WHAT IS
CHEMICAL
HUNGER?
The problem, as everyone who has ever
gone on a reducing diet knows, is not
merely taking the pounds off, but maintaining health and energy while doing it;
then comes the problem of making sure the
weight is not regained.
This book, written by a leading medical
authority, teaches you how to end the
useless and damaging torture of improper
dieting. Learn how to lose weight by eating
correctly—and healthfully.* It's easy,
successful and painless. Your reward will
be a slim, youthful and vigorous body.
* The answer: an understanding of chemical hunger
IMPORTANT!
To receive free advance news of exciting new
LANCER BOOKS each month send your name
and address to:
LANCER BOOKS, INC. · Dept. PDC
26 West 47th Street · New York 36, New York
A LANCER ORIGINAL · NEVER BEFORE
PUBLISHED
TAKE WEIGHT OFF
&
KEEP IT OFF
Max Konigsberg, M.D.
and Louis Golomb
LANCER BOOKS · NEW YORK
A LANCER BOOK · 1962
TAKE WEIGHT OFF AND KEEP IT OFF
Copyright 1962 by Lancer Books, Inc.
All rights reserved.
Printed in the U.S.A.
LANCER BOOKS, INC. · 26 WEST 47TH STREET · NEW YORK 36,
N.Y.
Foreword
STILL ANOTHER book on dieting? There must be a
hundred or so in print at this moment. The one type of
printed matter that rolls even more regularly off the
presses is its arch-rival, the cook book, telling of exotic
haute cuisine and other culinary arts, with all of which
diet is as closely linked as virtue is to sin.
Like sin, fat is something everybody is against and
few know how to cope with. Americans are certainly
diet conscious enough, but they have been offered so
many "fabulous formulas," "miracle diets," "crash"
programs— and now the 900 calorie diet! With
signposts all pointing in opposite directions, one simply
doesn't know which way to turn.
Do you, for instance, believe that fat, when it is not
"glandular," comes only from overeating? (You are
wrong.) That by counting calories anybody can reduce
and stay healthy and slim? Wrong again! That you must
deprive your body to keep it from plumping out? Ditto!
That "dieting," learning how to nourish yourself, is exclusively for fat people? Ditto again.
Nor does medical science speak out in a single voice.
Let us glance at three recent books dealing with diet.
Live Longer and Better by Dr. Robt. C. Peale, says: "Eat
and drink whatever you like. You don't have to give up
your favorite desserts or starchy foods."—but in modera7
tion. We are then instructed in a simplified method of
calorie counting.
But, Calories Don't Count is the comforting title of Dr.
Herman Taller's best-selling book. Announcing a
"revolutionary break-through in medical knowledge," it
cuts down to the vanishing point on carbohydrates, including fresh fruits and vegetables, and invites an omniverous eating of fats: "Eat fat to get slim."
While for Dr. Ancel Keyes, a significant name in
dietetics, fatty foods are the enemy, leading both to
obesity and to heart disease. He, too, urges calorie counting, but directed at a drastic reduction in our fat intake.
No wonder people turn to faddists and food quackery.
But what does a doctor, with no theoretical axe to grind,
think of all this? What does medical common sense advise? I trust I am qualified to express this common sense
view by my twenty-five years of practice involving an
almost daily preoccupation with the diet of my patients. I
am a gastroenterologist (a specialist in internal disorders)
with an abiding interest in both education and research. I
have taught at two fully accredited medical universities in
the New York area. I have also done experimental
research in my specialty, which is closely related to
nutrition.
This book attempts to sum up what physicians know
about diet as "preventive medicine," and how we feel
about such diverse matters as calories, food cultists and
even condiments. You will be guided through the immense field of dietetics, where you will learn the landmarks as well as the pitfalls. And on the narrower, embattled terrain of "dieting," we shall together explode the
booby traps.
When you have acquired a smattering of food facts
plus some knowledge of the workings of your body, you
will be prepared to undertake weight reduction. The
program offered here is fairly certain to meet with your
doctor's approval. For even while it rids you of excess
8
weight, it will at the same time greatly improve your
health and enhance your life prospects.
MAX S. KONIGSBERG, M.D.
with Louis GOLOMB
9
\
Chapter I
DIET AND DIETING
Introductory Note:
THIS BOOK is for you. Written primarily for the overweight, it should prove of equal value to all who have a
curiosity or concern about their body, about what makes
the machine tick—the human diet. It will show you how
to feed that machine for a maximum working efficiency
with least breakdown and greatest durability.
The keynote which we shall sound continually is
"high-protein." Young and old, sick and well, underweight, "normal" or obese—a balanced high-protein diet
will best provide each of you with the nourishment essential to true health and well-being. And for the overweight, a high-protein reducing diet will help you lose
weight painlessly, surely, safely.
Our reducing diet will be painless because it is easy to
follow and pleasant to take. No ineffectual calorie
counting—no flavored yet vomitory mixture or oil to
drink—and no starvation! Simply by eating more of
high-protein foods (meats that stick-to-the-ribs, "anticholesterol" fish, "perfect food" milk and its products),
you will set in motion the physiological processes which
will reshape your body into what it might have been and
can still become.
Our diet is safe because high-protein contains the
source materials which your tissues and organs require
11
for constant repair and replacement o£ its minute-byminute cellular obsolescence. Your body will thus be
preserved while you build new muscle structure in place
o£ the discarded £at. You do not need to starve your
body in order to slim it down.
Finally and o£ greatest importance, our diet is sure
because it attacks the most common cause of obesity,
which is overeating or bad eating in response to the false
pangs of "chemical hunger." If high-protein is to be the
keynote of this book, then its recurrent theme will be
chemical hunger: the gnawing symptoms produced by
your blood sugar chemistry.
High-protein kills chemical hunger through regulating
your blood sugar levels—we shall see how later. The destruction of this pseudo-appetite will let you diet without
having to call upon superhuman control and 24 hour
vigilance. It thereby ensures the success o£ your dietary
program.
A few decades back it was a political rallying cry that
one-third of the nation went hungry. Today, recent polls
tell us, one in three persons is contemplating reducing,
while about one in five has already made the attempt and
backslid. It has also been estimated that about one adult
in four is overweight, that is, at least twenty million
women and ten million men. You are not alone.
In our fortunate land, for the first time in the history of
man, almost all of us can satisfy not only hunger but our
craving for the richest and most luxurious foods. The
average American today can afford obesity and even
heart disease.
A recent Christmas issue of Life featured on its cover
page, in place of the woman or man of the hour, an
equally glamorous plum pudding flambé, with recipe on
an inside page, together with a dozen other luscious and
fat-gathering holiday concoctions. On every side,
through all the propaganda media, our senses are dazzled
by a multi-million dollar processing industry, coaxing
our appetite with a vast array of boxes, cans and bot12
ties packaged by Madison Avenue, all begging, "Eat
me!" "Drink me!" And it would certainly be nice if we
could glut ourselves without fear of consequences.
We are living in a veritable wonderland. Alice in her
wonderland, you may remember, partook of the "Drink
me" bottle and grew so gargantuan she could no longer
see her own feet. Luckily, she was able to dwarf herself
down instantly by eating of a bit of cake. If only we had
that recipe! It is being sought after as eagerly as explorers once looked for the Fountain of Youth.
