who acts on behalf of the Chief Executive or the
Director of Adults Social Services) for the appropriate supervisory body to decide whether circumstances exist for an extension to the authorisation.
The Authorised Signatory informs the managing authority of the outcome of the decision regarding the extension, the relevant person, the Best Interests
Assessor and any other associated persons. For details regarding who is the Authorised Signatory for the supervisory body, see 7.59 to 7.66 of this document.
The supervisory body may only extend the duration of the Urgent
Authorisation if:
The managing authority has made a request for a standard authorisation
There are exceptional reasons why it has not yet been possible to make a standard authorisation, and
It is essential for the deprivation of liberty to continue while the supervisory body makes its decision.
To enable this process to be recorded the DoLS Form 3 should be completed by the Nominated Person for the supervisory body.
17
The Authorised Signatory for the supervisory body must notify the managing authority of the length of any extension granted, amend the original urgent authorisation so that it states the extended duration. Where possible the managing authority should ensure that the relevant person understands the effect of the authorisation and the right to challenge the decision.
Copies of the amended Urgent Authorisation should be given by the managing authority to the relevant person and all those also involved.
If the supervisory body does not extend the authorisation, it must inform the managing authority of its decision and the reasons for it using the same form.
The managing authority is responsible for ensuring that it does not deprive a person of their liberty without an authorisation. Where a request for an authorisation is refused, it will need to review the relevant person’s actual or proposed care arrangements to ensure that a deprivation of liberty is not allowed to either continue or commence. The Best Interests Assessor should advise the managing authority should they believe that an urgent review or strategy meeting is required.
Ensuring that the urgent review or strategy meeting takes place is the responsibility of the managing authority. Both the Named Assessor, as the case responsible person, and the Best Interests Assessor should be invited to attend.
Notifications:
The managing authority is responsible for submitting the following notifications:
- The Care Quality Commission must be notified at the time a DoLS application is submitted and, if authorised, at the time of authorisation
(including period of authorisation)
-
The Coroner’s Office must be notified if a person dies whilst they are under a DoLS authorisation
(A new Coroners Act came into force on 25 th July 2013. Within it there is a legal duty to inform the coroner of any death that has occurred whilst a person is subject to the deprivation of liberty safeguards.
The term death whilst in state detention is added to death in custody.
When the death is likely to be related to the trauma of being deprived of liberty there must now be a formal inquest with a jury. Failure to notify the coroner has potentially serious consequences.)
18
7.2 The Role of the Mental Capacity Act Manager –
The Application Process
The MCA Manager has the responsibility for receiving the applications from managing authorities, be it care home or hospital, acknowledging receipt of the application with the managing authority, recording the essential information onto the MCA database and forwarding the details on to an appropriate Best Interest Assessor.
In the event that the MCA Manager is unavailable, the Safeguarding Adults
Business Team will manage the DoLS referral process.
7.3 The MCA Manager
On receipt of the application from the managing authority, the MCA
Manager and MCADoLS support team (part of the Safeguarding Adults
Business Team) check the validity of the application and will refer the application back to the managing authority has not provided sufficient details. In the event of this occurring, the time scales for completion will start again on receipt of the new application from the managing authority.
On receipt of a completed application from a managing authority, the MCA
Manager identifies if the relevant person has somebody to support them who is not engaged in providing care or treatment in a professional capacity or for remuneration. If they do not, the MCADoLS support team will instruct an IMCA to support the relevant person.
The MCA Manager contacts the assessors to undertake the six qualifying assessments, the assessments to be carried out by the Best Interests
Assessor. The assessors will be a Best Interests Assessor and a Mental
Health Assessor, both of whom will have undertaken the relevant training to undertake their particular role.
In the event that an urgent authorisation is in place the MCADoLS support team will notify the assessors required to undertake the six assessments and any Independent Mental Capacity Advocate (IMCA) appointed of the seven day timescale in which the assessments need to be completed.
The MCADoLS support team will distribute standard letters, specifically when a standard authorisation is due to expire within 28 days.
19
7.4 The Six Assessments
As soon as the supervisory body has confirmed that the request for a standard authorisation should be pursued, it must obtain the relevant assessments to ascertain whether the qualifying requirements of the deprivation of liberty safeguards are met. Assessments must be completed within 21 days for a standard deprivation of liberty authorisation, or where an Urgent Authorisation has been given, before the urgent authorisation
(including any extension) has been given.
The six assessments that are required to be completed do not have to be completed by different assessors, however, there must be at least two assessors (fulfilling the criteria between 4.13 and 4.18 of the DoLS code of practice) and they must each make their own decisions.
The following table explains at a glance the type of assessment that is required, its purpose and who it should be undertaken by:
Type of Assessment Purpose of the Assessment
Age Assessment
No Refusals Assessment
Mental Capacity Assessment
Undertaken by anybody who is eligible to act as a Best Interests Assessor.
The purpose of the assessment is simply to confirm whether the relevant person is aged
18 or over.
Undertaken by anybody who is eligible to act as a Best Interests Assessor.
The purpose of the assessment is to establish whether an authorisation to deprive the relevant person of their liberty would conflict with another existing authority for decision-making for that person; such as a valid decision by a Court Appointed
Deputy or an advanced decision to refuse treatment.
Undertaken by anybody who is eligible to act as mental health assessor or a Best
Interests Assessor.
The purpose of the assessment is to establish whether the relevant person lacks capacity to decide whether or not they should be accommodated in the relevant care home or hospital to be given the care or treatment.
20
Mental Health Assessment
Eligibility Assessment
Best Interests Assessment
Undertaken by a doctor who is either approved under section 12 of the mental health act 1983, or is registered medical practitioner with at least three years’ relevant post registration experience and who have undertaken appropriate DoLS training.
The purpose of the assessment is to establish whether the relevant person has a mental disorder within the meaning of the
Mental Health Act 1983. This means any disorder or disability of mind, including learning disabilities although excluding dependence on alcohol or drugs. It is not an assessment to determine whether the relevant person requires mental health treatment but specifically if a disorder exists.
Undertaken by a mental health assessor who is also a section 12 doctor or a Best
Interests Assessor who is also an approved mental health practitioner – AMHP.
The purpose of the assessment is to clarify the relevant person’s status or potential status under the Mental Health Act 1983.
For example a person would not be eligible for a deprivation of liberty authorization if they are detained as a hospital inpatient under the Mental Health Act 1983 or if the authorisation, if given, would be inconsistent with an obligation placed on them under the
Mental Health Act 1983.
Undertaken by the Best Interests Assessor.
The purpose of the assessment is to establish if deprivation of liberty is occurring or is going to occur and if so, whether:
It is in the best interests of the relevant person to be deprived of their liberty
It is necessary for them to be deprived of liberty in order to prevent harm to themselves and
Deprivation of liberty is a proportionate response to the likelihood of the relevant person suffering harm and the seriousness of that harm.
21
The Act states that where an ‘equivalent assessment’ to any of these assessments has already been obtained, it may be relied upon instead of obtaining a fresh assessment.
An equivalent assessment is an assessment that:
has been carried out in the preceding 12 months, not necessarily for the purpose of a deprivation of liberty authorisation.
meets all the requirements of the deprivation of liberty assessment (it is
unlikely that all the requirements could be met for a Best Interests
Assessment), and
The supervisory body accepts and sees no reason why it should no longer be accurate.
In certain circumstances, it may not be necessary to carry out one or more of the six assessments. In such instances DoLS Form 11 is to be used, recording that a previous equivalent assessment has been used instead.
Should this form be used, any equivalent assessments should be securely attached to DoLS Form 11 by the assessor.
7.5 The Best Interests Assessor
The first task of the Best Interests Assessor is to establish whether deprivation of liberty is currently occurring or is going to occur within the next 28 days, since there is no point in the assessment process proceeding further if deprivation of liberty is not an issue.
If the Best Interests Assessor considers that deprivation of liberty is occurring or is likely to occur with 28 days they should start a full best interests assessment, involving the relevant person within the process as much as is possible and practical and helping them to participate within the decision-making.
In addition to undertaking their own assessments, the Best Interests
Assessor will be required to liaise with all the others assessors within the process (the mental health assessor and any others) as it is the responsibility of the Best Interests Assessor to collate their assessments and forward the conclusion of each, either individually or collectively to the
Authorised Signatory for the supervisory body.
Within the process of assessment, the Best Interests Assessor must involve the relevant person in the assessment process as much as is possible and practical, and help them to participate in decision-making.
The relevant person should be given the support needed by the Best
Interests Assessor to participate and the appropriate means for communication or language where applicable.
