OCONEE REGIONAL HEALTH SYSTEM, INC
advertisement

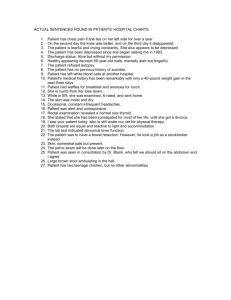
OCONEE REGIONAL HEALTH SYSTEMS, INC. POLICY AND PROCEDURE OCONEE REGIONAL MEDICAL CENTER SUBJECT: Reporting of Critical Test Results POLICY: ADM-PC-060 and Alert Values Applies To: All Clinical Departments Approved By: Chief Operating Officer Revision Date: May, 2008 Department: Administration ===================================================================== PURPOSE: To identify and establish the responsibilities of personnel reporting and receiving critical test results; to define critical tests and alert values; to list the critical tests and values for particular departments; to define the acceptable time for reporting these results to the responsible licensed caregiver; and to describe the process of reporting the Critical Tests/Values and identifying to whom they are to report. DEFINITIONS: Critical Test: means a test ordered for a patient with potentially life threatening symptoms which can narrow down a differential diagnosis and assist the physician in determining the appropriate course of action. They are reported even if within normal limits. These tests are usually ordered STAT. Alert Value: means a value at such variance with normal as to represent a pathophysiologic state that is life threatening unless some action is taken in a short period of time. Responsible Licensed Caregiver: means within the scope of their practice and in accordance with organizational policy, practice protocols or guidelines the following may receive and act on a critical result; a Nurse Practitioner (NP), Physician’s Assistant (PA), Registered Nurse (RN), Pharmacist or Licensed Respiratory Care Practitioner (RCP). POLICY: It is always preferable for the results of Critical Tests and Alert Values to be reported directly to the ordering physician. The performance of critical tests/procedures as defined by this policy is given priority over routine tests. They may or may not be designated as STAT. Critical test results (normal or abnormal), as defined by this policy, must be communicated to the responsible licensed caregiver ASAP but not more than 1 hour of being ordered. Alert Values must be communicated as soon as possible from the time they are recognized or with in 1 hour to the responsible licensed caregiver. SUBJECT: Reporting Critical Values / Results POLICY: ADM-PC-060 PROCEDURE: I. Include ordering physician’s name on every order. II. Follow department protocol to expedite the performance of the test. III. Prior to the performance of any diagnostic test, validate the correct patient by using two identifiers. IV. If the hard copy of the test result/value is not available for the responsible licensed caregiver to view, they will write down the results and read it back to the technologist or technician. V. The technician will document the notification including the time, date, and who communicated and received the critical value/result in the medical record.** ** Exception - Physician to physician communication. A record of this communication will be done via dictation. VI. CARDIOPULMONARY CRITICAL TESTs (as defined by this policy) A. B. C. D. VII. ABG’S EKG’s ECHO Ultrasound CARDIOPULMONARY ALERT VALUES A. ABGs CRITICAL ABG INDICATORS UNITS LOW LIMIT HIGH LIMIT PaCO2 mmHg 21 66 Ph - 7.21 7.59 PaO2 mmHg 45 - B. EKGs 1. 2. 3. 4. 5. PVCs >3 in a row Blocks Tachycardia >120bpm Bradycardia <40bpm Supraventricular Tachycardia Page 2 of 7 SUBJECT: Reporting Critical Values / Results POLICY: ADM-PC-060 6. Ventricular Tachycardia 7. Acute changes ST elevation or automated interpretation of EKG as Acute MI C. PULMONARY FUNCTION ALERT VALUES 1. FeV1 < 1.0L 2. Bronchial Provocation: ≥20% decrease in FeV1 D. CARDIAC ULTRASOUND ALERT VALUES 1. 2. 3. 4. Pericardial effusion with associated RV collapse Ejection fraction (EF) <20% or change in EF Acute Valvular Insufficiency Severe Aortic Stenosis or Mitral Stenosis PROCEDURE: A. Communicate results to the physician, primary nurse, or respiratory therapist. B. Abnormal EKGs or ABG results must be communicated within 15 minutes after results are known. ** Note: Dr. Wesley King requests all ABG’s ordered by him be called directly to him, even if results are within normal limits. C. Attach a comment in the LIS (Laboratory Information System) or progress notes that indicates to whom the critical limit results were communicated, noting “R&V” after having the party repeat and verify the results. VIII. RADIOLOGY A. CRITICAL TESTS (as defined by this policy) 1. 2. 3. 4. 5. B. Chest X-ray Ultrasound (abdomen/pelvis or testicular) Head CT Chest CT CT (abdomen and/or pelvis) CRITICAL ALERTS 1. 2. 3. 4. 5. 6. 7. 8. 