Later we shall analyze the various magic formulas,
gimmicks and fad diets to learn why they fail. Recently,
the 900 calorie merchants have claimed to furnish a
brand new full diet containing all the essential food
values of protein, carbohydrates and fats, plus vitamins
and minerals. But they already had a precurser several
years ago in McCall’s miracle diet, a six-ounce goblet of
"golden eggnog" drunk seven times a day. When Vogue
countered with its own twenty-five day "New cottage
cheese diet," a battle of the women's mags started. The
New York Times Magazine was then moved to comment
wryly on the "Great American Dieting Neurosis."
Women continue to flock to slenderizing salons and
people spend millions on do-it-yourself home reducing
gadgets. Men and women do a yearly vacation penance
at milk farms, health resorts and spas, where they are
starved, steam-cabineted, "masseured" and electrically
vibrated for a net loss of perhaps five pounds a week,
much of it water, at a cost reaching a hundred dollars per
pound. They then return home emaciated, but flushed
with a hard-won victory, only to recover their fat almost
as rapidly and often with a dividend.
The solution seems to point to calorie counting and
millions of Americans are doing it. If a calorie surplus
produces fat, they reason, then reverse the process. Create a calorie deficit by cutting down sharply on the intake of food and you slim out. Yet this doesn't seem to
work very well and we shall see why in a later chapter.
Put briefly here, it is less the total quantity of food we
13
eat than the kind, the nature of the calories consumed,
that is significant. And this knowledge of food values
must be put to work in a long range program.
Overweight is mainly the product of two factors in our
lives. As we grow older, our food requirements change.
At the same time, we tend to grow more inactive. At the
age of twenty-five we already need less and different
food than that of the growing period. The decrease in
calorie need has been estimated to equal about seven
percent for each decade of life. This means that if your
body required 3500 food calories at thirty, you may need
only 3000 at forty, and at fifty only 2600.
Inevitably, half of the men in their thirties are already
ten percent overweight (above an "ideal" weight.) For
while the normal appetite decreases, we go on consuming as much and even more, if we include as we must
high-calorie alcohol, than in our most exuberant youth.
Thus, at thirty, a man's first bulge appears, at thirty-five
a waistline, at forty the paunch.
Even with moderate indulgence we gain weight because we exercise less and less in later years. Older people have always been more sedentary. Before the advent
of steam heating, however, their bodies burned many
calories daily to keep themselves warm and to maintain
a normal temperature of 98.6. Today, our automated
industry and farming, gadgeted housekeeping, our motor-driven, push-button, television-viewing society has
greatly reduced the daily expenditure of energy. The
unused surplus of food taken in is converted into fat and
stored in tissue throughout our aging bodies.
Are you merely plump and appearance-conscious,
heavy with little fat, only slightly overweight, or decidedly obese? There is a simple rule-of-thumb by
which you can judge. Start with a base of five feet
equaling a hundred pounds. Then add five pounds for
each inch of your height above five feet for a medium
frame, going up ten percent for the large and down ten
percent for the small frame. Notice there is no age factor
in "ideal"
14
weight since, theoretically, all weight increase should
have stopped with your body growth.
Then check the result against the weight table in Chart
I of "average" weights, in relation to height and frame,
derived from insurance statistics. You may congratulate
yourself only if you are at least 10% below the American
average—this would be your "ideal," "desirable" or
"best" weight. Actuarial experts tell us there is a proved
correlation between "best" weight and our health and life
prospects.
While obesity itself has been called a disease, it is in
fact a symptom closely associated with numerous disorders. Thus, fat is never listed on the medical certificate
as the killer. People die of diabetes, kidney disease, coronary heart disease, a "stroke," and so on. But we know
that fat persons tend to diabetes, that they often infect
their kidneys, and that a heart or hypertension case with
obesity has a far greater chance of being stricken and less
chance for recovery.
You may be overweight without, as yet, showing any
grave symptoms. But are you mentally as well as physically vigorous, or sluggish, and do you tire easily? Obesity is also commonly linked with disorders of metabolism, such as gout, and with the minor ailments of
indigestion, constipation, muscle pains, etc. It is, in addition, uncomfortable in warm climates or in hot weather
and, finally, it is ungainly and sometimes grotesque.
There are few nastier epithets than "fat slob." If the chart
shows you as overweight (exceeding even the "average"
overweight), you should feel strongly impelled to reduce.
Is all overweight obesity? Your above-average weight
may be due less to fat than to a large frame with heavy
musculature. Such a person does fine in normal health,
but when disease strikes you are none the less more
vulnerable. Reduce down to the norm and, if possible,
below it. For optimum health prospects we should all
approach our "best" weight.
15
AVERAGE WEIGHTS FOR MEN AND WOMEN
According to Height and Age
Weight in Pounds (In Indoor Clothing)
Height
(In Shoes)
Ages
50-59
Ages
60-69
140
144
148
152
156
161
165
169
174
178
183
187
192
197
203
142
145
149
153
157
162
166
170
175
180
185
189
194
199
205
139
142
146
150
154
159
163
168
173
178
183
188
193
198
204
122
124
127
130
133
136
140
143
147
151
155
159
164
169
174
125
127
130
133
136
140
144
148
152
156
160
164
169
174
180
127
129
131
134
137
141
145
149
153
157
161
165
Ages
20-24
Ages
25-29
Ages Ages
30-39 40-49
1
134
138
141
144
148
151
155
159
163
167
172
177
182
186
190
137
141
145
149
153
157
161
165
170
174
179
183
188
193
199
Men
4'10" ..................
11" ..................
5' 0" ..................
1"...................
2" ...................
3" ...................
4" ..................
5" ...................
6" ...................
7" ...................
8"...................
9" ...................
10" ...................
11" ...................
6' 0 " ................
5' 2" ................
3" ...............
4" ...............
5" ...............
6" ...............
7" ...............
8" ...............
9" ...............
10" ..............
11" ..............
6' 0" ................
1" ..............
2" ...............
3"..................
4"..........................
28
132
136
139
142
145
149
153
157
161
166
170
174
178
181
102
105
108
112
115
118
121
125
129
132
136
140
144
149
154
Women
107
110
113
116
119
122
125
129
133
136
140
144
148
153
158
115
117
120
123
126
129
132
135
139
142
146
150
154
159
164
+
+
+
+ Average weights not determined because of insufficient data.
Source: Build and Blood Pressure Study, 1959, Society of Actuaries.
16
Certainly, an above-average overweight of ten pounds
or more is a clear danger signal. If you doubt that you
are obese, study your body. There will be puffs of fat in
your cheeks; your flesh will billow out and sag. In a man
the fat usually collects at the neck and in a ballooning
waist, while women gather fat in layers at the breasts
and buttocks.
A pinch test may be convincing. Take hold of a flap of
skin at the back of your arm or at the side of your lower
ribs. You are holding pure fat between your fingers. A
quarter of an inch of skin thickness is normal. The
excess above this should persuade you that you have let
yourself become obese.
Undeniably, the most common cause of fat is overeating, that is, eating more food than your body metabolism
can burn. Fat people often hide their secret shame over
their condition and its cause by a surface jollity and by
alibis which they themselves come finally to believe.