22
Within the process the Best Interests Assessor will need to consider:
Whether any harm to the person could arise if the deprivation of liberty does not take place?
What that harm would be?
How likely that harm is to arise – i.e. is the level of risk sufficient to justify a step as serious as depriving a person of their liberty?
What other care options are there which could avoid deprivation of liberty?
If deprivation of liberty is currently unavoidable, what action could be taken to avoid it in the future?
In addition the Best Interests Assessor should, as far as is practical and possible, seek the views of:
Anyone the relevant person has previously named as someone they want to be consulted
Anyone involved in caring for the person
Anyone interested in the person’s welfare (for example, family carers, other close relatives, or an advocate already working with the person) and
Any deputy representing the relevant person
The Best Interests Assessor is required to provide an independent and objective view of whether or not there is a genuine justification for deprivation of liberty, taking into account all the relevant views and factors.
If the Best Interests Assessment supports deprivation of liberty, the Best
Interests Assessor must state what the maximum duration should be within the case concerned, not exceeding in 12 months. The Best Interests
Assessor should:
Set out the reasons for selecting the period stated, and
Take into account any available indication of how likely it is that the relevant person’s circumstances will change, including the expected progression of illness or disability
The underlying principle is that the deprivation of liberty should be for the minimum period necessary so, for the maximum 12-month period to apply, the Best Interests Assessor will need to be confident that there is unlikely to be a change in the person’s circumstances that would affect the authorisation within that timescale.
The Best Interests Assessor must provide a report that explains their conclusion and give reasons for it. They must state in their assessment the name and address of every interested person whom they have consulted in carrying out the assessment. Family and friends may not be confident about expressing their views and it is the responsibility of the Best Interests
23
Assessor to enable them to do so – using support to meet communication or language needs as necessary.
NOTE: If translators are required, independent translators should be instructed.
Family members should not act as interpreters for other members of their family.
If the Best Interests Assessor does not support deprivation of liberty, then their report should aim to be as useful as possible to the providers of care in deciding on future action and care provision. A copy of the report should be included in the relevant person’s care plan or case notes to ensure that their views about how deprivation of liberty can be avoided are made clear to the providers of care and relevant staff.
If it appears that the relevant person is being deprived of their liberty, the
Best Interests Assessor should recommend someone to be appointed as the Relevant
Person’s Representative although their appointment cannot however take place unless an authorisation is given by the supervisory body.
As soon as possible after carrying out their assessments, the Best Interests
Assessor must provide a report that explains their conclusions and their reasons for it. In addition they must collate the assessments from all the assessors within the process and give copies of these along with their report to the nominated representative for the supervisory body so that the authorisation for a deprivation of liberty, with timescales and conditions attached, can be finalised.
7.6 The Authorised Signatory for the Supervisory Body
If all the assessments in the standard authorisation assessment process indicate that the relevant person meets all the qualifying requirements, then the supervisory body must give a deprivation of liberty authorisation. DoLS
Form 12 is to be used for this process.
An Authorised Signatory is appointed for the respective supervisory body who may attach conditions to the authorisation.
The power of authorisation should be assigned to a senior level, acting on behalf of the Chief Executive for Health and the Director of Adult Social
Services for the Local Authority.
The supervisory body must set the period of the authorisation, which may not be longer than that recommended by the Best Interests Assessor. It may be beneficial for the Best Interests Assessor to brief the Authorised
Signatory for the supervisory body either by telephone or face-to-face in order to enable them to raise any questions that may arise and to enable them to complete this process.
24
Note: Any meeting which is required to be undertaken will need to be within the allocated timescales and must not delay the process.
As soon as possible after giving the authorisation, the Authorised Signatory for the respective supervisory body must forward a copy of the authorisation to The MCA Manager to distribute copies to:
The managing authority
The relevant person
The Relevant Person’s Representative
Any Independent Mental Capacity Advocate (IMCA) instructed for the purpose in relation to the relevant persons detention and
Every interested person named by the Best Interests Assessor in their report as somebody they have consulted in carrying out their assessment.
If any of the assessment concludes that one of the requirements is not met, then the assessment process should stop immediately and authorisation may not be given. The nominated person for the respective supervisory body must forward a copy of the decision to the MCA Manager to distribute copies to:
Inform anyone still engaged in carrying out an assessment that they are not required to complete it
Notify the managing authority, the relevant person, any IMCA involved and every interested person consulted by the Best Interests
Assessor that authorisation has not been given
The DoLS Form 13 is to be completed within this process by the Authorised
Signatory for the supervisory body.
On completion of the process, the Authorised Signatory should arrange for all the assessments, forms and the Best Interests Assessors report to be returned to the MCADoLS Support Team so that a record can be kept of all the applications which have been received.
25
7.7 The Independent Mental Capacity Advocate – IMCA
If there is nobody appropriate to consult, other than people engaged in providing care or treatment for the relevant person in a professional capacity or for remuneration, the managing authority must highlight this in
Section B9 of DoLS Form 4 (the Request For A Standard Authorisation
Form). Should this be highlighted, The MCA Manager must instruct an
IMCA on receipt of the form, to represent the relevant person. It is particularly important that the IMCA is instructed quickly if an urgent application is to be made.
A friend or family member is not considered to be acting in a professional capacity simply because they have been appointed as the person’s representative for a previous application.
An IMCA instructed at this initial stage of the deprivation of liberty safeguards process has additional rights and responsibilities compared to an IMCA more generally instructed under the Mental Capacity Act 2005.
IMCAs in this context have the right to:
Give information or make submissions to assessors, which assessors must take into account in carrying out their assessments
Receive from the supervisory body any copies of any deprivation of liberty assessments that are undertaken
Receive a copy of the outcome of the authorisation of deprivation of liberty, if authorised.
Be notified by the supervisory body if they are unable to authorise an application for a deprivation of liberty.
Apply to the Court of Protection for permission to take the relevant person’s case to the Court in connection with a matter relating to the giving or refusal of a deprivation of liberty by a supervisory body.
An IMCA will need to familiarise themselves with the circumstances of the person to whom the deprivation of liberty safeguards are being applied, and to consider what they may need to tell any of the assessors during the course of the assessment process. They will also need to consider whether they have any concerns about the outcome of the assessment process.
Differences of opinion between an IMCA and an assessor should ideally be resolved while the assessment is still in progress. Where there are significant disagreements between an IMCA and one or more of the assessors that cannot be resolved between them, the nominated person for the supervisory body should be informed by the Best Interests Assessor,
IMCA or MCA Manager before the assessment is finalised. The nominated person for the supervisory body should then consider what action might be appropriate. The objective should be, wherever possible, to resolve differences of opinion informally in order to minimise the occasions on which it is necessary for an IMCA to make application to the Court of Protection.
26
The IMCA and Relevant Persons Representative (RPR) service is provided by Cloverleaf Advocacy. All IMCA and RPR referrals should be made directly to the service via post or via telephone. See contact details below:
Cloverleaf Advocacy
1 st Floor
Wellington Road
DEWSBURY
WF13 1HF
Telephone: 01924 454875
Fax:. 01924 438444
8. WHAT IF AN APPLICATION FOR A DEPRIVATION OF LIBERTY IS REFUSED?
The managing authority is responsible for ensuring that the relevant person is not deprived of their liberty without an authorisation being approved by the supervisory body.
The supervisory body is responsible for ensuring that any care package is commissioned in compliance with the Code of Practice for the Mental Capacity Act
2005, and doesn’t include an inappropriate deprivation of liberty.
The actions that both managing authorities and commissioners of care should consider if a request is turned down will depend on the reason why the authorisation has not been given.
If the Best Interests Assessor concluded that the person was not in fact being, or going to be, deprived of liberty, no action is likely to be necessary
If the Best Interests Assessor concluded that the proposed deprivation of liberty was not in the person’s best interests, the registered person of the managing authority (in conjunction with the commissioner of the care) will need to consider how the care plan could be changed to avoid deprivation of liberty. They should examine carefully the reasons given in the Best Interests
Assessor’s report and may find it helpful to discuss the matter with the Best
Interests Assessor.
Where appropriate, they should also discuss the matter with family and carers. If the person is not yet a resident in the care home or hospital, the revised care plan may not involve admission to that facility.
If the mental capacity assessor concluded that the person has capacity to make decisions about their care, the managing authority will need to consider, in conjunction with the supervisory body, how to support the person to make such decisions.
If the person does not have a mental disorder, the care plan will need to be modified to avoid a deprivation of liberty.
Where there is a valid refusal by an attorney or deputy or an applicable and valid advance decision, alternative care arrangements will need to be made.
If there is a question about the refusal, a decision may be sought from the
Court of Protection.
