Physical Therapy Prescription
advertisement

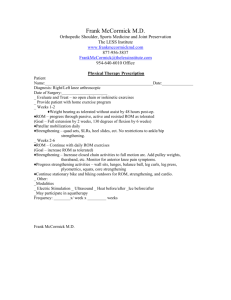
Frank McCormick M.D. Orthopedic Shoulder, Sports Medicine and Joint Preservation The LESS Institute www.frankmccormickmd.com 877-956-3837 FrankMcCormick@thelessinstitute.com 954-640-6010 Office ROTATOR CUFF REPAIR PROTOCOL Name_______________________________________________________________________________ Date__________________ Diagnosis________________________________________________________________________________________ Date of Surgery_________________________ Frequency: 1 2 3 4 times/week Duration: 1 2 3 4 5 6 Weeks ______Weeks 0-1: Patient to do Home Exercises given post-op (pendulums, elbow ROM, wrist ROM, grip strengthening) Patient to remain in splint for 4 weeks ______Weeks 1-6: Sling only! The rotator cuff tendon needs to heal back into the bone ROM goals: 140º FF/40º ER at side; ABD max 60-80º without rotation No resisted motions of shoulder until 12 weeks post-op Grip strengthening No canes/pulleys until 6 weeks post-op, because these are active-assist exercises Heat before PT, ice after PT ______Weeks 6-12: Begin PROM AAROM AROM as tolerated Goals: Same as above, but can increase as tolerated Light passive stretching at end ranges Begin scapular exercises, PRE’s for large muscle groups (pecs, lats, etx) At 8 weeks, can begin strengthening/resisted motions Isometrics with arm at side beginning at 8 weeks ______Months 3-12: Advance to full ROM as tolerated with passive stretching at end ranges Advance strengthening as tolerated: isometrics bands light weights (1-5 lbs); 8-12 reps/2-3 sets per rotator cuff, deltoid, and scapular stabilizers Only do strengthening 3x/week to avoid rotator cuff tendonitis Begin eccentrically resisted motions, plyometrics (ex. Weighted ball toss), proprioception (es. body blade) Begin sports related rehab at 4 ½ months, including advanced conditioning Return to throwing at 6 months Throw from pitcher’s mound at 9 months Collision sports at 9 months MMI is usually at 12 months post-op Comments: ____Functional Capacity Evaluation ____Work Hardening/Work Conditioning ____ Teach HEP Modalities ___Electric Stimulation ___Ultrasound ___ Iontophoresis ___Phonophoresis ____ Heat before/after ____Ice before/after ___Trigger points massage ___TENS ___ Other _____________________________ ____ Therapist’s discretion Signature__________________________________________ Date__________________