A favorite self-delusion is, "I can't do anything about
it. It's my glands." Glandular malfunctioning can be
quickly ruled out by your physician. He may order a
BMR (to check on the metabolic rate) or, better yet, a
PBI (protein-bound iodine blood test), and perhaps also
a skull x-ray of the sella turcica, the bony covering of
the pituitary gland to see if it is enlarged.
Only two to five percent of obese persons are "glandular." These can be treated by injections and pills to control the pituitary or thyroid. The normally fat person
must look elsewhere for cause and cure.
There is a more common obesity due to faulty metabolism (the rate at which food is burned). Patients say,
with a great deal of truth: "Everything I eat turns to fat."
Such people do pose a problem for there is much about
metabolism we do not yet understand. If the imbalance
cannot be corrected, they must learn to live in terms of
their handicap. They are probably eating too much or
badly or both.
Others blame their heredity. "It runs in my family,"
patients have said. "My parents, my children, we are all
17
this way." But the hereditary factor in overweight is
slight. Frame is inherited, not a tendency to fat. The
supposed family characteristic is merely the result of
faulty eating habits transmitted by emulation which must
now be unlearned.
One sometimes hears frank confession: "I just can't
resist food . . ." "I must have a snack between meals . . .
before bedtime ... I keep nibbling all day, etc."
"Whenever I feel tense, I eat, mostly sweets. . . ."
Overeating at its various levels may be simple selfindulgence or a defense against outside pressures and
inner tensions. And always there is an element of compulsion.
We shall return in Chapter II to these psychological
obstacles to weight reduction. Here one can only repeat
what every doctor says when faced with compulsive behavior: You must learn restraint, self-discipline! "Appetite grows by what it feeds on." "Assume a virtue . . ."
said Hamlet to his mother. "Refrain tonight and that
shall lend a kind of easiness to the next abstinence; the
next more easy."
Yes, all it takes is will power, the very power you have
shown yourself lacking in. This advice, known as "bootstrap psychology," must always sound a little hollow.
Nevertheless, only you can lift yourself up out of your
predicament. You will develop the necessary determination when you recognize its value for your health and
well-being. Few persons knowingly eat themselves into
the grave.
There is an apocryphal story of a physician who
shocked severely obese patients into maximum cooperation. He laid before them a life-size photograph of a rat
suffering from bulimia. The little creature had been tormented by experimenters, as life harries all of us, into
finding an ever-present solace in food through incessant
eating. The photo shows him tottering on his tiny legs,
his body swollen to the point of collapse. The patient is
presumably seized with such disgust that he will never
18
gorge himself again. (By the way, an underfed rat appears to live longer than a fully fed one, and this may
hold true also for humans.)
In most of us, however, a vision of the "body beautiful" should be more compelling than the sight of a
bloated rat. What is your mental image of yourself, the
real you?
Men tend to see themselves mostly a shade taller than
they are, more slender and muscular, really not far removed from the youth of college or senior high school
days.
A woman's self-image is more dependent on social position (slenderness is said to be a female suburban status
symbol) and on the latest modes, whether from Paris or
the Sears catalogue. She will go seeking a "new self' in
the beauty salon and on shopping sprees, when it is in
fact being shaped by her way of life and in her kitchen
and dining room.
If you hold before yourself an idealized self-portrait of
a healthy body instead of a taunting flesh, it may help
fortify your resistance to the insidious vice of even a
mild gluttony.
We return to the one person in five who has exercised
restraint and then retrograded. A woman patient had over
the years gone through a variety of highly touted
reducing regimes. Five feet two, she had let herself
fatten now to one hundred fifty pounds, an unhealthy
condition.
Yet she had periodically succeeded in losing weight on
these starvation diets. As an invariable result, her skin
would sag into overlapping folds where the flesh (and
muscular tissue) had been. Her face and hands, starved
of necessary proteins, would wrinkle. She was nervous
at work and irritable at home, by her own confession,
unlivable-with. And so each time back to the old feeding
trough. By now, her health was also suffering from the
repeated fluctuations in weight which can be very
destructive.
19
Anybody can reduce by consuming only one thousand
calories a day, even when they subsist on ice cream. But
at what cost?
Drastic reducing on a "crash" program must bring
equally drastic results. For your body will crave all the
more the essential food which it has been unjustly denied.
The result is a compensatory gorging and a return to
former eating patterns, with increasing obesity. Losing
weight is not meaningful unless the weight loss is later
maintained by a program of intelligent feeding. Don't
look for short cuts, the nine or thirty-day diet. Develop
the psychological readiness for the long, the life-long
haul.
By all means, eat smaller portions. But remember that a
weight loss of over two pounds a week is not desirable. A
too stringent curb on necessary food forces the body to
consume valuable bone and tissue structure and lowers
your resistance to disease.
It is remarkable that, with all the amount and variety of
foodstuffs available in our country, a recent study
revealed that only twelve percent of a cross-section of the
population escaped deficiency in one or more vital food
factors. Starvation in the midst of plenty. And, no doubt,
many of the undernourished were among the fat and
overweight, a double retribution.
What dietary program shall we advocate once we have
explained the role that nutrition plays in the human body?
By a limitation of certain types of food and a substitution
of others, we will help you reduce down to a satisfactory
and permanent balance between calorie intake and the
expenditure of energy. The American tendency to eat
softer, sweeter and fatter must be corrected. Only a highprotein diet accomplishes these ends.
No medication is needed. The right foods are in themselves curative. When an obese patient comes to me, I
map out a diet which may vary with the degree of obesity, the daily expenditure of energy at work, how much he
or she can safely lose and how rapidly. No less im20
portant is a program of physical exercise suitable to the
age, capabilities and daily routine.
Walking is fine, long and vigorous walks of two to
five miles a day. Golfing is excellent, if the lost calories
are not then replaced in locker room drinking. Tennis,
swimming and horseback riding are superlative for the
younger obese with strong hearts. Meanwhile, in your
daily activity move zestfully, intensely. Indolence and
passivity are as conducive to fat as overeating is.
Recently, when a high-protein diet was urged upon an
obese patient, Mrs. A., she protested: "But I am on highprotein!" And her smile said, "That's old hat."
We checked. She did have an egg each day for breakfast, about 4 pound of meat or fish for dinner and occasionally some for lunch—and that was it. (No milk or
cheese, to which she claimed to be allergic.) The remaining high-protein was supposed to be supplied by
vegetable proteins and "enriched" cereals and bread.
Her maximum protein intake per day tallied up to less
than 50 grams, just half of what she should be eating. A
hundred grams is the daily optimum requirement for the
healthy adult, and particularly in weight reduction.
Yes, high-protein is no novelty, any more than some
other ideas circulating about, such as peace and brotherhood. But an idea becomes valuable only to the extent
that it is properly understood and applied—and the
analogy isn't altogether far-fetched. When all the nations
of the world can offer their peoples more and better protein, we shall be a lot closer to universal peace and
amity. We mean better protein than the starvation rice or
millet upon which the hundreds of millions eke out their
destiny.
We in America who have unlimited Grade A protein
foods at our disposal have not yet learned their crucial
role in building the body and maintaining its health.