If the person is under 18, use of the Children Act 1989 may be considered.
27
Where the Best Interests Assessor comes to the conclusion that the best interests requirement is not met, but if it appears to the Best Interests Assessor that the relevant person is already being deprived of their liberty, the Best Interests
Assessor must inform the Authorised Signatory for the supervisory body and explain in their assessment why they have reached that conclusion.
The supervisory body will need to liaise with the managing authority in order to ensure that a deprivation of liberty is not permitted to continue in the absence of an appropriate application having been made.
The person’s care plan and the provision of care must be reviewed immediately and the changes made as soon as possible. The steps taken to end the deprivation of liberty should be recorded in the care plan. Where possible it will be important to involve family, friends and carers in speedily deciding how to prevent the unauthorised deprivation of liberty from continuing.
It is the responsibility of the registered person of the managing authority to comply with the law in this situation and it will need to keep the person’s care under review to ensure that unlawful deprivation of liberty does not arise in future.
Should the supervisory body have continuing doubts about the matter, it should alert the Care Quality Commission (CQC) who can be contacted at the following address:
CQC National Customer Service Centre
Citygate
Gallowgate
Newcastle upon Tyne
NE1 4PA
Telephone: 03000 616161
Additional contact details are provided on the CQC website: http://www.cqc.org.uk/content/contact-us
9.
THE ROLE OF THE RELEVANT PERSON’S REPRESENTATIVE
Once a standard authorisation has been granted, a Relevant Person’s
Representative must be appointed by the Best Interests Assessor as soon as possible to represent the person who has been deprived of their liberty.
The Best Interests Assessor must appoint a Relevant Person’s Representative for every person in respect of whom a standard authorisation for deprivation of liberty is issued. The representative is appointed at the time the authorisation is granted or very shortly thereafter.
28
The role of the Relevant Person’s Representative, once appointed, is:
to maintain contact with the relevant person and visit at least once every fortnight, and
to represent and support the relevant person in all matters relating to the operation of the deprivation of liberty safeguards, including, if appropriate, triggering a review, using an organis ations’ complaints procedure on the person’s behalf or making an application to the Court of Protection.
Note: This is a crucial role in the deprivation of liberty process, providing the relevant person with representation and support that is independent of the commissioners and providers of the services they are receiving.
The managing authority’s responsibilities toward the Relevant Person’s
Representative
Immediately after a standard authorisation has been issued, the managing authority must take all practical and appropriate steps to ensure that the relevant person and their representative understand:
the effect of the authorisation
their right to request a review
the formal and informal complaints procedures that are available to them
their right to make an application to the Court of Protection to seek a variation or termination of the authorisation, and
their right to request the support of an IMCA.
In providing information to the relevant person and their representative, the managing authority should take account of the communication and language needs of both the relevant person and their representative. Provision of information should be seen as an ongoing responsibility rather than a one-off activity.
9.1
Who can be a Relevant Person’s Representative?
To be eligible as a Relevant Person’s Representative, a person must be:
18 years of age or over
willing to be appointed, and
able to keep in contact with the relevant person.
The person must not be:
prevented by ill health from carrying out the role of representative
financially interested in the relevant person’s managing authority
a close relative of a person who is financially interested in the care home or the hospital
29
if the person is deprived of liberty in a care home or hospital, employed by, or providing services to, that care home or hospital
employed to work in the relevant person’s supervisory body in a role that is, or could be, related to the relevant person’s case.
The appointment of a Relevant Person’s Representative is in addition to, and does not affect, any appointment of an attorney or deputy. The functions of the representative are in addition to, and do not affect, the authority of any attorney, the powers of any deputy or any powers of the court.
There is no presumption that a relevant person’s representative should be the same as the person who would be their nearest relative for the purposes of the Mental Health Act 1983, even where the person is likely to be subject simultaneously to an authorisation under this procedure and a provision of the Mental Health Act 1983.
10. INSTRUCTING AN IMCA TO ACT DURING A STANDARD AUTHORISATION
FOR A DEPRIVATION OF LIBERTY, WHEN THERE IS NO RELEVANT
PERSON’S REPRESENTATIVE AVAILABLE
A person who is being deprived of their liberty will be in a particularly vulnerable position during any gaps in the appointment of a relevant person’s representative, since there may be nobody to represent their interests or to apply for a review on their behalf. In these circumstances, if there is nobody who can support and represent the person (other than a person engaged in providing care and treatment for the relevant person in a professional capacity or for remuneration), the managing authority must notify the supervisory body, who must instruct an
IMCA to represent the relevant person until a new representative is appointed.
At any time when the relevant person does not have a representative, it will be particularly important for supervisory bodies to consider exercising their discretion to carry out a review if there is any significant change in the person’s circumstances.
In North East Lincolnshire, the IMCA Service is provided by Cloverleaf Advocacy
Service.
Cloverleaf can be contacted at the following address and contact numbers:
Cloverleaf Advocacy
1 st Floor
9 Wellington Road
DEWSBURY
WF13 1HF
Telephone: 01924 454875
Fax: 01924 438444
Email: imca@cloverleaf-advocacy.co.uk
30
11. INSTRUCTING AN IMCA TO ACT DURING A STANDARD AUTHORISATION
FOR A DEPRIVATION OF LIBERTY TO SUPPORT THE RELEVANT PERSON
OR THEIR REPRESENTATIVE
It is the responsibility of the supervisory body to instruct an IMCA if the relevant person or their representative requests one. This task will be undertaken by the
MCA Manager. The intention is to provide extra support to the relevant person or a family member or friend acting as their representative if they need it, to make use of the review or court of protection safeguards. If the person already has a paid
‘professional’ representative, the need does not arise and so an IMCA would not be provided.
Note: In any deprivation of liberty application, only one IMCA will be appointed.
The role of the IMCA is to explain the authorisation to them: what it means, why it has been granted, why it is considered that the person meets the criteria for authorisation, how long it will last and how to trigger a review or challenge in the
Court of Protection. The IMCA can provide support with a review or with an application to the Court, for example to help the person to communicate their views.
The IMCA will have the right to make submissions to the supervisory body on the question of whether a qualifying requirement is reviewable or to give information, or make submissions, to any assessor carrying out a review assessment. Both the relevant person and their representative must be told about the IMCA service and how to request an IMCA.
An IMCA must be instructed if the person or their representative requests this provision. A request may be made more than once during the period of the authorisation. For example, help may be asked for at the start of the authorisation and then again later in order to request a review.
In addition, if the supervisory body has reason to believe that the review and deprivation of liberty safeguards might not be used without the support of an IMCA, then they must instruct an IMCA. For example, if the supervisory body is aware that the person has selected a representative who needs support with communication, it should consider whether an IMCA is needed.
12. REQUESTS FROM A THIRD PARTY FOR AN APPLICATION FOR AN
AUTHORISATION FOR A DEPRIVATION OF LIBERTY
The safeguards include procedures for responding to situations where an individual believes that someone in a care home or hospital is being deprived of their liberty but without proper authorisation. If an individual believes that someone is being deprived of their liberty without proper authority, the Act allows for them to ask the managing authority to request a standard authorisation. The individual may do this using DoLS Letter 1- Letter to the Managing Authority.
If the managing authority does not then request a standard authorisation “within a re asonable period” the individual may ask the supervisory body to decide whether or not there is an unauthorised deprivation of liberty. The individual may do this using DoLS Letter 2
– Letter to the supervisory body.
31
NOTE: The use of these letters is not mandatory, however any oral or written request should include the information highlighted in bold within the letter template.
In such instances this letter would be forwarded to the MCA Manager, the details inputted and recorded onto the MCA database and then the standard authorisation process would be followed from this point in accordance with the process akin to an application via a standard authorisation form.
If a request is received via the DoLS email address or via fax, the relevant persons details and the minimum data is recorded on the MCA database. The request to assess whether or not there is an unauthorised deprivation of liberty should be completed by MCA Project Manager and recorded on DoLS Form 16 - Record of
Supervisory Bodies Action on Receipt of Notification of a Possible Unauthorised
Deprivation of Liberty.
If it is felt that the request is not frivolous or vexatious or the issue has already been decided by the supervisory body and there have been no changes in the relevant person’s circumstances since the issue regarding deprivation of liberty was last decided, then an assessment will be required.
The decision regarding whether the request is frivolous or vexatious will be undertaken by the Authorised Signatory for the supervisory body. A Best Interests
Assessor will need to be commissioned to undertake a report of the situation and will need to record their findings using DoLS Form 17
– Unauthorised Deprivation of Liberty Assessors Report.
