Supplemental material - Theoretical expectations and supportive
advertisement

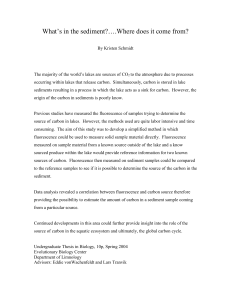
Supplemental material - Theoretical expectations and supportive observations It was the aim of the present investigation to derive information on cerebral perfusion based on two basic sources, firstly the configuration (peak intensity, duration) of the fluorescence bolus passing through arteries and parenchyma and secondly, the differences in the time-points of detection in arteries, brain tissue and veins, i.e. the delay or transit times between different compartments. To give reproducible information on cerebral perfusion, bolus configuration should therefore ideally depend on perfusion of vessels or parenchyma alone. Theoretically, however, there are numerous factors that might influence bolus configuration, peak intensity and time of appearance when the fluorescence technique is used in daily routine. Variations related to injection rate, dose and systemic hemodynamic factors: In routine use, the anesthesiologist would inject a defined volume of dissolved ICG into a central venous catheter as quickly as possible, and not into a peripheral vein, since a distal injection site would be expected to more strongly influence bolus coherence, thus reducing peak intensity and duration. A larger amount of ICG would be expected to give higher peak intensity and a more prolonged signal. In our practice, bolus size (5mg dissolved in 10 ml of water) and injection site were always the same. However, differences in injection speed, a variable that could not be completely controlled, might have induced variations in bolus configuration, since the small ICG bolus was injected manually. Hemodynamics would also be expected to influence bolus configuration and timing. Theoretically, conditions with high cardiac output might result in the bolus appearing more quickly within the brain with the bolus possibly changing its configuration. For example, in our experience, blood pressure appeared to have an influence on fluorescence transit time and intensity. For one patient with an aneurysm of the anterior communicating artery, fluorescence was recorded before and after surgery. After an (unanticipated) decrease in systolic arterial blood pressure from 140 mmHg to 80 mmHg, maximal fluorescence, rise time and time to peak nearly halved (maximal fluorescence intensity: 109.5 vs. 52.3 AI, rise time: 5.8s vs. 2.9 and time to peak: 5.3s vs. 4.9). In contrast, the derived parameter cBFI was unchanged after lowering of arterial blood pressure (cBFI: 18.3 vs. 19.3). Therefore, definition of the surrounding conditions and maintenance of blood pressure appears crucial for evaluation of ICG-fluorescence based data for some of the parameters. Factors related to illumination conditions and optical detection system: More or less light will influence the amount of detectable fluorescence and this will influence the absolute intensity of fluorescence. It is common knowledge that the intensity of fluorescence is directly proportional to the amount of excitation light. Excitation light depends on zoom, distance, angulation, and the illumination intensity of the light source. Thus, when considering the hemodynamic factors of interest in the present investigation, it can be anticipated that factors strongly dependent on maximal detectable fluorescence, such as maximal fluorescence or cBFI, will be subject to larger variations when comparing individual patients. On the other hand, hemodynamic factors depending only on time will not be susceptible to the amount of excitation light, such as “rise time”, time to peak fluorescence or transit times. Anatomical factors: One critical factor is the limitation of detectability of fluorescence to the superficial regions of the vessel because the penetration depth of near infrared light being emitted is limited. Thus, only the superficial layer of tracer (ICG) is actually visualized in larger vessels. This is the important contradistinction from techniques for perfusion measurement, such as perfusion CT or ICG NIRS.1;2 With these validated methods, basically the entire volume of the tracer is detected and can be used for determination of perfusion parameters. If the whole bolus volume could be captured with ICG angiography, there would for instance be a linear relationship between vessel size and bolus intensity. However, since only a restricted depth can be detected, maximal fluorescence will asymptotically converge toward maximally detectable fluorescence intensity with increasing vessel diameter. Fig. 1 demonstrates this relationship as measured in 25 arterial vessels of varying diameter. In addition, if the entire bolus could be imaged, the fluorescence profile of at a single point in the profile of a single, circular vessel would have to be strictly related to the diameter of the vessel, that is, fluorescence would have to follow an inverse parabolic distribution when measured across the vessel cross section. Since with larger vessels the penetration depth of fluorescence emitted by ICG is limited, this may not be the case. Fig. 2 demonstrates the theoretical and measured profile of a single large vessel (MCA) with abrogation of the expected fluorescence peak. Finally, the blood flow profile within the vessel itself may influence the time of delectability of the bolus. Under laminar flow conditions the highest velocity of blood is within the center of the vessel. Under these conditions the fluorescence bolus will therefore be detected with slight delay, because the visible outer regions of the vessel will be perfused slightly later by the fluorescence agent. This is also demonstrated in Fig. 2 as measured in a patient. In the early arterial phase only the central region of the vessel shows fluorescence. At the peak arterial phase, the entire circumference of the vessel fluoresces. This phenomenon will play a greater role in larger vessels as compared to smaller vessels. On the other hand, with turbulences, for instance after stenosis or after vessel bifurcations, the fluorophore may apparently be detectable at an earlier point of time, because turbulences result in the fluorophore distributing more readily into outer regions of the vessel. Theoretically therefore, a fluorescence bolus may be detectable more distally first and then in the nearby, more proximal, larger vessel. Artifacts The current analysis also indicated the possibility of artifacts under specific conditions. Surgical material situated in the operation field, e.g. cottons for brain protection, obscured cerebral vessels in the ICG-based angiography in some cases. Of course, these materials could quickly be identified by standard light microscopy. However, they also have a constant or a fluorescence signal resembling a sine curve due to the pulsation of the brain. In fact, this artifact shows the inverse effects of the correction algorithms of the Flow 800 software for intensity and brain pulsation on non-pulsatile fluorescing surfaces. References 1. Terborg C, Birkner T, Schack B, Weiller C, Rother J . Noninvasive monitoring of cerebral oxygenation during vasomotor reactivity tests by a new near-infrared spectroscopy device. Cerebrovasc.Dis. 2003;16(1):36-41. 2. Konstas AA, Goldmakher GV, Lee TY, Lev MH . Theoretic basis and technical implementations of CT perfusion in acute ischemic stroke, part 1: Theoretic basis. AJNR Am.J Neuroradiol. 2009;30(4):662-668.