Mrs. A., a sedentary housewife, had fattened on "highprotein" that was rather on the sweet and starchy side.
She had come to the doctor to ask for an appetite depressant.
21
"I know I eat too much," she said. "I can't understand
it but I'm always hungry." She stuffed herself at the
table. Yet, between meals, she felt faint unless she was
munching, usually on something sweet. Ashamed of her
voracious appetite she nibbled on the sly, away from the
family, and had even been awakened from sleep by the
urge to pilfer the ice box.
We earlier referred to the psychological stresses that
lead to compulsive eating and we devote the following
chapter to them. Somehow, to these non-psychiatric
eyes, Mrs. A. did not appear psychologically motivated.
We knew her as a quite stable person who enjoyed a
normal sex life in a fulfilling home environment.
Her hunger pangs, apparently fictitious, seemed very
real to her because they were actually experienced. They
simulated and exaggerated true hunger and were all the
more irresistible. They were symptoms of the "chemical
hunger" you read about at the beginning of the chapter.
To the doctor they indicated a deficiency of sugar in the
blood, in her case we discovered, an extremely low
blood sugar level.
If the reader is overweight it is almost certainly due to
overeating, though the need may not be as compelling as
in Mrs. A. Then, whatever the underlying psychological
cause, your false appetite is likewise a manifestation of
this chemical hunger. As you read on, you will learn the
cause and effect linkage between your food and your
blood sugar levels. You will come to understand how a
true high-protein diet helped Mrs. A. reduce successfully
by killing the hunger pangs which had made her overeat.
We wish we could trumpet out the story of highprotein in tones of command with the selling power of
radio and TV. "Reduce by destroying chemical hunger!
Banish the midriff bulge! Keep nutrition up and calories
down! A fabulous way to a lovely skin—to a new life
through . . . I"
This book, however, is dedicated to persuading you
with the quieter voice of reason that you can indeed eat
22
your way to better health, appearance and longevity. For
the high-protein will safeguard your weight reduction
because it strikes at the physiological roots of overeating—the low blood sugar of chemical hunger.
23
Chapter II
PSYCHOLOGY OF THE FAT
AND THE LEAN
"HOW DID I ever let myself get this way?" a patient
once asked. "And how can I get out of it?" In this chapter we shall go into the psychological "how" of both
cause and cure of overweight.
Most dieting books and manuals and some doctors
sound a single theme on an accusatory note: "You became fat through overeating. So you must cut down on
food to reduce." This mechanical view of the problem
has led to calorie counting and "crash" dieting.
Avoiding the redundant obvious, let us say rather:
"The fat you acquired by overeating, and the overeating
itself, served a psychological purpose—they fulfill for
you some emotional need. Therefore, your success in reducing (on a balanced high-protein diet) will depend
upon an understanding of your impulses, of what
prompted you. Only when you can hurdle the obstructive emotion, will you be able to build healthier eating
habits.
Breaking any habit pattern is difficult enough. How
much harder is it when it involves food, our deepest
need, shared by man with all animals and perhaps with
higher species. Its satisfaction is even more fundamental
and durable than the sex urge, even if no "Romeo and
Juliet" has ever been written about a passion for waffles.
24
Extending from before birth throughout our lifetime, it is
virtually synonymous with life itself.
"I just love to eat," a grossly overweight patient confessed, as if that were the sin. We should all love food
(in moderation), though its primary function is to provide energy and cellular replacement.
Too much of American abundance is snatched down
in haphazard undernourishment at the "greasy-spoon"
cafeterias and lunch wagons and the kitchenless soda
counters which constitute much of our eating out. While
perched on the opposite gastronomic pole is the
gourmet, intent only on gratifying his taste buds, with no
regard for the blossoming fat. He lays on with lavish
butter spreads and cream sauces at home and scours the
continents in quest of Cordon Bleu cookery. But surely
there is a middle path. Cannot the science of nutrition be
blended with the culinary arts to provide an American
cuisine, nourishing and delightful yet unfattening?
Still, why do we overeat? Let us examine together a
number of cases of obesity as they present themselves in
a doctor's office, naked in the spirit as in the flesh.
The patient mentioned above, whom we shall call
Mary, could "chew a brick wall" when hungry, though
she and her family managed nicely on fatty steaks and
fried potatoes, along with pastries and puddings and vast
amounts of cereals and bread. She was raised, she
recalls, on potatoes and bread, in an impoverished home
where they were trained to "clean the plate." She grew
up into plump womanhood and has been growing out
since.
Married to a well-paid truck driver, she and her husband go off on weekly shopping forays to the supermarket and indulge in eating sprees at home. Their
children, conditioned by them, already display a "family
tendency" to overweight. Fat has long been considered a
mark of social status in many parts of the world where
only the wealthy can afford it. In our affluent society
there has been a democratization of obesity. The worker
25
husband could now blow himself up to look like the
communist caricature of a banker—but should he?
For Mary, food has become a symbolic substitute, as
the wafer and wine are in church ritual. It represents not
only health and well-being but the security she missed in
childhood. She is making up for her early deprivation by
overeating now. Compensatory eating, to fill a real or
imaginary need, is perhaps the most common cause of
overfeeding and obesity.
Another patient, Jane, had weighed a hundred and
twenty pounds before marriage. Six years later she
weighed in on the office scale at a hundred and sixty.
What had happened?
"When I was pregnant with my first, I had such a
craving for sweets ... I must have felt I had it coming to
me."
As solace, she regularly got down mountains of ice
cream topped by pyramids of whipped cream, plus peanut
butter and jelly sandwiches with heavily sweetened
coffee. Her faulty eating habits, in disregard of a doctor's
diet, luckily did not endanger the child. After its birth
there followed a half-hearted attempt to reduce that failed.
The same process of consolation eating and of permanent
weight gain occurred with the second and then the third
child. (Psychologists have suggested that an inability to
lose weight after giving birth may indicate an
unconscious wish to hold on to the baby.)
Yet Jane did not need any psychiatric probing. She
came to understand that her obesity was due to selfindulgence growing out of a destructive self-pity. She was
free now to undertake a dieting regime that would rid her
of her incubus of fat.
Compensatory eating, as with Jane and Mary, is often
combined with "tension eating." John, a successful lawyer
working under great pressure, could not deny himself that
second dessert or third cocktail. His work built up
powerful tensions which he dissipated by wolfing down
huge quantities of food and drink. Eating, spiced with
alcohol, soothed and sedated him.
26
John apparently needed this safety valve. He could not
unwind at his work, though totally engrossed by it, nor
did he find adequate release in an unsatisfactory home
life or in social relationships. At fifty-two, of medium
height and frame, he weighed close to two hundred
pounds.
Always healthy and functioning at high gear, he was
jolted from his complacency when he was rejected for
additional life insurance. At the doctor's office he later
learned of a heart "irregularity." He knew then he had to
reduce weight by a drastic overhaul of his eating and
drinking habits.
Anne, who worked in an office at a tedious job under
a difficult boss, similarly combined compensatory with
tension eating. She nibbled chocolate bars and cookies
to "get through the day" (to ward off the tension) and
had a daily malted ice cream with some meatless sandwich for lunch. Inadequately nourished, she undoubtedly needed the extra sugar ration for short spurts of
energy, but the surplus was being changed by her body
chemistry and was accumulating as fat.
