pilot ethnic minority testing project 12.13
advertisement

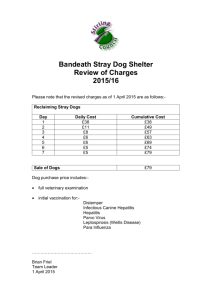
Project Initiation Document Project Name Hepatitis (B and C) Awareness and Testing in Minority Ethnic Populations (HATMEP) Sponsor Lothian Viral Hepatitis Managed Care Network Project Leads Mina O’Hara, Lindsay Bowden, Karen Matthews, in conjunction with MEHIS Start Date January 2013 Completion Date March 2015 Aims To work with minority ethnic groups in Lothian representing high/intermediate prevalence countries (for viral hepatitis) to educate, inform and raise awareness about hepatitis B and C, including awareness about prevention and prevention of onward transmission. To offer testing following education sessions to those over 16 years1, for hepatitis B and C, and HIV if appropriate. Collaborate with GPs to raise awareness about potential need for testing in these populations. Offer referral to secondary care to those with a positive result. Explore feasibility of offering a regular community-based outreach testing clinic in conjunction with MEHIS Gather together a stock of resources in translation including audio visual Objectives Eastern/Central European communities Procure or produce materials in Polish encouraging Polish people to get tested for Hepatitis B (and at the same time Hep C) and to use existing services e.g. GPs and other testing clinics. 1 Work with Polish community outlets e.g. shops, churches, clubs, consulate to promote materials, and raise awareness. Work with Harm Reduction Team regarding materials in Polish relating to injection of performance and image enhancing drugs. People under 16 years of age will be signposted to their GP if appropriate 1 Work with GPs to discuss why Polish people may be requesting testing for hepatitis B. Investigate how we can reach the Romanian, Slovenian and Lithuanian populations, especially the Romanians whose numbers are expected to increase in Lothian in the near future. Build links with groups or institutions where Romanians congregate (e.g. Romanian Consulate, Orthodox Church in Meadow Place, Streetwork and Homeless organisations, and the car boot sale in the Omni) and consider offering testing clinics as a way of raising the profile of Hepatitis C testing. Advise that those placing themselves at risk when abroad can seek hepatitis B immunisation at a private travel clinic or GP. Immunisation for travel purposes will most likely incur a fee in general practice. South Asian communities Make available materials in Urdu, Punjabi, Bengali encouraging people from South Asia to get tested for hepatitis B and C and to use existing services e.g. GPs and other testing clinics. Continue to make links with community/faith groups to raise awareness, offer on-site testing for hepatitis B and C, and refer all with a positive result on to secondary care services. Work with GPs to discuss why people from South Asia may be requesting testing for hepatitis B and C. Advise that those placing themselves at risk when abroad can seek hepatitis B immunisation at a private travel clinic or GP. Immunisation for travel purposes will most likely incur a fee in general practice. Advise those identified as positive who have children to seek testing for children at RHSC and hepatitis B immunisation for household contacts at GP Chinese communities Make available materials in Chinese languages encouraging people from China to get tested for hepatitis B and to use existing services e.g. GPs and other testing clinics. Work with MEHIP to refresh the 2002 Chinese Hepatitis B Education Project; this time offering on-site testing at the same time. Refer all with a positive result on to secondary care services. 2 Work with GPs to discuss why people from China may be requesting testing for hepatitis B. Advise that those placing themselves at risk when abroad can seek hepatitis B immunisation at a private travel clinic or GP. Immunisation for travel purposes will most likely incur a fee in general practice. Advise those identified as positive who have children to seek testing for children at RHSC and hepatitis B immunisation for household contacts at GP African communities In the longer term it is hoped that joint work can be carried out with African communities in conjunction with Waverley Care. Deliverables Information for communities in translation Operational policy describing service delivery and follow-up Information and awareness raising sessions, developed with community/faith groups On-site testing sessions Materials for general practice e.g. local AIDS sheets Rationale and policy guidance People born or brought up in a country with an intermediate or high prevalence (2% or greater) of chronic hepatitis B are at increased risk of hepatitis B compared with the general UK population. This includes all countries in Africa, Asia, the Caribbean, Central and South America, Eastern and Southern Europe, the Middle East and the Pacific islands. The HPA migrant health site suggests screening all Polish people for hepatitis B and only to screen for hepatitis C if other risk factors apply (injecting drug use is biggest risk in Poland). The same advice applies to Latvia, Bulgaria and Estonia. The HPA migrant health site says that for Romania, Slovenia, Lithuania have an intermediate prevalence of hepatitis B and consideration should be given to screening for hepatitis B, particularly among those who have recently arrived. These countries also have a considerably higher prevalence of hepatitis C than the UK and consideration should be given to screening for hepatitis C. SIGN Guideline 92 on the Management of hepatitis C advises testing for “people who have received medical or dental treatment in countries where HCV is common and infection control may be poor”. 