Full Article
advertisement

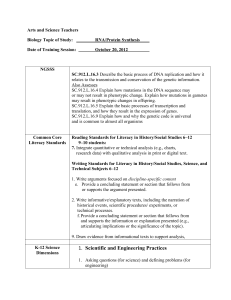
Phenotypic and Genotypic Assays for HIV-1 Drug Resistance Oct., 1999 Genotypic and Phenotypic Assays for HIV-1 Drug Resistance I. Introduction: The virus population in an HIV-1 infected individual has quasispecies nature just like any other RNA viruses. So-called quasispecies refers to the existence of genetically distinct viral variants that evolve from the initial virus inoculum. For retroviruses, such as HIV-1, this is mainly due to its reverse transcriptase does not have the DNA proofreading mechanisms and the rapid viral turnover yyy Eigen, 1993 Sci. Am:269, 4249; Drake, PNAS, 1993 90: 4171-4175; Mansky, 1995 JV, 69:5087-5094 kkk. The size of HIV-1 genome is about 104 nucleotides, the error rate of reverse transcriptase is about 1/105 nucleotides and it is estimated that there are 109 viral particles produced per day and the rounds of replication is about 107, therefore, about 3300 newly produced viruses will carry a particular mutation each day yyy Coffin, 1995, Science Vol. 267: 483-489; Kuritzkes, 1999 HIV Clinical Management, Vol.13 kkk. Although the usage of combination therapy of potent antiretroviral drugs in HIV1 infected individuals has produced significantly reductions of HIV-1 RNA in plasma to below detectable levels and resulted in dramatic decrease in disease progression and mortality in the developed world yyy Palella, 1998 NEJM 338:853-860 kkk there is increasing evidence demonstrated the failure of such potent combination therapy. Numerous factors could contribute to the failure of antiretroviral therapy including limited potency of the regimen, poor adherence, pharmacological factors, limited penetration of drug into sanctuary sites, and progressive immunologic decline, but drugresistance variants may be the results of all of above and most likely to be responsible for the failure of combination therapy yyy Hirsch, 1998, JAMA vol. 279: 1984-1991; Kuritzkes, 1999 HIV Clinical Management, Vol.13 kkk. When antiviral drug selective pressure is applied to viral quasispecies in an infected person, preexisting minor viral species resistant to that drug rapidly become predominant and are selected as the most fit species in the presence of drug. In addition, persistent viral replication permits further viral evolution leading to high-level drug resistance by cumulative mutation acquisition 1 Phenotypic and Genotypic Assays for HIV-1 Drug Resistance Oct., 1999 yyy Coffin, 1995, Science Vol. 267: 483-489; Hirsch, 1998, JAMA vol. 279: 1984-1991 kkk. Resistance to antiretroviral drugs is determined by mutations in the genetic regions that encode the protease (PR) and reverse transcriptase (RT). There are two types of mutations: primary and secondary mutations. Primary mutations alter the binding sites of drug to its target and result in an increase in the amount of drug necessary to inhibit the function of enzymes. Secondary mutations increase the level of resistance by improving the fitness of viruses carrying primary mutations, such mutations have little or no effect to resistance in the absence of the primary mutations yyy Kuritzkes, 1999 HIV Clinical Management, Vol.13 kkk. There are also two types of resistance: 1. Genotypic resistance: a prediction of resistance based on the virus gene sequences and a database containing the phenotypic resistance information for virus gene sequences. 2. Phenotypic resistance: an increase in the concentration of drug required inhibiting a virus relative to a drug sensitive reference virus. yyy Dutko (you wrote this in the outline) kkk II. Why is it important to measure drug resistance? Currently, there are very few laboratory tools that clinician could use to guide the selection of antiretroviral therapy in treatment-experienced patients with virologic failure. Although treatment history and presumed patterns of cross-resistance provide some guideposts for making rational treatment decisions, history alone may be a poor indicator of the extent of resistance in the virus population in an infected individual. Drug resistance testing of HIV-1 could be a valuable tool in patient management in such circumstances. As mentioned above, the quasispecies nature of HIV-1 plays a very important role in the emerging of drug resistance virions. It is likely that the success of combination drug therapy (such as HAART) has been determined even before it starts. Performing drug resistance tests up-front may provide the most valuable information to maximize the effect of any combination therapy yyy Perrin, 1998 Science Vol. 280:1871-1873 kkk. Therefore, the significance of drug resistance tests including the choice of initial treatment regimen, explaining and managing 2 Phenotypic and Genotypic Assays for HIV-1 Drug Resistance Oct., 1999 treatment failure, tracking the prevalence of drug resistance in HIV-1 primary infection, and guiding the choice of salvage therapy in the treatment failure patients yyy Kuritzkes, 1999 HIV Clinical Management, Vol.13 kkk. Recent advances in drug susceptibility testing and preliminary data from pilot studies provide encouraging results that may speed the implementation of these assays yyy Durant, 1999 The Lancet Vol. 353: 2195-2199; Saag, 1999 39th ICAAC kkk. III. How is resistance measured? 1. Genotypic assays for drug resistance: to sequence the HIV-1 protease and reverse transcriptase genes and to predict the potential drug resistance based on the deduced amino acid sequences of these proteins. Such assays are depend on the amplification of the interested genes from HIV-1 RNA in plasma and previously demonstrated data to formulate any prediction. 2. Phenotypic assays for drug resistance: to test the susceptibility of HIV-1 to inhibition by a particular drug. Drug susceptibility is defined by determining the amount of drug required to inhibit virus production in vitro by 50% (IC50), 90% (IC90), or 95% (IC95), most commonly used is IC50. Figure 1 shows a drug susceptibility profile difference between drug sensitive and resistance patients (adapted from brochure of PhenoSense, ViroLogic Inc.). 3. Concordance and discordance between Figure 1 genotypic and phenotypic assays. Concordance results are the ones that genotypic and phenotypic testings are in agreement. This is heavily depending on the depth of our knowledge on how the protease and reverse transcriptase works and all the potential interactions in the 3 Phenotypic and Genotypic Assays for HIV-1 Drug Resistance Oct., 1999 enzyme coding regions. Discordance is the phenotypic testing results are different from the predicated results obtained from genotypic testing. Such discordance is mainly caused by the lack of understanding of all possible mutational interactions (primary and secondary mutations, known and unknown mutations). For example, some naturally occurring codons within the PR or RT genes may modulate the enzyme functions (phenotype) when known drug resistance mutations present on these genes and produce drug sensitive virions and vise versa. 4. Advantages and disadvantages of genotypic and phenotypic assays. As shown in figure 2 (modified from Kuritzkes, 1999 HIV Clinical Management, Vol.13), both tests have advantages and disadvantages when come to clinical utilities. Figure 2 IV. Companies involved in phenotying and genotyping. 1. ViroLogic Inc. PhenoSenseTM HIV. This assay basically performing a phenotypic assay based on the genetic information that obtained from patient plasma samples. Almost a combination between genotypic and phenotypic tests, PhenoSenseTM HIV amplifies 4 Phenotypic and Genotypic Assays for HIV-1 Drug Resistance Oct., 1999 the nucleic acid from patient plasma first and then incorporates the patient-derived segment into a resistance test vector that has an indicator gene (Luciferase). Such vectors are then introduced into host cells through transfection, and virus particles are collected from the transfected cells and used for infecting target cells. Drug susceptibility is measured by comparing luciferase activity produced in the presence and absence of antiviral drugs. PhenoSenseTM HIV needs about 14 days to get results which is longer than genotypic test (usually a few days) and shorter than phenotypic test (usually 4to 6 weeks). The assay can readily perform on patients with viral load as low as 500 copies per ml. It was estimated that over 90% of successful rate if the patient’s viral load is 500 to 1000 copies per ml. Minority resistance species can also be detected if it is over 10% to 40% of total viral population yyy ViroLogic Brochure on PhenoSenseTM HIV kkk. The latest results have shown that this assay can provide consistent and reproducible results when assessed twice over