Becoming less attractive to men and approaching
thirty, she mostly sat home evenings "eating her heart
out" plus whatever the icebox held for snacks during
television watching or reading. "I felt so sorry for myself," she said, "thinking of the fun I used to have and
what I was missing." The more sedentary, the more
tense, the more she nibbled and fattened.
Then, threatened with the loss of her job because she
looked so "sloppy," she several times crash-dieted for
momentary weight losses she could never maintain.
What was needed was a profound transformation of her
eating patterns. But before she could diet successfully,
she too had to learn to accommodate her tensions.
Both John and Anne considered themselves victimized
by the pressures of their work. In other cases, tension
leading to overeating and obesity can be brought on by
some emotional crisis such as the death of a loved one,
failure in sexual relations, or by apprehension over some
27
impending event. In addition, there is the fearful daily
battering most of us take, and the downright disagreeable
chores attached to much of living— A perfect rationale
for overeating, if you are looking for one.
Yet tension in itself is a part of our life equipment, as
natural and protective as our reaction to heat and cold. It
mounts when we are confronted by some looming threat
to our safety, happiness or self-esteem. And we are
certainly living in a dangerous and difficult time,
properly called the "age of anxiety." But when, if ever,
from its earliest beginnings has mankind lived without
anxiety for sheer survival?
Few persons are blessed with an environment free of
stress or with an inner serenity immune to it. The less
sorry we feel for ourselves the closer we come into harmony with the relentless universe. And the less -need we
have to explode our tensions through food and drink.
The fat we gather in overeating or inactivity may also
serve its own subconscious purpose. Henry was a plump
and pampered boy who was called Fatty-grub by the
other kids. Exiled from their play by his flabby muscles
and their scorn, he did grow into a fatso. He protests he
did not eat more than other boys, at least not until later;
he simply became increasingly inactive. That this holds
generally true for obese children was borne out in a
recent study of their eating and exercise habits.
"Nobody (except my mother) likes me," he decided.
The world appeared as an enemy to be kept at bay. He
ate to fill a psychic void and his fat was transformed into
an insulation, a bulwark against people, also an alibi for
'lazy" behavior at school and slow movement outside.
"Don't hurry me," it said. "You see I can't go any faster."
He had disqualified himself from boy-girl contacts
(girls laughed at him), and later from vying for economic
betterment. At thirty-three, of more than average
intelligence, he held a menial job and was unmarried.
His fat had thus cushioned him against marriage, the
economic struggle, the very give-and-take of life itself.
28
Henry had always felt that his condition lay basically
in his make-up, probably glandular or "something wrong
inside." Yet medical tests failed to reveal any glandular
or metabolic disturbance. He came to the doctor because
he had reached a point in his adult development where
the normal urge had risen to win a mate, to make a better
place for himself in society. That is, he was excellently
motivated to diet and exercise himself back into the
mainstream of life. He will succeed in the degree that he
feels he can dispense with his protective buffer of fat.
Florence, who is receiving psychological help, was
able to analyze the meaning of her obesity. As a girl she
was normally slim but, "I felt like such an ugly duckling,
so unsure of myself. Whenever I had a date, my face
would break out." Her anxiety made her so selfconscious she dreaded the ordeal and wasn't very good
fun—one way of keeping her from competing for male
companionship.
After a wretched childhood, she got on badly with her
quarreling parents and was desperately afraid of marriage, of sexual aggression. Then came the solace overeating and obesity. Her fat was a refuge from an unhappy
home life, a shield against all feeling but primarily
directed against the opposite sex. Like Henry, she had
taken herself out of competition. Unlike him, however,
she would periodically attempt drastic reducing
measures.
In one of her slimmed-down periods she met a man
and persuaded herself into accepting a marriage proposal, mostly to take her "out of the house." But soon a
violent rejection of sexual life was expressed in
omniverous eating. The fat returned in bulk and it
succeeded in its unconscious purpose of erecting a
barrier against the husband, who turned to other women.
Left to herself, "I went to pot. I lost interest in everything except food: friends, the workings of my brain, the
world outside."
At the doctor's office she described alarming symp29
toms, mostly of anemia, felt "sluggish, numb," and was
starting to lose her hair which she treasured.
Since her divorce, Florence has undertaken a vigorous
campaign of rehabilitation. With a newly developed selfawareness she is determined to slough off the sheath of fat.
Setting a minimum goal of one to two pounds a week, she
keeps a bathroom chart for a constant check-up on her
progress.
At first she would break down and cheat and each ` time
felt ashamed enough to give up. Then she placed a mirror
inside the refrigerator and her bathroom scale next to it. No
more icebox raids. As a final gimmick, whenever shopping
for clothes, she buys a frilly dress one size too small which
she cannot wear till she reduces down to it. Her ingenuity
has paid off. On a minimal high-protein diet, which sustains
her for a demanding secretarial job, she has in several
months lost over ten pounds and is well on her way.
Where fat serves as a shield against love, companionship,
or economic striving, we are caught up in a vicious circle.
The fatter Henry and Florence became, the less chance of
winning a mate, advancement or good social relationships.
They would then eat all the more to make up for what they
lacked. Food thus came to replace these adult
achievements. The patient has now regressed to early
childhood, but without the natural safeguard of the normal
child who does not eat beyond satisfying hunger pangs.
Such compulsive eating may at times turn obsessive,
resulting in a gross deformation of the human shape.
Margaret, a patient in the psychiatric ward of a local
hospital, was a victim of obsessive eating. The psychic
roots of the malaise lay in the death of a beloved parent
early in childhood. She was at twenty-seven so grotesquely
obese she could barely be maneuvered through the door.
She appeared otherwise quite rational and had lately
expressed an interest in dieting.
"We don't encourage these people to diet," a psychiatric
worker explained. "What will replace for her this
30
all-absorbing need? . . . Love? Loving and being loved
are so uncertain. Food is always at hand."
Though obsessive eating is fortunately rare, with the
superabundance of food and the scarcity of love there
may be a germ of it in much of obesity.
In all the cases presented here except Margaret's what
prognosis would you make for each patient? What do
you think are your chances for success in dieting? According to the findings of a Cornell University study,
there is a direct correlation between successful reducing
and the emotional stability of the dieter. That is, an
emotional unbalance tends to maintain a food
imbalance.
A group of over a hundred dieters was subdivided into
three categories of "high," "average" and "low" emotional stability. The top stability group met with fair to
excellent results. They had permitted themselves
through middle-age inactivity and over-exercise at the
table to become obese. They mostly enjoyed eating and
had little knowledge of their bodily requirements.
Learning about the causes of overweight, they made
excellent subjects for any dietary regime.
In the middle stability group, representing the American average of overweights, the results ranged from
moderate to fair with few failures. These people required not only food facts but an insight into their emotional problem. The obesity could be controlled to the
extent that they faced up to the cause of their overeating
in their inner tensions and anxieties.
The low stability group was only moderately successful in about a third of the cases, with outright failure of
more than half. Many of these persons apparently
needed psychiatric help to implement a dieting program.