On receipt of DoLS Form 17, the Authorised Signatory for the supervisory body will need to complete DoLS Form 18 – Supervisory Body’s Decision Following the
Receipt of an Unauthorised Deprivation of Liberty Assessors Report.
If the relevant person is subject to an authorised deprivation of liberty, the following steps must be taken:
The managing authority is deemed to have requested a standard authorisation in relation to the relevant person.
The managing authority therefore must provide the supervisory body with the information that is required whenever such a request is actually made. It must now complete DoLS Form 4 and send it to the supervisory body, via email, fax or post.
The Best Interests Assessor, Section 12 doctor, IMCA and the six assessments will be arranged by the MCA Manager, on behalf of the supervisory body as the completed DoLS Form 4 will have triggered a request for a standard authorisation.
The present care and/or treatment has been found to amount to deprivation of liberty. If the managing authority considers that this care and/or treatment should continue while the assessments are carried out, it must give itself an urgent authorisation by completing DoLS Form 1
If an urgent authorisation form is issued then the necessary assessments must be completed within the period of the urgent authorisation.
32
13. REVIEWS
The managing authority must set out in the care plan clear roles and responsibilities for monitoring the DoLS and confirm under what circumstances a review is necessary. For example, if a person’s condition is changing frequently, then their situation should be reviewed more frequently. In addition, the supervisory body must carry out a review if requested to do so by the relevant person or their representative, or the managing authority may also carry out a review at any other time. There are no restrictions on when a review can be requested.
In general, the grounds for requesting a review are that:
The relevant person’s circumstances have changed from those which formed the basis of the original application.
The person is ineligible because they now object to receiving mental health treatment in hospital
There has been a change in the relevant person’s situation and, because of the change, it would be appropriate to vary the authorisation.
NOTE: A standard authorisation only permits deprivation of liberty: it does not mean that a person has to be deprived of liberty. If a care home or hospital identifies that deprivation of liberty is no longer necessary then they must end it immediately, by adjustment of the care regime or whatever other change is appropriate. They should then apply to the supervisory body to apply to discharge the authorisation. While this review is happening, the person concerned should no longer be subject to deprivation of liberty.
The supervisory body must carry out a review (known as a part 8 Review
– as it is covered with Chapter 8 of the DoLS Code of Practice) if one is requested by the relevant person, by their representative or by the managing authority. The following letters and form should be used by the identified person if a review is requested:
DoLS Letter 3
DoLS Letter 4
– Review requested by the Relevant Person
– Review requested by the Relevant Persons Representative
DoLS Form 19
– Review requested by the managing authority
NOTE: The use of these letters is not mandatory. A request may be made orally, by a different letter of the person’s choosing or in any other way that the person wishes. Receipt of these forms should be recorded on the MCA database held by the supervisory body.
The supervisory body may itself decide to carry out a review without any request being made for one. If it decides to hold a review without a request being made it should use DoLS Form 20 – Supervisory Body Notifies Relevant Interested
Parties.
33
This form is used to give notice that a review is to be carried out, whether because a request has been received or because the supervisory body itself has decided to conduct one. This form is to be issued by the Authorised Signatory but they may delegate this responsibility to another appropriate person in certain circumstances.
Having given notice that a review is to be held, the supervisory body must then decide whether any of the qualifying assessments are reviewable. In essence what must be decided is whether evidence exists that the relevant person may no longer meet the criteria for being deprived of their liberty under the Mental Capacity Act
2005. In general a review should be carried out if it is possible that the relevant person no longer meets one or more qualifying assessments.
With one exception, the supervisory body must arrange for fresh assessments to be carried out for each qualifying requirements that appears to be reviewable. The exception is where it has been decided that the best interest’s requirement is reviewable on the sole ground that there has been a change in the person’s case as a result of which the conditions of the standard authorization need varying. This process would need to be undertaken by a commissioned Best Interests Assessor and signed off by the Authorised Signatory for the supervisory body. This may not necessarily be the same Best Interests Assessor who undertook the original assessments.
The DoLS Form 21
–
Supervisory Body Records Its Decision as to Whether any
Qualifying Requirements are Reviewable should be used for this process.
Where the supervisory body arranges fresh assessments relating to one or more of the qualifying requirements, these assessments are called “Review
Assessments.” However the assessments are recorded using the same forms that are used to assess a relevant person following a request for a new standard authorisation.
These forms are:
DoLS Form 5 – Age Assessment
DoLS Form 6 – Mental Health Assessment
DoLS Form 7
– Mental Capacity Assessment
DoLS Form 8
– No Refusals Assessment
DoLS Form 9 – Eligibility Assessment
DoLS Form 10 – Best Interests Assessment
The supervisory body should use DoLS Form 22
– Supervisory Body’s Decision
Following Receipt of Review Assessments to record its decision following the receipt of the review assessments. This would need to be completed by the nominated person for the supervisory body.
Any termination of the standard authorisation should be recorded by the
Authorised Signatory for the supervisory body using DoLS Form 23 – Supervisory
Body gives notice that a Standard
Authorisation has ceased to be in force.
34
The reasons why a standard authorisation will cease to be in force are that:
The care home or hospital gave notice to the supervisory body that the relevant person has ceased to meet the eligibility requirement. 28 days have now elapsed since the notice was given without the suspension having been lifted.
The standard authorisation has expired.
A review of the standard authorisation has been completed and the review concluded that the relevant person no longer meets the requirements for being deprived of their liberty under the Mental Capacity Act 2005.
Following a change in the place where the person was deprived of liberty, the standard authorisation has been replaced by a new standard authorisation and has therefore ceased to exist.
The Court of Protection or another applicable court has made an order that the standard authorisation is invalid or that it shall no longer have effect.
The relevant person has died.
Once a standard authorisation comes to an end, the managing authority cannot lawfully continue to deprive a person of their liberty. If they consider that a person will still need to be deprived of liberty after the authorisation ends, they need to request a further application to begin immediately after the expiry of the existing one, recognising that the process to complete a further authorisation can take up to 21days.
Once commenced, the process for re-application follows the same process for requesting the previous authorisation, with the same assessment processes needing to take place.
However, the need to instruct an IMCA will not usually arise because most people at this stage will already have a person appointed to represent their interests.
14. RECORD KEEPING
It is essential that full records of assessments and decision making, including the identity or identities of decision maker(s) are kept and that the relevant forms are retained on the MCA database used by the supervisory bodies recording systems and on the records of the managing authorities. This will also include those forms which were completed and where the application for a deprivation of liberty was not authorised. See Appendix 4 for the Mental Capacity Act Record.
15. ADDITIONAL DoLS FORMS
The remaining forms which could be used as part of the DoLS process are included within this section with a brief explanation of their usage:
DoLS Form 14 – Suspending a Standard Authorisation
35
Used when a resident is subject to a standard authorisation under the Mental
Capacity Act 2005 and a Mental Health Act 1983 section or order that may conflict with it in some way. The law provides that the Mental Health Act 1983 powers generally take priority over Mental Capacity Act 2005 powers. Completed by the managing authority and forwarded to the Authorised Signatory for the supervisory body. The effect of DoLS Form 14 is that the existing authorisation no longer authorise the managing authority to deprive the relevant person of their liberty.
•
DoLS Form 15
– Notice that a Suspension has been lifted
Used when the managing authority identify that the relevant person becomes eligible to be deprived of their liberty within 28 days of DoLS Form 14 being issued.
Completed by the managing authority and forwarded to the Authorised Signatory for the supervisory body. In the event that the managing authority is unaware of the identity of the Authorised Signatory for the supervisory body, then they should forward either of these forms to the MCA Manager to forward on their behalf.
Likewise it would be good practice to inform the Best Interests Assessor of these developments, so that it can be recorded on the respective recording systems of each supervisory body together in a way that minimises the burden on the person being assessed.
However, in the interests of ensuring that an appropriate degree of objectivity is brought to the assessment process, and to avoid the risk that arbitrary decisions will be taken about deprivation of liberty:
There must be a minimum of two assessors, e.g. Best Interests Assessor and doctor who has carried out Mental Health assessment.
The mental health and Best Interests Assessors must be different people.
The Best Interests Assessor can be an employee of the supervisory body or managing authority, but must not be directly involved in the care or treatment of the person that they are assessing nor in decisions about their care.
A potential Best Interests Assessor should not be used if they provide treatment or care to the relevant person or are in a line management relationship with the professional proposing the deprivation of liberty or the mental health assessor.
None of the assessors may have a personal financial interest in the care of the person they are assessing.
The assessor must not be a close relative of the person being assessed or a close relative of a person with a personal financial interest in the person’s care.
Where the managing authority and supervisory body are both the same body, the supervisory body may not select to carry out a best interests assessment a person who is employed by the body or providing services to it.