a median of 30 days in patients on stable antiretroviral therapy yyy Haubrich, Abstract 417, 39th ICAAC, 1999 kkk. Another study headed by Dr. Saag of University of Alabama at Birmingham using this assay showed that the test more accurately predicated resistance to antiretroviral drugs than the patient’s previous track record of treatment yyy Saag, 1999 39th ICAAC kkk. 2. Virco/Laboratory Corporation of America Genotypic assay: VircoGENTM. Nucleic acid sequence based assay and its software is connected to the VIRCO’s database to quickly identify the potential phenotypes of drug resistance. The preliminary data showed that patients had sensitive viruses determined by this assay were four times likely to respond to drug. The turn-around time is about five to ten working days therapy yyy LabCorp/VIRCO News Releases June, 1998 kkk. Phenotypic assay: AntivirogramTM. In vitro cell culture based assay the turn-around time is about three to four weeks yyy LabCorp/VIRCO News Releases June, 1998 kkk. 3. Visible Genetics 5 Phenotypic and Genotypic Assays for HIV-1 Drug Resistance Genotypic assay: TruGeneTM. Oct., 1999 Nucleic acid amplification and sequence analysis based assay in combination with Roche Amplicor extraction methods. The only genotypic test that can analyze viral load as low as 200 copies per ml or less and still provide useful information. The latest results showed that TruGeneTM testing has a significant benefit on the virological response when choosing a therapeutic alternative yyy Visible Genetics Inc., News releases, June, 1999; Durant the Lancet, 1999 Vol. 353:2195-2199 kkk. 4. Specialty Laboratories Genotypic assay: HIV-1 GenotypRTM Plus. Nucleic acid amplification (PCR) and sequencing analysis based assay. The turn-around time is about 7-9 days. Phenotypic assay: a probe based technology to detect drug resistance phenotypically. The turn-around time is about four weeks and cost ($600 per sample) less than other phenotypic tests (average $1000 per sample) yyy Specialty Laboratories Brochure, 1999 kkk. V. Comparison among different assays: 1. Genotypic assays: VircoGENTM,. TruGeneTM, and GenotypRTM Plus: All three assays cost about the same, around $500 per sample and the turn-around time is about five to ten days. TruGeneTM is the most sensitive assay (can go below 200 copies per ml) and VircoGENTM has direct access to an extensive database for data interpretation. GenotypRTM Plus takes about 7 to 9 days that may save a day or two compare to the other two assays. 2. Phenotypic assays: PhenoSenseTM HIV,. AntivirogramTM, and Phenotypic assay by Specialty Labs.: PhenoSenseTM HIV is the fastest one (turn-around time 14 days or less compares to four to six weeks) and has been demonstrated to be able to provide very predicative results for selection of drug therapy. AntivirogramTM is produced by same manufacturer as genotypic assay VircoGENTM and both tests results could be done by one shipment of samples and obtain complementary results from one source. The phenotypic assay offered by Specialty Labs. is the most cost-effective one among these three assays, $600 per sample compares to $1000 per sample. 6 Phenotypic and Genotypic Assays for HIV-1 Drug Resistance Oct., 1999 3. Genotypic vs. phenotypic assays: Genotypic assays are less expensive, take less time and easier to perform, and offer results faster. But such assays need expert interpretation of the results and it still is difficult to predict the consequences of mutational interactions on the phenotype. Although it takes longer and more difficult and expensive to run a phenotypic test, phenotypic assays can provide susceptibility data even the genetic basis of a particular resistance has not been identified or understood. Importantly, phenotypic assay measures the net effect of the sum of different mutations and crossresistance even some of the interactions are poorly understood. 