Mayo Clinic psychiatrists have indeed advised against
any dieting at all for persons with a deep-seated emotional disturbance. Before the safety valve of food is
removed, a second line of defense must be established.
Failure, adding feelings of guilt and ineffectuality, only
exacerbates the emotional unbalance. These individuals
will sometimes develop fresh symptoms called "the diet31
ing depression." At least they should not make the attempt without the supervision of a doctor. Even for the
more stable, it has been suggested that dieting should be
postponed during a period of great stress, as in sickness
or the menopause.
A small minority of persons, therefore, may not be
able to undertake a dieting program unaided. The overwhelming majority, however, the average American
overweight, can learn on his own to control, modify or
redirect his impulse to overeat—once he understands its
"defensive" origin.
Eating, like all life activity, must be a compromise.
Adults measure an impulse against its consequences. We
do not race a car to the maximum shown on the dial nor
do we often kill those we dislike. We likewise can muster self-discipline to overcome habits of self-indulgence.
There are surely better ways of expressing inner conflicts than by punishing our stomachs and deforming or
enfeebling our bodies.
An awareness of the urgency (see the following chapter) and a readiness, a total commitment to retraining
your attitudes and habits must come first. If you are
strongly enough motivated, you will reduce your weight.
Can you now apply what you have read here to your
personal psychological problem? (If you have one—and
you may not). Ask yourself: "Why do I overeat? What is
my special weakness—all day nibbling, "coffee and"
breaks, between-meals and bedtime snacking? Do I
know my actual food needs? What substitute gratifications can I find? Do I exercise enough? And how can I
dissipate my daily tensions through means other than
food?"
A pamphlet of the National Association for Mental
Health suggests ways of handling one's tensions that we
can apply to dieting. Here are some suggestions:
1. Channel your frustrations into productive activity or
else seek some satisfactory displacement in daily recreation. There are ample diversions to choose from other
32
than food to help dispel your "blues." A normal sex life,
when it is possible, is of utmost importance.
2. Find a physical outlet for your emotions. Schedule
regular and pleasurable exercise, as violent as your age
and bodily condition allow. It will serve the double purpose of exploding tensions and consuming calories. If
you have a garden, dig like mad; if a home owner, you
can putter, but molto furioso. At the very least, take long
and vigorous walks.
3. Make yourself accessible to others. Don't
withdraw. Social relationships will take the edge off the
personal anxieties you have been sedating with food.
4. Involve yourself in some community service
organization. Working for others will distract you from
yourself; feeling sorry for somebody else will keep you
from consolation eating.
5. If you need guidance or psychological aid, there
are various community and welfare agencies where you
can apply. To find out about counseling, get in touch
with the local or state Mental Health Association.
6. And if you suspect there is a medical problem attached to your tensions and overweight, go see a doctor.
He will guide you in your dietary regime and, where it
is indicated, will recommend psychological help.
(Of course, if the doctor is himself overweight,
through carelessness, neglect or the same pressures to
which you are subject, he may be somewhat perfunctory
or defeatist in his attitude. Then proselytize him. It has
been said: "Doctor, cure thyself!")
You may be reading this book with a jaundiced eye.
You have tried so many Get-Thin-Quick schemes and
failed. This holds true more often for women, since men
have been proven, statistically, to be better dieters. Perhaps they were convinced by the recent splurge of publicity on heart disease that it is a matter of life and death
for them. While a woman may still feel that all that is at
stake is vanity, which is really her pride that goeth
before the fat.
A doctor sees calorie-counting women patients with
33
little energy, taut skin and frazzled nerves. One is almost
tempted to say they might be better off slightly overweight, rather than having to wage their ceaseless battle
"against nature," lured on by the glamour of slenderness
exemplified by the latest French Look and the undernourished, breastless and hipless American mannequin.
Compulsive dieting can be as neurotic as compulsive eating. Inevitably, many of these women in their middle
years sink with a sigh of relief into the protective folds of
fat, accepting it along with gray hair as part of the aging
process. But it isn't; and they need not.
The grossly overweight reducer who has never stuck to
a diet may require (even after all the exhortation in this
chapter) the added incentive and stimulus of doing-ittogether. Alcoholics Anonymous has shown the way to
effective group therapy, and overeating obviously has
much in common with overdrinking.
The F.A. (Fat Anonymous) movement was initiated in
1954 by Dr. John Pate, Health Director in Washington
D.C. It has since spread country-wide. If you should be
interested in joining or forming such a group, here is how
they usually function.
A number of overweights come together in a club under
the direction of a doctor, health officer, or public health
nurse. They pledge to follow a dietary schedule and to
appear at consecutive weekly meetings over a period of
four to six months. Members must lose at least a pound a
week or they are dropped.
At the weekly meeting there is a public weighing-in
ritual accompanied by much chaffing and applause, and
also by laughter and tears. These people are sold on what
they are accomplishing and there are few dropouts and
little backsliding. The atmosphere of sympathetic pullingtogether and of the censure or approval of fellow sufferers
has worked small miracles for thousands who could not
succeed by their solitary effort.
Whether you diet singly, as a family, or with a group,
here are some final do's and don'ts:
1. Be firm in your resolution to make significant ad34
justments in your living patterns but don't become fanatical. Too great rigidity tends to snap back in a
counter-reaction.
2. Set yourself a modest and attainable goal. Reach it
in small stages of one to two pounds a week. Each
cumulative victory will fortify you for the next advance.
3. Don't forget that exercise, recreation and a limiting
of alcohol
are
as
important
to
weight
maintenance
as proper eating. The only calorie counting you need do
henceforth is of the second drink and of rich desserts.
4. Follow the high-protein diet which will be explained in subsequent chapters. It will bring your weight
down and keep it at a metabolic balance.
5. The cook in your home should use the offered
menu suggestions creatively, so you will relish the
smaller portions you must eat at the start. Take time for
eating and have congenial surroundings that make it
pleasurable. If you must eat out, be discriminating in
your food choices.
6. When entertaining or being entertained, let your
friends understand your problem, again without being
too rigid, and they will cheerfully cooperate in your venture.
7. Lastly, if you follow through, your reward will be
not only pride of accomplishment but the joyous feeling
of being youthfully attractive and healthy.
35
Chapter III
THE ILLS FLESHINESS IS HEIR TO
IN THIS chapter we shall try to sum up what medicine
knows about the diseases which ravage obese man—
much like scratching the Lord's prayer on the head of a
pin.
If we began with "Diet or die!" it might scare the fat
off some readers and worry the mild overweights back
into slimness. Such an ultimatum, while dramatic
enough, would be in pretty poor taste. Yet it isn't far from
a doctor's lips at times, when an obese patient comes to
him with heart disease, hypertension or diabetes.
Consider heart disease, the nation's number one killer
that takes 500,000 victims each year. Whether or not certain foods help bring it on and others can avert it we shall
go into later, in a review of the great medical debate on
cholesterol. But of this there is no doubt: When an
overweight develops a heart ailment or other grave
disorder, obesity will greatly aggravate it and may deal
the death blow.
Perhaps imagery will make the point more vivid. It is a
fact that you can read your life expectancy in the numbers on your bathroom scale. Or, put differently, your
waist line does indeed measure your life line (each excessive inch—minus one year).