36
16. CONTACT DETAILS
For more information of the deprivation of liberty safeguards, or any other issues relating to the Mental Capacity Act (2005), please contact:
The NEL Mental Capacity Act Support Team
Telephone: 01472 232244
Email: focus.mcadols@nhs.net
37
APPENDIX A
OVERVIEW OF THE DEPRIVATION OF LIBERTY SAFEGUARDS PROCESS
Hospital or Care Home Managers identify those at risk of deprivation of liberty and request authorisation from supervisory body
Age
Assessment
Mental Health
Assessment
Assessments commissioned by supervisory body. IMCA instructed for anyone without representation
Mental Capacity
Assessment
Best Interests
Assessments
No Refusals
Assessment
Eligibility
Assessment
Authorisation Expires and
Managing Authority
Requests Further
Any
Assessments
Says No
All Assessments
Support
Authorisation
Authorisations
Request for Authorisation
Declined
Best Interests Assessor
Recommends Period for
Which Deprivation of
Managing Authority Requests Review
Because Circumstances Change
Liberty should be authorised
Authorisation Is Given and
Person’s Representative
Appointed
Authorisation Implemented By
Managing Authority
Best Interest Assessor
Recommends Person to Be Appointed As
Representative
Person or Their Representative Request
Reviews
In urgent situations, a hospital or care home can give an urgent authorisation for seven days while obtaining a standard authorisation
Person or Their
Representative
Applies To Court Of
Protection, Which
Has Powers to
Terminate
Authorisation or
Vary Conditions
Review
APPENDIX B
SUPERVISORY BODY ACTION ON RECEIPT OF A REQUEST FROM A MANAGING AUTHORITY OR AN ELIGIBLE PERSON TO
DETERMINE WHETHER OR NOT THERE IS A CURRENT UNAUTHORISED DEPRIVATION OF LIBERTY
REQUEST RECEIVED
Supervisory body makes and keeps written record of request.
FROM A MANAGING AUTHORITY
Is the application valid and complete?
Yes - Does the person have somebody not engaged in providing care or treatment in a professional capacity or for remuneration to support them?
Yes
No - Refer back to managing authority for necessary action/to provide further information. Restart application process on receipt of revised application/further information
NO - Supervisory body must instruct a section 39A IMCA.
Supervisory body to appoint assessors to assess the six qualifying requirements
(no need to assess any qualifying requirement in respect of which a valid equivalent assessment is available). Supervisory body gives the best interests’ assessor any relevant needs assessment or care plan drawn up by them or on their behalf.
FROM AN ELIGIBLE PERSON
Has the person asked the managing authority to apply for an authorisation and the managing authority not done so within a reasonable period?
Yes - Is the request frivolous or vexatious, or has the question whether or not there has been an unauthorised deprivation of liberty already been decided with no subsequent change of circumstances?
No - Supervisory body to select a person suitable and eligible to carry out a best interests' basement to assess whether or not there is an unauthorised deprivation of liberty. The assessment must be completed within 7 days.
No - Refer the matter back to the eligible person to approach the managing authority.
Yes - Notify the eligible person, the person to whom the request relates, and the managing authority that the supervisory body has been asked to decide whether or not there is an unauthorised deprivation of liberty but that it is not to be pursued.
Is an urgent authorisation in force? Doe the person have somebody not engaged in providing care or treatment in a professional capacity or for remuneration to support them
39
No – Assessments must be completed within 21 days from the date the supervisory body receives the request for an authorisation.
Yes - Assessments must be considered with in the period of the urgent authorisation, including any extension granted by the supervisory body.
Yes No - Supervisory body must instruct a section 39A IMCA
All assessments positive and supervisory body has written assessment.
Any assessment negative.
Supervisory body gives authorisation in writing specifying the period of the authorisation (no longer than recommended by the best interest assessor) and any conditions that apply.
Supervisory body appoints relevant persons representative – the person recommended by the best interests assessor or, if no recommendation, a (paid) relevant person’s representative.
Assessment process ceases.
Supervisory body refuses authorisation and notifies the managing authority, the relent person, any section 39A IMCA and every interested person consulted by the best interest’s assessor.
Supervisory body gives a copy of the authorisation to the relevant person’s representative, the managing authority, the relevant person, any section 39A IMCA and every interested person consulted by the best interest’s assessor.
Supervisory body makes and keeps a written record of request’s for standard authorisations in respect of which they have not given an authorisation
Supervisory body to notify the eligible person, the person to whom the request relates, the managing authority and any section 39A IMCA of the decision and who has been appointed to undertake the assessment
Does assessment confirm that there is a deprivation of liberty?
Yes
No
- Is the deprivation of liberty already authorised?
No - Supervisory body to notify the outcome of the assessment, and to give copies of the assessment, to the eligible person, the person to whom the request relates, the managing authority and any section 39A IMCA
Yes – Supervisory body top notify the outcome of the assessment, and to give copies of the assessment, to the eligible, the person to whom the request relates, the managing authority and any section 39A IMCA
Supervisory body makes and keeps a written record of the standard authorisations they have given and in respect of each authorisation:
the name of the relevant person
the name of the relevant hospital or care home
the period during which the authorisation is to be in force
the purpose for which the authorisation is given
any conditions subject to which the authorisation is given, and
the reason why each qualifying requirement is met
Supervisory body to notify the outcome of the assessment to the eligible person, the person to whom the request relates, the managing authority and any section 39A IMCA.
The managing authority must supply the supervisory body with the information that the managing authority would have had to include in a request for a standard authorisation
Action must continue as if a request for a standard authorisation had been received from a managing authority.
40
APPENDIX C
A
CHECKLIST FOR MANAGING AUTHORITY
SELF URGENT DoL AUTHORISATION
Name of relevant person: ……………………………….……………..……..………………….
Name of Managing Authority: …..………………………………………………….………………...
Name of person making application: …………………………….………………………………….
Date application made and sent to Supervisory Body: ……………………………………...
GIVING SELF URGENT DoL AUTHORISATION YES NO
Has Form 1 been received?
Has the Form been signed?
Has the form been dated?
Has each box been completed as appropriate?
If answer is ‘no’ to any question, contact person who completed form.
If answer is ‘yes’ to each question, then progress.
Has a copy of Form 1 been given to person deprived of their liberty
Has a copy of From 1 been given to any IMCA appointed?
Has a letter been sent to the person deprived of their liberty outlining the effect of the DoL and their right to make application to the Court of
Protection?
Has a copy of Form 1 been filed in a separate DoLS folder to be kept with patient’s case notes?
Has a copy of Form 1 been sent to central location for audit/monitoring purposes?
Has original Form 4 been sent to the Supervisory Body?
NB In exceptional circumstances when it has not been possible for a standard authorisation to be completed then Form 2 should be completed
(request for extension).
Has Form 2 been completed?
Has Form 2 been signed?
Has Form 2 been dated?
Has Form 2 been faxed immediately to Supervisory Body?
Has original Form 2 been posted to Supervisory Body?
Has a copy of Form 2 been filed in a separate DoLS folder to be kept with patient’s case notes?
Has a copy of Form 2 been sent to central location for audit/monitoring purposes?
Have details been entered in part H of Form 1?
Has copy of amended Form 1 been given to the person DoL?
Has copy of amended Form 1 been given to any IMCA appointed?
B
CHECKLIST FOR MANAGING AUTHORITY
STANDARD AUTHORISATION
Name of relevant person: ……………………………….……………..……..………………….
Name of Managing Authority: …..………………………………………………….………………...
Name of person making application: …………………………….………………………………….
Date application made and sent to Supervisory Body: ……………………………………...
REQUEST FOR STANDARD AUTHORISATION YES NO
Has Form 4 been completed?
Has the Form 4 been signed?
Has the Form 4 been dated?
Has each box been completed as appropriate?
If answer is ‘no’ to any question, revisit the form and complete.
If answer is ‘yes’ to each question, then progress.
Send Form to Supervisory Body at Swinton Grange.
Has BIA made contact?
Has discussion taken place whether it is restriction or DoL?
Has alternative care regimes been considered?
Have you received a copy of Form 12 (DoL authorisation).
If answer is ‘yes’ then
Have you informed relevant parties as outlined in 12.19 & 12.20 of procedure?
Has a copy of Form 4 been filed in a separate DoLS folder, to be kept with patient’s case notes?
Has a copy of Form 4 been sent to central location for audit/monitoring purposes?
NB If standard authorisation is NOT granted, then a Form 13 will be issued and forwarded to the Managing Authority. This should be filed in the relevant section of the person’s case notes.