7 Phenotypic and Genotypic Assays for HIV-1 Drug Resistance VI. Oct., 1999 Drug resistance categories There are three types of drug resistance: to PIs (protease inhibitors), to NNRTIs (non-nucleoside reverse transcriptase inhibitors), and to NRTIs (nucleoside reverse transcriptase inhibitors). Figure 3 shows the key codons for all three types of drug resistance. Figure 3 Figure 3 Shows the most common HIV-1 mutations selected by PIs (A), NRTIs (B), and NNRTIs (C). For each amino acid residue listed, the letter above the listing indicates the wild type (drug sensitive) amino acid in that position and the italicized letter below the residue indicates the substitution that confers drug resistance. The black bars represent drug selected primary mutations, the white bars represent drug selected secondary mutations, and the blackand-white bar indicates a mutation selected in vitro, but rarely seen in specimens from patients in whom therapy fails. 1. Key codons for resistance to protease inhibitors (PIs) Indinavir (Crixivan): M46I, L; V82A,F,T (sensitive position resistance) Ritonavir: V82A,F,T Saquinavir: G48V Nelfinavir: D30N Amprenavir: I50V Besides the drug resistance to individual ptotease inhibitor, there are many studies showed that cross-resistance among PIs present another big challenge for antiretroviral therapy drug selection and patient management yyy Condra, 1995 Nature Vol374:569-571; Condra, 1998 Drug Resistance Updates; Palmer, 1999 AIDS, Vol 13:661-667 kkk. As high as 77-95% of patient plasma-derived recombinant HIV-1 isolates showed broad crossresistance among different protease inhibitors has been reported yyy Hertogs, Abstract 42195, 12th World AIDS Conference, Geneva, 1998 kkk 2. Key codons for resistance to NRTIs Zidovudine: K70R; T215Y Didanosine: L74V Zalcitabine: L74V; T69D 8 Phenotypic and Genotypic Assays for HIV-1 Drug Resistance Oct., 1999 Lamivudine: M184V Stavudine: V75T Abacavir: M184V Multinucleoside resistance: Q151M; A62V; V75I; F77L; F116Y 3. Key codons for resistance to NNRTIs (key resistance codons) Navirapine: K103N; V106A; V108I; V181C,I; Y188C; G190A Delavirdine: K103N; Y181C,I Efavirenz: K103N VI. Clinical results There are several studies have been published using drug resistance testing. Some of the studies were retrospective and some of them were prospective. The following are two examples: 1. VIRADAPT: a prospective randomized study comparing genotype-guided therapeutic decision-making vs. standard of care in 108 patients on a stable failing antiretroviral regimen. In this study, TruGeneTM by Visible Genetics Inc. was used as the drug resistance test. As shown in Figure 4 the use of drug resistance test could be beneficial as measured by viral loads in plasma from both control and genotypeguided patients yyy Durant, et al., Lancet, vol.353, No. 9171: 2195, 1999; Garraffo, et al., Abstract 1166, 39th ICAAC, 1999; Chaix, et al., Abstract 466, 39th ICAAC, 1999 kkk. The VIRADAPT Trial: HIV-1 RNA Mean Change From BL at 3 and 6 Months The VIRADAPT Trial: Patients With Undetectable HIV-1 RNA at 3 and 6 Months Genotypic Group Control Group 35 Control Group Genotypic Group 0 30 –0.20 25 –0.40 Plasma HIV-1 RNA (log10 ) % Patients With HIV-1 RNA <200 Copies/mL –0.60 –0.80 20 15 10 –1.00 5 –1.20 0 0 –1.40 0 3 Time, months 6 3 6 Time, months Durant et al. Lancet. 1999;353:2198. Durant et al. Lancet. 1999;353:2197. 9 Phenotypic and Genotypic Assays for HIV-1 Drug Resistance Oct., 1999 Figure 4 2. GART study (Genotypic Antitretroviral Resistance testing): a multicenter, randomized pilot study to determine the short-term effects of genotypic analysis in management of patients failing antiretroviral therapy. ABI sequencing instrument was used to perform the genotypic analysis. Total 153 patients were enrolled and divided to two groups, one GART, the other one no-GART. With expert interpretation, GART group was superior to no-GART as measured by short-term viral load response (-1.14 log vs. –0.65 log) yyy Baxter, 1999 Antiviral Therapy Vol.4: 43 kkk. VII. Conclusions The latest promising results by several groups (Saag, Durant, and Baxter) showed that either genotypic or phenotypic drug resistance tests are feasible and could be very beneficial in guiding the choice of treatment regimen in patients failing current therapy if they were done correctly. However, there are a number of unanswered questions will present big challenge for such tests including to establish an uniform criteria for data interpretation, quality control for all different assays, development of more sensitive ways to detect minor mutations, time-consuming issue, and costly issue. Despite these known limitations, drug resistance tests in combination with development of new classes of antiviral drugs may be the only ways that can fight treatment failure, at least for now. 10