VANDERBILT PEDIATRIC HEART TRANSPLANTATION
advertisement

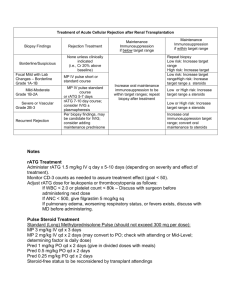
Update: 11/23/01 VANDERBILT PEDIATRIC HEART TRANSPLANTATION Rejection Protocol Mild rejection/Asymptomatic 1A No change in therapy 1B Consider Oral Pulse Steroids Moderate rejection/Asymptomatic or mild symptoms 2 No change in therapy 3A Pulse steroids; IV if early post-transplant; PO if late post-transplant Moderate/severe rejection/Hemodynamically significant 3B IV pulse steroids; Consider Thymoglobulin; Mechanical support as needed 4 IV pulse steroids; Thymoglobulin; Mechanical support as needed “Guideline” regarding interpretation of ECHO scores: It is important to know how ECHOs compare with past ECHOs for that patient and what the SF is. This program only scores points for SF <28%, most transplants run SF>35-40%. Clinical symptoms None ECHO score 0-3 ECHO score > 4 No change in surveillance. Change, possible alternative cause Very suspicious of rejection Admit, observe, repeat ECHO < 24 hrs, consider biopsy. Biopsy Repeat ECHO < 24 hours Treat for rejection Treat for rejection Optimize oral regimen whenever rejection occurs or is suspected. H2 antagonist is added for ulcer prophylaxis during steroid therapy. Biopsy should always be done prior to initiation of therapy beyond steroids, or for persistent rejection, unless clinically too unstable for biopsy at presentation. High dose IV Solumedrol (methylprednisolone) for symptomatic rejection or early moderate to severe rejection: 125 mg BID x 3-4 days (<1 yr) or 250 mg BID x 3-4 days (>1 yr to adolescent) or 1 gram qd or 500 mg BID x 3-4 days (adolescent) High dose PO Prednisone for asymptomatic, late moderate rejection (3A): infant/child: 1 mg/kg/dose PO BID, rapid daily taper to 0.8, 0.6, 0.4 mg BID then wean off over next 10 days. adolescent: 50 mg PO BID, rapid daily taper to 40, 30, 20 BID, then decrease by 1 mg/dose/day until twice daily maintenance dose of 10 mg PO BID is attained at 2weeks, wean further as indicated. Alternative PO Prednisone for asymptomatic, late (>60d) moderate rejection (3A): infant/child: 1 mg/kg/dose PO BID x 3 days, then resume prior prednisone dose. adolescent: 100 mg PO QD x 3 days, then resume prior prednisone dose. Thymoglobulin (ATG): 1.5-3.0 mg/kg/day QD for 5 days (up to 7-14 days; as short as 3 days). See separate order sheet for details.