42
C
CHECKLIST FOR MANAGING AUTHORITY –
SUSPENDING AN AUTHORISATION
Name of relevant person: ……………………………….……………..……..………………….
Name of Managing Authority: …..………………………………………………….………………
Name of person reporting suspension:…………………………….………………………………..
Date of Mental Health Act detention; or date of new conditions to an existing MHA Section eg., Community Treatment Order or Guardianship: ……………………………………………….
(Reasons might be where the DoLS specify residence at a particular hospital/care home and the CTO or Guardianship specifies residence at a different hospital/care home).
(Initials in these columns rather than a tick)
CHECKLIST - SUSPENDING AN AUTHORISATION YES NO
Have papers detaining the relevant person under a Section of the
Mental Health Act been completed and received on behalf of the
Hospital Managers OR has Guardianship been agreed with the
Director of Social Services?
If no, then DoL continues.
If yes, then proceed as follows:-
Has Form 14 been completed?
Has Form 14 been signed?
Has Form 14 been dated?
Has the Form 14 been faxed to the Supervisory Body?
Has the original Form 14 been sent to the Supervisory Body?
Has a copy of Form 14 been filed in a separate DoLS folder, to be kept with patient’s case notes?
Has a copy of Form 14 been sent to central location for audit/monitoring purposes?
Has a copy of Form 14 been given to the relevant person?
Has a copy of the Form 14 been given to the relevant person’s representative?
43
D
CHECKLIST FOR MANAGING AUTHORITY –
NOTICE THAT SUSPENSION HAS BEEN LIFTED
Name of Managing Authority: …..………………………………………………….…………
Name of person making application: …………………………….………………………….
Date of Mental Health Act detention or date of new conditions to an existing MHA Section eg., Community Treatment Order or Guardianship: …………………………………………..
(Reasons might be where the DoLS specify residence at a particular hospital/care home and the CTO or Guardianship specifies residence at a different hospital/care home).
Date suspension lifted: …………………………………………………………
(NB: suspension can only be lifted within 28 calendar days, inclusive of the original Mental
Health Act detention/conditions).
(Initials in these columns rather than a tick)
NOTICE THAT SUSPENSION HAS BEEN LIFTED YES NO
Is the person no longer subject to detention under the Mental Health
Act or conflicting conditions attached to CTO or Guardianship etc.
Is it less than 28 days from the original suspension of DoL authorisation?
If ‘no’ to either of the above questions, then DoLS authorisation comes to an end.
If ‘yes, then progress as follows:
Has Form 15 been completed?
Has Form 15 been signed?
Has Form 15 been dated?
Has Form 15 been faxed to the Supervisory Body?
Has original Form 15 been send to the Supervisory Body?
Has a copy of Form 15 been filed in a separate DoLS folder, to be kept with patient’s case notes?
Has a copy of Form 15 been sent to central location for audit/monitoring purposes?
44
E
CHECKLIST FOR MANAGING AUTHORITY –
REQUEST FOR A REVIEW BY MA
Name of relevant person: ……………………………….……………..……..…………
Name of Managing Authority: …..………………………………………………….…………
Name of person making application: …………………………….………………………….
Date of planned formal review: …………………………………………………………………
(Initials in these columns rather than a tick)
CHECKLIST – REQUEST FOR A REVIEW BY MA YES NO
Does the Managing Authority believe a DoL is no longer required?
If yes:-
Has care plan been adjusted or changes implemented?
Has Form 19 been completed?
Has Form 19 been signed?
Has Form 19 been dated?
Has Form 19 been faxed to Supervisory Body?
Has original Form 19 been sent to Supervisory Body?
Has a copy of Form 19 been filed in a separate DoLS folder, to be kept with patient’s case notes?
Has a copy of Form 19 been sent to central location for audit/monitoring purposes?
45
F
CHECKLIST FOR SUPERVISORY BODY –
STANDARD AUTHORISATION
Name of relevant person:……………………………….……………..……..………………...…
Name of Managing Authority: …..………………………………………………….…………
Name of person making application:…………………………….……………….………………….
Date application made by Managing Authority : …………………………………………..……..
Date received by Supervisory Body: …………………………………………………………
Check Part C (C1) – page 10 of Form 4.
Is the patient
‘ordinarily resident’ within North
Yorkshire & York
PCT?
No
Yes
Contact the appropriate
Supervisory Body and advise them the MA has inadvertently sent the forms to our SB.
Follow checklist below.
Ask them if they wish NHSNYY to act on their behalf. If so, commence assessment process.
(PCT-PCT protocol will be used -
Contact MCA and DoL Lead). If they wish to follow up themselves, make arrangements to forward papers to them. Document details.
Is the standard application a result of the MA giving themselves an
‘urgent’ authorisation?
If ‘yes, has Form 1 been received, and checked that all boxes are completed and signed.
Yes No
Yes Date ‘urgent’ authorisation given.
……………………………………….
No - then
(contact MA immediately, for
Form 1 - and also ensure Form 4 has been submitted at same time.
(Initials in these column rather than a tick)
REQUEST FOR STANDARD AUTHORISATION
DoLS Administrator :
Has Form 4 been completed?
Has the Form 4 been signed?
Has the Form 4 been dated?
Has each box been completed as appropriate?
If answer is ‘no’ to any question, revisit the form and complete.
If answer is ‘yes’ to each question, then progress.
Has there been any previous application?
If yes, then has circumstances changed since last application?
If no change in circumstances, then contact Senior Commissioner for advice on way forward.
If yes, then proceed with assessment arrangements.
Is an IMCA required?
YES NO
46
If yes, then DoLS Administrator completes Form 30 and forward to
Cloverleaf Advocacy.
Has MH/Eligibility Assessor been appointed?
Has Form 29 been completed and forwarded to MH Assessor?
Has Form 6 and Form 9 been forwarded to MH Assessor?
Has payment claim form been sent to MH Assessor? Complete part
1 and 2 only. (Complete Part 3 on return before passing to SB Panel member to sign).
Identify most appropriate BIA from BIA list.
Complete Form 28 and forward a copy/fax to BIA.
Fax Form 4 and any additional information to BIA.
Collate all documents and retain all originals in file.
Have details been entered in register?
Have details been entered on the spreadsheet (IT System when available)
BIA :
Has age assessment Form 5 been completed?
Has no refusals assessment Form 8 been completed?
Has Mental Capacity Assessment Form 7 been completed?
Has Best Interest Assessment Form 10 been completed?
Has BIA consulted with MH Assessor as appropriate?
If IMCA appointed, has Form 31 been completed?
Has Form 24 identifying RPR been completed?
Collate all forms and forward to Supervisory Body (DoLS Admin
Team)
NB If one of the assessments fails to meet the criteria, halt all other assessments, then
Has Form 10 been completed giving reasons why criteria not met?
Has all other forms completed prior to cessation of assessment been sent to the Supervisory Body?
DoLS Administrator
On receipt of Forms 6-10, 24, (and 31 if appropriate), collate and pass to Senior Commissioner Panel.
Have details been entered in register?
Have details been entered on the spreadsheet (IT System when available)
SB Authorising Panel
Are all requirements met?
If yes, complete Form 12.
47
Have conditions been considered?
Have Panel’s conditions been considered (if appropriate)?
If conditions changed or added to, has Panel contact BIA to discuss?
Has time limit been set on authorisation?
Have Panel members signed Form 12?
Has Form 25 been completed?
Has Form 32 been completed? (front sheet completed and bottom of page 2 signed and dated)
Have original Forms 12, 25 and 32 been forwarded to DoLS
Administrator?
DoLS Administrator
On receipt of Forms. Check – has RPR been identified and confirmed (signed) on Form 24?
If not, section ‘f ‘of Form 25 needs to be completed by RPR - has page 4 for RPR to complete been sent out? (Keep photocopy before sending out until original returned)
Has a RPR been identified on Form 25?
If not, has the Senior Commissioner been advised?
When confirmed, refer to RPR Provider. (Cloverleaf)
Have details been entered in the Register?
Have details been entered on the spreadsheet (IT System when available)
Has review date been entered in diary? [28 calendar days prior to expiry (and 7 calendar days for authorisation of less than 28 days)]
Have copies of assessment reports and DoL authorisation been forwarded to those identified in 12.19 and 12.20 of procedure?
For use by MCA DoLS Admin Team below this line
NOTES:
48
G
CHECKLIST FOR SUPERVISORY BODY AUTHORISATION PANEL
(REQUEST FOR EXTENSION TO URGENT DoL)
Name of relevant person: ……………………………….……………..……..…………
Name of Managing Authority: …..………………………………………………….…………
Name of person making application: …………………………….………………………….
Date application made by Managing Authority: …………………….………………………..