3 The Scottish Government’s Sexual Health and Blood Borne Virus Framework (2011-15) sets out the following actions in relation to viral hepatitis and minority ethnic populations: Under outcome 3 (People affected by BBVs lead longer, healthier lives): ‘awareness raising and other initiatives among migrant populations to encourage test uptake among people who have come from areas of high prevalence for hepatitis C such as Pakistan and other South Asian countries.’ And Under outcome 2 (A reduction in the health inequalities gap in sexual health and BBVs) ‘multi-agency partners should work together to ensure that prevention, treatment and care pathways for hepatitis B consider the language, literacy and/or cultural challenges to risk populations accessing these services in Scotland to optimise their uptake.’ NICE guidance ‘Hepatitis B and C: ways to promote and offer testing to people at increased risk of infection’ (2012) recommends that local community services serving migrant populations work in partnership with primary care practitioners to provide testing of adults and children at increased risk of infection. This should include raising awareness of hepatitis B and C, promoting the availability of primary care testing facilities and providing support to access these services. However, the UK National Screening Committee published a position statement in March 2011 saying that screening for Hepatitis B and Hepatitis C amongst ethnic minorities born outside the UK was not recommended, but that the position would be reviewed in 2014. A number of research questions were identified that would help to inform a decision on screening for Hep B and C. Prevalence Eastern/Central European populations Since 2004, when the EU opened up to Eastern European countries, there has been an increased number of migrants from EU8 countries (primarily Poland but also Czech Republic, Slovakia, Hungary and to a lesser extent Lithuania, Latvia and Estonia) coming into Scotland. Scotland will have new migrant groups from Bulgaria and Romania arriving in larger numbers from later this year when restrictions on entry are lifted. 4 The prevalence of hepatitis C in these countries is estimated to be 1.90% in Poland, 0.75% in the Czech Republic, 1.50% in Slovakia, and 3.5% in Romania. This compares with 0.9% prevalence in Scotland. The prevalence of hepatitis B (surface antigen) is between 2% and 7% in all of Eastern Europe except Slovakia (ECDC: Hepatitis B and C in the European neighbourhood 2010) and it would be expected that similar proportions of migrant communities in Scotland would be affected by these viruses. South Asian populations The estimated prevalence of hepatitis C in South Asian populations living in Glasgow is 4.1% (South Asian Study and HCV test database). Chinese populations The Chinese Hepatitis B Education Project, started in Lothian in 2002, established that 10% of Edinburgh’s Chinese population were chronically infected with hepatitis B. Previous/ongoing activity in Lothian Chinese communities (Edinburgh) Chinese Hepatitis B Education Project (started 2002), Liver Unit, Royal Infirmary Awareness raising and testing with Chinese community/faith groups (restarting March 2013) South Asian communities Awareness raising and testing with South Asian community/faith groups (started 2010) e.g. Pakistan Society, NKS, mosques in Edinburgh. Eastern/Central European communities Hepatitis C Trust: Awareness raising in preparation for one testing day in Hepatitis C Trust Van offered September 2012. with Svetlika, Fort Community Centre. MELA Hepatitis C Trust stall/ testing van at MELA in Sept 2012, and stall only in Sept 2010 Materials currently available in Lothian English BBV testing leaflet (NHS Lothian) Take Control (for new hepatitis C diagnoses) NHS Health Scotland, 2011 Hepatitis B: pioneering liver health (British Liver Trust) Polish Awareness raising leaflet (Hepatitis C Trust) 5 Take Control (for new hepatitis C diagnoses) NHS Health Scotland, 2011 Urdu Hepatitis C: The more you know the better (NHS England, Hepatitis C Trust, 2009) Chinese languages Knowing about Hepatitis B (NHS Lothian, MEHIP 2005) Hepatitis B in Cantonese (British Liver Trust) All available from Lothian Viral Hepatitis Managed Care Network, Laura Weddell Tel 0131 465 5450 Hepatitis Scotland and Glasgow and Greater Clyde Health Board are working to develop patient information in translation for new diagnoses of hepatitis B and C, for all health boards to use. Costs Of purchasing leaflets in translation. BBV nurse specialist time to develop relationships with community/faith groups in order to jointly work up awareness-raising sessions and on-site testing. Assumptions That the interpreting services LITS can support this work That the relevant link workers at MEHIS act as ‘enablers’ between community /faith groups and the BBV nurse specialists. Risks That people testing positive cannot be contacted for follow-up That people testing positive do not attend for follow up. Stakeholders Minority Ethnic Health Inclusion Service (NHS) LMC (GP sub-committee) Hepatitis C Trust Minority Ethnic community groups/faith organisations BBV clinical nurse specialists C Plus Annette Wilson, Waverley Care Jessie Anderson, Access Practice 6 Viral Hepatitis Managed Care Network Testing and Referral Action Group Christine Evans, NHS Lothian Executive Lead for Viral Hepatitis Project control and reporting Planning meetings with stakeholders will be organised by the project leads/MCN. Project outcomes will report in to the MCN Testing and Referral Action Group. Hilda Stiven Lothian Hepatitis MCN Co-ordinator 16/02/2016 7