Travel Questionnaire
advertisement

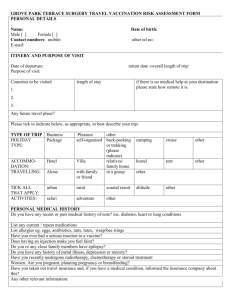
The Alexandra Practice 365 Wilbraham Road Whalley Range Manchester M16 8NG Travel Clinic Questionnaire – Registered Patient Please note that we will not issue travel vaccinations to patients who are travelling within 7 days of this request. Name Address Date of birth Postcode Telephone number Male / Female Trip details Date of departure Trip duration Countries to be visited Date of return Medical history Do you have any current or past medical history of note? (inc. diabetes, heart, lung conditions)? Do you or any close family members have epilepsy? Do you have any history of depression, anxiety or mental illness? Are you taking any medication currently? Please list Do you have any allergies? For example eggs, antibiotics, nuts? Have you ever had a serious reaction to a vaccine? Women only: are you pregnant, planning pregnancy or breastfeeding? Do you have any allergies? For example eggs, antibiotics, nuts? Have you taken out travel insurance? If you have a medical condition, have you informed your travel insurance company? The Alexandra Practice 365 Wilbraham Road Whalley Range Manchester M16 8NG Vaccination history: Have you ever had any of the following vaccinations? If so, please give date Tetanus Polio Typhoid Hepatitis A Meningitis Yellow Fever Rabies Jap B Encephalitis Have you ever taken Malaria tablets? If so, which and when Diphtheria Hepatitis B Influenza Tick Borne To be completed with the nurse: I have no reason to think that I might be pregnant. I have received information on the risks and benefits of the vaccines recommended and have had the opportunity to ask questions. I consent to the vaccines being given. Signed ____________________________ Date ____________________________ For official use only Patient name _______________________ Travel risk assessment performed Travel vaccines recommended for this trip Yes Hepatitis A Hepatitis B Typhoid Cholera Tetanus Diphtheria Polio Meningitis ACWY Yellow Fever Rabies Jap B Encephalitis Other Travel advice given Food, water and personal hygiene Insect bite prevention Insurance Yes / No No Travellers diarrhoea Hep B & HIV Animal bites Air travel Accidents Sun / heat protection Malaria prevention advice and prophylaxis Specify medication Further information e.g. weight of child Staff signature _______________________ Position __________________ Date __________