How do we know? From all our medical observation
36
and, lately, from vital statistics, some of which are summarized and interpreted for you in the graphs that follow.
And though they may be dull, and surely troubling,
please don't skip over them, for they are literally of life
and death importance.
Let us say modestly that you are (only) fifteen pounds
overweight. Imagine yourself carrying about a fifteen
pound baby all the live-long day, or holding a pack of
that weight on your back—standing with it, propelling it
forward, lifting it up steps.
"Oh," you argue. "Weight isn't concentrated that way.
It's spread across the body."
True. Fat at first hides cunningly, so that you are
scarcely aware of it. But your heart knows, for it must
pump fresh blood bringing nutriment to every microscopic cell of it each waking and sleeping moment of the
twenty-four hours and draw off the wastes. And your
blood knows as it surges and strains to reach it and
sometimes over-performs, just as the heart may, resulting
in the hypertension of high blood pressure. And the
lungs know as they suck in the extra oxygen needed
(often to burn "extra" food—compounding the felony)
and heave out the extra carbon dioxide and water vapor.
Double your overweight, as you are likely to do if you
follow the American trend (see Graph I, below), and you
will then know it too. Even after mild exertion, the obese
person feels his heart pounding wildly, his blood racing,
his lungs gasping for breath.
Many stout persons suffer from inadequate aeration of
the lungs. They get easily winded and have trouble supplying the body with oxygen. (This is why overweights
with asthma and chronic bronchitis do not do as well and
have a poorer prognosis than the lean ones.) When the
condition is associated with a heart ailment, the heart
muscle is more likely to fail. The resulting decompensation can bring on a vicious cycle of fluid retention
in the body with the lungs becoming water-logged. Not a
hopeless situation, but one to be avoided—by reducing.
37
You may be overweight, yet feel perfectly fit and look
it. Perhaps you should know about a condition called
Polycythemia, in which the number of blood cells is
greatly increased (with the hemoglobin count above 100
and up to 120). Such persons are ruddy-cheeked and
appear muscular and strong; they have mostly had a
background of athletic youth. Then, in mid-life, they
develop an enlarged heart. With it comes inadequate
blood vessel function which can lead to failure of the
circulation.
The "healthy" overweight finds any physical stress
situation more difficult to handle and, particularly, a
grave illness. Let him come down with an ordinary "flu,"
involving lung congestion, and it may turn serious. You
have perhaps seen or heard of this happening to someone
you know. He is like a loaded truck lumbering uphill
with carburetor and spark plug trouble. Unable to burn its
fuel properly, it can't pull the load and starts coughing
and sputtering. It sometimes stalls, never makes that hill.
The most common cause of heart disease is arteriosclerosis, or hardening of the arteries. In this degenerative
condition the arteries lose their elasticity because their
linings have become encrusted with deposits of fat-like
substances. These join to form thick pads called
atheromatous plaques, which impede and sometimes
entirely stop the free flow of blood to the heart. The
artery then resembles a corroding iron pipe in which rust
has formed and gradually coalesces, narrowing the
passage to a pin-hole.
If the arterial blockage is in the brain, it may result in a
cerebral hemorrhage or "stroke." In most cases thrombosis has occurred—the plugging of a blood vessel by the
formation of a clot which cuts off the blood supply to a
particular area of the brain, which is eventually
destroyed. Far fewer strokes are produced by the actual
rupture of a blood vessel with hemorrhaging. Still less
frequent is the embolism caused by the lodging of some
foreign substance or tissue (sometimes fat!) in a brain
38 .
artery. (For the fatal correlation of strokes with overweight, see Graph II.)
Heart disease itself strikes mainly in the middle years,
but there is no age limit. One in five men die of it in the
prime of life, 35 to 44; one in three at 45 to 64. During
the Korean War, coronary blood vessel narrowing and
death from heart disease were discovered in young soldiers of 19 and 20. While it also attacks normal weights,
from Graph II you can see that overweight increases the
fatality by 43% to 51%.
The tendency to arteriosclerosis, heart failure and
strokes is greatly enhanced by high blood pressure. Here
we observe a significant up-and-down correspondence
with overweight. As a person with mild blood pressure
gains weight, his pressure rises. But fortunately, the converse holds true. When he reduces, lessening the strain
on the heart, pressure falls and may approach normal.
Diabetes and gout are closely related to obesity,
though neither is caused by it. Twice as many overweights develop diabetes; over sixty percent of diabetics
are obese. What happens is that the body mechanism for
converting starches to glucose has gone haywire. This
condition is characterized by increased sugar levels in
the blood and possibly by sugar in the urine.
Diabetes runs in families, implying some hereditary
predisposition. When such a person with only a slight
elevation in blood sugar gains weight, his sugar level
rises and he may become diabetic. But when he reduces,
paralleling what happens in high blood pressure, the
blood sugar level falls. He now gradually improves his
glucose tolerance and is less restricted in diet. To the
extent that he maintains normal weight, he will function
close to normally. Today the diabetic who cares can live
as long as the next person.
Gout is a metabolic disease which became a cartoonist's joke and also provided laughs in early Chaplain
films. The layman can instantly diagnose it in the cartoon
when he sees a fellow in a wheelchair with a well-padded
and bandaged leg held horizontally—especially
39
if the man is fat and the caption or "balloon" conveys a
British accent. Even though Dr. Johnson had the gout
and managed despite it to rule the English literary roost,
it isn't British, nor is it funny. We come across it quite
often here and it's a very, very painful business.
There are diseases of the digestive system which also
relate to overweight. Cirrhosis stalks more overweight
men (usually "drinking" men) while gall stones more
often trouble women, in line with the old medical cliché:
"female, fat and forty."
Every surgeon who must slice through layers of fat
tissue knows the added vulnerability and the poorer
prognosis of the obese patient. In addition, women who
are seriously overweight have difficulty conceiving and
also give birth to fewer live or healthy babies. Which
should explain your obstetrician's insistence upon a strict
diet in pregnancy.
There are many minor ailments, too, which are
worsened by obesity though they are not related to it—
hernia, for instance, or arthritis of the knees. You may
have watched some elderly, obese woman trying to cross
the street. She can't step down directly, but must stoop
and turn sideways. Slowly and unsteadily she lifts one
foot off, then, with a sigh, gets the other to follow. Losing weight wouldn't cure the arthritis of this poor soul,
but it would help her get around a lot better, with less
strain on her swollen joints.
You may not yet accept our say-so for all the suffering
and danger overweight carries with it. What statistical
validity is there to this dire prognosticating? Figures can
be construed into a lie when somebody is out to sell a bill
of goods. When they are simple arithmetic of addition
and percentages, gotten up by a disinterested agency,
they are worth heeding. The vital statistics offered below
are brutal, but terribly convincing.