Date received by Supervisory Body: …………………………………………………………
REQUEST FOR EXTENSION TO URGENT DoL YES NO
Has Form 2 been received?
Has the Form been signed?
Has the form been dated?
Has each box been completed as appropriate?
If answer is ‘no’ to any question, contact the Managing Authority
If answer is ‘yes’ to each question, then progress.
Senior Commissioner to complete Form 3
MCA DoL Admin:
Has form 3 been received?
Has the form been signed?
Has the form been dated?
Has each box been completed as appropriate?
If answer is ‘no’ to any question, refer back to Senior Commissioner
If the answer is ‘yes’ to each question, then progress.
Has the MCA DoL Admin sent copy of Form 3 to Managing Authority?
Have details been entered in the DoLS Register?
Have details been entered on spreadsheet ? (IT System when available)
Have all original documents been filed in the person’s MCA DoL file?
Now refer to Standard authorisation.
For use by DoLS Admin Team below this line:
---------------------------------------------------------------------------------------------------------------------------
NOTES :
49
H
CHECKLIST FOR SUPERVISORY BODY –
AUTHORISATIONS NOT GRANTED
Name of relevant person: ……………………………….……………..……..…………
Name of Ma naging Authority: …..………………………………………………….…………
Name of person making application: …………………………….………………………….
Date application made by Managing Authority: ……………………………………..
Date received by Supervisory Body: …………………………………………………………
REQUEST FOR STANDARD AUTHORISATION NOT GRANTED YES NO
Supervisory Panel:
Has Form 13 been completed?
Has the Form 13 been signed?
Has the Form 13 been dated?
Has each box been completed as appropriate?
If answer is ‘no’ to any question, revisit the form and complete.
If answer is ‘yes’ to each question, then progress.
Has Form 13 been forwarded to DoL Administrator?
DoL Administrator
Has Form 13 been sent to appropriate parties as outlined in 13.2 and 13.3 of procedure?
Has further action been recommended?
If yes, then has action been followed up?
Have details been entered in Register?
Have details been entered on the spreadsheet (IT System when available)
Have all documents been filed in persons DoL file?
For use by DoLS Admin Team below this line:
NOTES:
50
I
CHECKLIST FOR SUPERVISORY BODY –
UNAUTHORISED DoL
Name of relevant person: ……………………………….……………..……..…………
Name of Managing Authority: …..………………………………………………….…………
Name of person who has alerted SB to possible Do L: ………………….…………………….
Date received by Supervisory Body: …………………………………………………………
UNAUTHORISED DoL YES NO
DoLS Administrator
Has a letter been received by Senior Commissions from a party other than the Managing Authority suggesting there is an unauthorised DoL.
If so, complete Form 16.
Has the Form 16 been signed?
Has the Form 16 been dated?
Has each box been completed as appropriate?
If answer is ‘no’ to any question, revisit the form and complete.
If answer is ‘yes’ to each question, then progress.
Has there been any previous application?
If yes, then has circumstances changed since last application?
If no, then contact Senior Commission for advice on way forward.
If yes, then proceed with assessment arrangements.
Have copies of Form 16 been sent out as outlined in Form 14.3 of procedure?
Has BIA been contacted to carry out an assessment?
Has the BIA completed a Form 17?
Have forms been distributed as outlined in 14.6 of procedure?
Collate all documents and retain all originals in file
Have details been entered in Register?
Have details been entered on the spreadsheet (IT System when available)?
Have forms been sent to SB Authorisation Panel?
SB Authorisation Panel
Has decision been made and Form 18 been completed?
Has form 18 been signed?
Has Form 18 been dated?
Has Form 18 been forwarded to DoLS Administrator confirming whether authorisation would be appropriate?
51
DoLS Administrator
If, decision is an unauthorised DoL in place, has DoLS Administrator commenced Standard Authorisation process?
Has Form 18 been distributed as outlined in 14.10 of procedure?
Has Managing Authority been informed that it must grant itself an urgent authorisation?
Have details been entered in Register?
Have details been entered on the spreadsheet? (IT System when available)
NB Now follow checklist for Standard Authorisation.
52
J
CHECKLIST FOR SUPERVISORY BODY
SUSPENDING AN AUTHORISATION
Name of relevant person: ……………………………….……………..……..…………
Name of Managing Authority: …..………………………………………………….…………
Name of person reporting suspension: ……………………….…….………………………….
Date of Mental Health Act detention or date of new conditions to an existing MHA Section eg., Community Treatment Order or Guar dianship: …………………………………………..
(Reasons might be where the DoLS specify residence at a particular hospital/care home and the CTO or Guardianship specifies residence at a different hospital/care home).
(Initials in these columns rather than a tick)
CHECKLIST - SUSPENDING AN AUTHORISATION YES NO
Has Form 14 been received?
Has Form 14 been signed?
Has Form 14 been dated?
Good Practice: Has a copy of Form 14 been sent to Supervisory
Authorisation Panel for information?
Have details been entered in the Register?
Have details been entered on the spreadsheet? (IT System when available)
Has Form 14 been filed in relevant person’s DoL file?
Below this line: for use by DoLS Admin Team only
---------------------------------------------------------------------------------------------------------------------------
NOTES:
53
K
CHECKLIST FOR SUPERVISORY BODY
NOTICE THAT SUSPENSION HAS BEEN LIFTED
Name of Managing Authority: …..………………………………………………….…………
Name of person making application: …………………………….………………………….
Date of Mental Health Act detention or date of new conditions to an existing MHA Section eg., Community Treatment Order or Guardianship: …………………………………………..
(Reasons might be where the DoLS specify residence at a particular hospital/care home and the CTO or Guardianship specifies residence at a different hospital/care home).
Date suspension lifted: …………………………………………………………
(NB: suspension can only be lifted within 28 calendar days, inclusive of the original Mental
Health Act detention/conditions).
NOTICE THAT SUSPENSION HAS BEEN LIFTED YES NO
Is the person no longer subject to detention under the Mental
Health Act or conflicting conditions attached to CTO or
Guardianship etc.
Is it less than 28 days from the original suspension of DoL authorisation?
If ‘yes, then progress as follows:
Has Form 15 been completed?
Has Form 15 been signed?
Has Form 15 been dated?
Has Form 15 been sent to relevant person?
Has Form 15 been sent to person’s representative?
Has Form 15 been sent to any IMCA instructed under 39D MCA?
Good Practice: Has copy of Form 15 been sent to Supervisory
Body Authorisation Panel for information?
Has original Form 15 been filed in relevant person’s DoL file?
Have details been entered in the Register?
Have details been entered onto the spreadsheet? (IT system when available)
If DoLS Admin Team have identified that 28 days have elapsed since the original suspension, the progress as follows:
Has Supervisory Body Authorisation Panel been advised?
Has Supervisory Body Authorisation Panel completed Form 23?
Has Form 23 been signed?
Has Form 23 been dated?
Has a copy Form 23 been sent to the Managing Authority?
54
Has a copy Form 23 been sent to the Relevant Person?
Has a copy Form 23 been sent to the Relevant Person’s
Representative?
Has a copy Form 23 been sent to every person named and consulted by the BIA?
Have details been entered in Register?
Have details been entered onto the spreadsheet? (IT System when available)
Has Form 23 been placed in the person’s DoLS file?
55
L
CHECKLIST FOR SUPERVISORY BODY –
NOTICE THAT A REVIEW IS TO BE CARRIED OUT
Name of relevant person: ……………………………….……………..……..…………
Name of Managing Authority: …..………………………………………………….…………
Name of person making application: …………………………….………………………….
Date application made by Managing Authority: ……………………………………..
Date received by Supervisory Body: …………………………………………………………
CHECKLIST - NOTICE THAT A REVIEW IS TO BE CARRIED
OUT
YES NO
Has a Form 19 been received?
Has Form 19 been signed?
Has Form 19 been dated?
Has Authorisation Panel been informed and completed Form 20?
Has Form 20 been signed?
Has Form 20 been dated?
Has a copy of Form 20 been sent to relevant person?
Has a copy of Form 20 been sent to person’s representative?
Has a copy of Form 20 been sent to the Managing Authority?
Have details been entered in Register?
Have details been entered on to Spreadsheet? (IT System when available)
Has Authorisation Panel completed Form 21?
Has Form 21 been signed?
Has Form 21 been dated?
Has appropriate Assessor been appointed and given copy of Form
21?
(Assessor will complete Form 5-10 as appropriate)
When received, has the form(s) been completed, signed and dated?
Has form(s) been sent to SB Authorisation Panel?
Has Form 22 been competed by SB Authorisation Panel?
Has Form 22 been signed?