9. Aortic Dissection Bowel Perforation with Free Air Esophageal or Bronchial Obstruction CVA, Brain or Spinal Cord Mass or Bleed Ectopic Pregnancy Leaking Aortic Aneurysm Life Threatening Misplaced Tube or Line Ovarian/Testicular Torsion Pulmonary Embolism Page 3 of 7 SUBJECT: Reporting Critical Values / Results POLICY: ADM-PC-060 10. Significant Solid Organ Laceration 11. Spinal Cord Compression or Injury 12. Tension Pneumothorax 13. Cardiac tamponade 14. Pericardial effusion with or without cardiac tamponade 15. Acute congestive heart failure 16. Myocardial rupture IX. LABORATORY ALERT VALUES A. HEMATOLOGY 1. 2. 3. 4. 5. 6. 7. 8. WBC <1,000/mm3 Platelets <30,000/mm3 Hemoglobin <6 mg/dl Hematocrit <15 INR Partial Thromboplastin (PTT) Heparin PTT < 66 Manual Diff instance only 9. Malaria smear B. >35,000/mm3, First instance only >1000,000/mm3, First instance only >20 mg/dl >60 >4.1 >95 >120 Blasts or Malignant cells, first Positive CHEMISTRY AND DRUG LEVELS: 1. Glucose 2. Sodium 3. Potassium 4. CO2 5. Calcium 6. Magnesium 7. Phosphorus 8. Ammonia 9. Bilirubin 10. TSH 11. CKMB 12. Troponin 13. SGOT 14. SGPT 15. BUN 16. Creatinine 17. Acetaminophen 18. Digoxin 19. Ethanol 20. Gentamicin 21. Phenobarbital <40 mg/dl <120 mEq/L <2.5 mEq/L >400 mg/dl >160 mEq/L >6.5 mEq/L <15 mEq/L <7.0 mg/dl >13.0 mg/dl <1.0 mg/dl >5.0 mg/dl <1.0 mg/dl >9.0 mg/dl >100 First instance only > 15 >50 First instance only Elevated, First instance only Elevated, First instance only >500 First instance only >500 First instance only >100 First instance only >5 First instance only >50 First instance only or higher than previous >2.5 ng/ml >400 First instance only P>10.0 mcg/ml- CALL TO PHARMACY T>2.5mcg/ml - CALL TO PHARMACY >40 mcg/ml Page 4 of 7 SUBJECT: Reporting Critical Values / Results 22. Phenytoin 23. Procainamide & NAPA 24. Quinidine 25. Salicylate 26. Tegretol (Carbamazepin) 27. Theophylline 28. Valproic Acid 29. Vancomycin 30. HIV-1 antibody screen C. RPR Rotavirus RSV AFB culture and smear 5. Blood cultures 6. C. Diff 7. Cryptococcus antigen 8. CSF & Body Fluid Smear & Stains 9. Hemophilus influenza antigen 10. Neisseria Meningitidis Antigen 11. Stool Cultures 12. OR Gram stains 13. Surveillance swabs 14. Wound Cultures Reactive Positive Positive Positive, First instance only, complete notification when ID is received from reference lab. Positive, first instance only unless subsequent stains are different from original* Positive, First instance only Positive Malignant cells or Blasts, Positive gram stains or fungus, positive India Ink preparations Positive Positive Positive for Salmonella, Shigella, Yersenia, Campylobacter, Vibrio, E Coli 0157** Positive Positive for VRE, MRSA, VRSA Positive for clostridium BLOOD BANK 1. Cross match 2. Antibody Screens 3. Antibody screen during pregnancy E. >30 mcg/ml >30 mcg/ml >5 mcg/ml >30 mg/L >15 mg/dl >20 mcg/ml >100mcg/ml P >26 mcg/ml- CALL TO PHARMACY T>10 mcg/ml- CALL TO PHARMACY Reactive MICROBIOLOGY 1. 2. 3. 4. D. POLICY: ADM-PC-060 No match, Incompatible prior to surgery or significant delay in testing Reactive Positive (one causing HDN) PROCEDURE: ALERT VALUES will be called directly to the responsible licensed caregiver within 1 hour. For more specific instructions: see Laboratory Policy LAB-GEN-1007: Alert Values. Page 5 of 7 SUBJECT: Reporting Critical Values / Results POLICY: ADM-PC-060 F. DOCUMENTATION: Documentation of when, to whom and “read back and verified” must be entered into the medical record. The information may be entered via the Laboratory computer system or noted in the Progress Notes or Nurse’s notes as applicable. G. PERFORMANCE MONITORING: 1. A review of 50% of all critical tests WITH CRITICAL RESULTS will be done by the Patient Safety Committee or their designee. The threshold is 97% of critical tests were completed and the results reported to the responsible licensed caregiver with in 1 hour. 2. A review of 100% of all laboratory alert value turn around times will be done by Lab. The threshold is 97% of alert values are reported with in 1 hour to the responsible licensed caregiver. REVIEW RESPONSIBILITIES: Patient Safety Committee FORMS: None REFERENCES: JCAHO 2005 National Patient Safety Goal 2b LAB-GEN-1007: Alert Values LAB-GEN-1012: Reporting of Amended Results * LAB-MC-462: Positive Blood Culture Physician Notification ** LAB-MC-490: Rapid Identification of E. Coli ORMC Cardiopulmonary policy # 01-23-03 ORMC Radiology policy # RAD 8 b “Reporting Critical Results” Reporting of Amended Results - Consult LAB policy LAB-GEN-1012: Reporting of Amended Results. Medical Laboratory Observer Clinical Laboratory Reference, Table of Critical Limits APPROVAL SIGNATURES: _____________________________________ ___________________________________ Chair - Patient Safety Committee Chief Operating Officer _____________________________________ ___________________________________ Chief of Staff Policy and Procedure Committee Page 6 of 7 SUBJECT: Reporting Critical Values / Results Date of Origin: December 2003 Revision Date: May 9, 2008 Page 7 of 7 POLICY: ADM-PC-060