Has Form 22 been dated?
Has a copy of Form 22 (and copy of review assessment forms) been sent to the Managing Authority?
Has a copy of Form 22 (and copy of review assessment forms) been sent to the Relevant Person?
56
Has a copy of Form 22 (and copy of review assessment forms) been sent to the Relevant Person ’s Representative?
Has a copy of Form 22 (and copy of review assessment forms) been sent to the any Sec 39D IMCA appointed?
Have details been entered in Register?
Have details been entered on Spreadsheet? (IT System when available)
Has Form 32 been updated?
Has original Form 22 and 32 been filed in person’s DoL file?
If authorisation is to cease:-
Has Supervisory Body Authorisation Panel completed Form 23?
Has Form 23 been signed?
Has Form 23 been dated?
Has a copy of Form 23 been sent to the Managing Authority?
Has a copy of Form 23 been sent to the Relevant Person?
Has a copy of Form 23 been sent to the Relevant Person’s
Representative?
Has a copy of Form 23 been sent to every person named and consulted by the BIA?
Have details been entered in Register?
Have details been entered on spreadsheet ? (IT System when available)
Has original Form 23 been filed in person’s DoL file?
If authorisation is to continue:-
Form 12 Standard Authorisation Form needs to be completed and process followed as outlined in F
Below this line: for use by DoLS Admin Team only
---------------------------------------------------------------------------------------------------------------------------
NOTES:
57
M
CHECKLIST FOR SUPERVISORY BODY
SELECTION, APPOINTMENT AND TERMINATION OF A
RELEVANT PERSON’S REPRESENTATIVE
Name of relevant person: ……………………………….……………..……..…………
Name of Managing Authority: …..………………………………………………….…………
Date of reason for selection, appointment or termination:
(i.e. standard authorisation application, review or other reason) …….………………………….
( CHECKLIST - SELECTION, APPOINTMENT AND TERMINATION
OF A RELEVANT PERSON’S REPRESENTATIVE
YES NO
SELECTION:
Has Form 24 been completed by BIA?
Has the person signed Form 24 to confirm willingness to be relevant person’s representative?
Has Form 24 been sent to SB Authorisation Panel?
Has Form 24 been completed?
Has Form 24 been signed?
Has Form 24 been dated?
Have details been entered in Register?
Have details been entered on spreadsheet? (IT System when available)
Has Form 24 been filed in person’s DoL File?
APPOINTMENT:
Has Form 25 been completed by the SB Authorisation Panel?
Has Form 25 been signed?
Has Form 25 been dated?
Has Form 25 been sent to the person appointed?
Has Form 25 been sent to the relevant person?
Has Form 25 been sent to the Managing Authority?
Has Form 25 been sent to any LPA or Deputy?
Has Form 25 been sent to any IMCA appointed?
Has Form 25 been sent to every interested person named and consulted by the BIA?
Have details been entered in Register?
Have details been entered on spreadsheet? (IT System when available)
Has Form 25 been filed in person’s DoL file?
58
DoLS ADMIN TEAM
PENDING TERMINATION PROCESS
From bring forward system, identify 28 days prior to expiry SB
Authorisation Panel’s need to complete Form 26.
Has Form 26 been completed?
Has Form 26 been signed?
Has Form 26 been dated?
Has a copy of Form 26 been sent to RPR?
Have details been entered in register?
Have details been entered on spreadsheet? (IT System when available)
Has Form 26 been filed in person’s DoL file?
TERMINATION PROCESS:
Has Form 27 been completed by SB Authorisation Panel?
Has Form 27 been signed?
Has Form 27 been dated?
Has a copy of Form 27 been sent to the relevant person?
Has a copy of Form 27 been sent to the Managing Authority?
Has a copy of Form 27 been sent to the LPA or Deputy?
Has a copy of Form 27 been sent to any IMCA appointed?
Has a copy of Form 27 been sent to every person named and consulted by the BIA?
Have details been entered in register?
Have details been entered on spreadsheet? (IT System when available)
Has Form 27 been filed in person’s DoL file?
Below this line: for use by DoLS Admin Team only
---------------------------------------------------------------------------------------------------------------------------
NOTES:
59
APPENDIX D
DEPRIVATION OF LIBERTY
YOUR ESSENTIAL PREPARATIONS
1. Consider whether any service user or patient in your service, who may lack capacity, ever has restrictions imposed upon them for their own best interests.
This might include:
Locked internal or external doors
Separation from other people in the building
The use or threatened use of restraint to make them do something that they are resisting, or restrict their freedom of movement, whether they are resisting or not
The use of behaviour modifying medication, including tranquilizers or anti-psychotic medication
The covert administration of medication
Verbally placating the person, or ignoring their needs
Restrictions caused by staff shortages or priorities elsewhere in the service
Restrictions caused by the use of equipment (e.g. bedsides, ‘stroke chairs’, being physically impeded by furniture)
Limits on the persons contact with friends/family o o o o
Restrictions on: o Meal options o o o
When and how to wash
Clothes to wear
Leisure activities
Access to their own money
Access to community facilities
The practicing of their own faith
Access to an independent advocate
2. Are all decisions to impose these restrictions taken (and reviewed) in a structured way, and are the reasons for making the decision recorded?
3. Is good prac tice followed in care planning and is the person’s care plan followed on an ongoing basis?
4. Has the person been assessed as to whether they lack capacity to decide whether or not to accept their care or treatment in line with the principles of the Act?
5. Co nsider whether the person’s needs be met in a less restrictive way – e.g. the minimum restriction necessary for the shortest period possible
6. Have proper steps been taken to help the person retain contact with family, friends and carers?
7. Does the person have access to an advocacy service?
60
APPENDIX E
CHECKLIST FOR THE
REVIEW AND APPROVAL OF PROCEDURAL DOCUMENT
Title Of Document Being Reviewed:
Yes/No/
Unsure
Comments
1. Title
Is the title clear and unambiguous?
Is it clear whether the document is a guideline, policy, protocol or standard?
2. Rationale
Are reasons for development of the document stated?
Yes
Yes
Yes
3. Development Process
Is the method described in brief?
Are people involved in the development identified?
Yes
No
Yes
Document to be amended in line with national and regional developments in case law
Development undertaken in consultation with members of the MCA Local
Implementation Network
Do you feel a reasonable attempt has been made to ensure relevant expertise has been used?
Is there evidence of consultation with stakeholders and users?
4. Content
Is the objective of the document clear?
Is the target population clear and unambiguous?
Are the intended outcomes described?
Are the statements clear and unambiguous?
5. Evidence Base
Is the type of evidence to support the document identified explicitly?
Are key references cited?
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Via the MCA Local
Implementation Network
See introduction
Understanding of what constitutes a DoL and the
DoLS process
Based on the Mental
Capacity Act 2005 and the supporting Code of Practice
61
Title Of Document Being Reviewed:
Are the references cited in full?
Are supporting documents referenced?
6. Approval
Does the document identify which committee/group will approve it?
If appropriate have the joint Human
Resources/staff side committee (or equivalent) approved the document?
7. Dissemination and Implementation
Is there an outline to identify how this will be done?
Does the plan include the necessary training/support to ensure compliance?
8. Document Control
Does the document identify where it will be held?
Yes/No/
Unsure
No
Yes
Yes
No
Yes
Yes
No
Comments
Not applicable
Via intranet
Summary of contact details
Document will be stored on the MCA page of the
NELCTP intranet site
9. Process to Monitor Compliance and
Effectiveness
Are there measurable standards or KPIs to support the monitoring of compliance with and effectiveness of the document?
Is there a plan to review or audit compliance with the document?
10. Review Date
Is the review date identified?
Is the frequency of review identified? If so is it acceptable?
11. Overall Responsibility for the Document
Is it clear who will be responsible for coordinating the dissemination, implementation and review of the document?
12. Document format
Has the cover sheet of the document been completed to the relevant stage of consultation/approval/ratification?
Does the document meet the template
Yes
Yes
Yes
Yes
Unsure
Yes
Yes
Standards stipulated by the
Mental Capacity Act 2005
Compliance survey undertaken Sep 10
Mental Capacity Act
Manager will be the lead officer.
62
Title Of Document Being Reviewed:
Yes/No/
Unsure
Comments document requirements of the Document
Control Policy?
Have the appendices (Checklist, Single
Equality Scheme) been completed to the satisfaction of the reader?
Committee Approval
Yes
When approved by a committee/group, this should be captured within the minutes and the
Chair of the meeting should complete this section (electronically)
Name Date
Committee Ratification
When ratified by a committee/group, this should be captured within the minutes and the
Chair of the meeting should complete this section (electronically)
Name Date
63