This material, derived from a very recent publication
of the Metropolitan Life Insurance Company (1960), is
based on a survey, "Build and Blood Pressure Study,"
made by the Society of Actuaries. The study covers mor40
TABLE II
"BEST" WEIGHTS FOR MEN AND WOMEN
According to Height and Frame—Ages 25 and Over
Weight in Pounds (In Indoor Clothing)
MEN
Height
(In Shoes)
5' 2"
3"
4"
5"
6"
! '■ '
8"
9"
10"
11"
6' 0"
1"
2"
3"
4"
Small Frame
Medium Frame
112-120
115-123
118-126
121-129
124-133
128-137
132-141
136-145
140-150
144-154
148-158
152-162
156-167
160-171
164-175
118-129
121-133
124-136
127-139
130-143
134-147
138-152
142-156
146-160
150-165
154-170
158-175
162-180
167-185
172-190
Large Frame
126-141
129-144
132-148
135-152
138-156
142-161
147-166
151-170
155-174
159-179
164-184
168-189
173-194
178-199
182-204
WOMEN
4' 10"
11"
5' 0"
1"
2"
3"
4"
5"
6"
7"
8"
9"
10"
11"
6' 0"
92- 98
94-101
96-104
99-107
102-110
105-113
108-116
111-119
114-123
118-127
122-131
126-135
130-140
134-144
138-148
96-107
98-110
101-113
104-116
107-119
110-122
113-126
116-130
120-135
124-139
128-143
132-147
136-151
140-155
144-159
104-119
106-122
109-125
112-128
115-131
118-134
121-138
125-142
129-146
133-150
137-154
141-158
145-163
149-168
153-173
Source: Build and Blood Pressure Study, Society of Actuaries,
Chicago (1959).
41
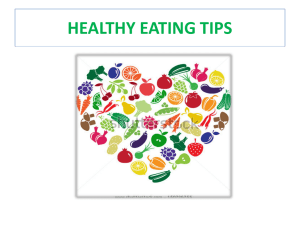
GRAPH I
TOO MANY PEOPLE ARE OVERWEIGHT
Proportion Exceeding Best Weight
By 10% or more
By 20% or more
Age
When
Insured
MEN
31%
20-29
53%
30-39
60%
12%
25%
32%
40-49
63%
34%
50-59
WOMEN
23%
41%
59%
67%
20-29
30-39
40-49
50-59
12%
25%
40%
46%
Best weight is slight or moderate underweight,
ranging from about 5-10% below average weight at age
30 to about 10-15% below at ages 45 and over.
Source: Metropolitan Life Insurance Company.
42
tality records of nearly six million insured persons in
twenty-six American and Canadian life insurance companies over the period 1935-1953. Again we urge you to
examine the graphs and we shall try to help with their
elucidation.
In the opening chapter you were asked to check your
weight against Table I of average weights, with a reminder that the American norm is well above a desirable
weight level. Look now at Table II of best weights and
see how you compare. The best weight is simply the
optimum weight at which fewest persons are stricken by
the various diseases afflicting all of us.
Graph I, which shows the proportion of men and
women exceeding their best weight, gives a truer picture
of their health prospects. Where only 1 man in 5 and 1
woman in 4 are considered 10% or more above average
weight, the percentage of overweight persons soars when
they are compared by best weight standards.
In their twenties, almost 1 man in 3 and 1 woman in 4
are already 10% or more overweight, the number rising
sharply at each age level for both sexes. A similar rise is
shown for the 20% or more overweights. Thus, over a
third of our people past 40 are seen to be obese, an
alarming indication and a warning signal to America.
Of the sexes, the ladies appear better-behaved, in their
diet at least, up to the age of indiscretion (40). Once over
the breach, their overweight grows scandalously, far
outstripping the men. The cause, as was suggested
earlier, was letting down their guard from sheer "battle
fatigue," to which might be added the different tempos of
the middle years. With the children now off to school or
away from home, there comes time for canasta, socials,
luncheons and such—and soon the dress size changes.
The dreadful meaning and consequences of Graph I are
made clear at a glance by Graph II, showing excess
mortality at different weight levels for each sex. By
excess is meant the death rate above that of standard risks
at average weights. Notice how the mortality rises
43
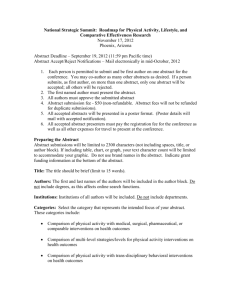
GRAPH n
OVERWEIGHT SHORTENS LIFE
Excess Mortality*
MEN
10% overweight
WOMEN
13%
20% overweight
30% overweight
`9%
25%
21%
42%
30%
Excess Mortality Due Chiefly to Heart and
Circulatory Diseases
Excess* for Principal Diseases Among Persons
About 20% or More Overweight
Heart disease
Cerebral hemorrhage
Malignant neoplasms
Diabetes
Digestive system diseases
(gall stones, cirrhosis, etc.)
Men
43%
53%
16%
133%
68%
Women
51%
29%
13%
83%
39%
* Compared with mortality of Standard risks (Mortality ratio of
Standard risks = 100%).
Source: Metropolitan Life Insurance Company.
almost proportionately to the weight rise, with a sad
bonus for the male side.
Several points should be made. First, that if the mortality comparison were made with persons at the "best"
weight level, the "excess" mortality would be several
times as great. Also, that the findings are, if anything,
greatly understated, since the insurees and especially
the very obese, are subject to careful selection, with the
rejection of all persons having a disease "beyond a minor
impairment."
44
Below the graph are given the death rates for obese
persons due to heart and circulatory diseases. It makes as
painful reading as any battle casualty list. (How many of
us have lost loved ones to these killers?) Remember that
the percentages do not represent total death statistics.
Nor do they compare the sexes, except indirectly. They
show only the overweight death rate excess of each sex,
respectively, above the standard risk for the disease in
each sex.
In general, women sustain their overweight far better
than men, we do not quite know why. It may be due in
part to their keeping closer to best weight levels in their
earlier years. However, while they suffer only half as
many heart casualties as the male, their overweight excess above average-weight women is a high 51%. Worth
comment, too, is the inordinately great excess of diabetic
mortality. Diabetes accounts for but a small proportion of
the death total, yet it takes a vicious toll of the overweight, and particularly among men.
But there is a happy ending for you in this melancholy
story. If you have been persuaded to reduce your weight,
you may yet be wondering: Is it perhaps too late? Can
weight reduction at any time of life stave off the effects
of these maladies and enhance your prospects? Graph III
brings good news which echoes the leitmotif of this
book.
It charts the progress of overweight policy holders,
charged above-standard rates, who reduced in order to
requalify as standard risks. Notice that the moderately
overweight cut their death rate excess by 19%. The gain
would have been greater had all these well-intentioned
people maintained their reduced weight.
For the markedly obese, the death rate plunged amazingly from 151% excess down to below the norm—
showing what a good scare, perhaps, plus self-discipline
can accomplish. (We might add an aside for those among
us who are less concerned with mere survival than with
getting around, being able to function, that the killing
diseases can also cripple, sometimes long years before.)
45
GRAPH III
WEIGHT REDUCTION BENEFITS THE OVERWEIGHT
Comparison of Overweight Men Who Reduced with General
Experience of Overweight Men of Similar Degree
Degree of Overweight
When Insured
Mortality Ratio
(Ratio of all Standard
risks = 100%)
MODERATE (Averaging 25%)
109%
Reduced Weight Cases
All Cases
128%
MARKED (Averaging 35-40%)
Reduced Weight Cases
All Cases
96%
151%
The information on overweights who reduced is based on those
originally rated Substandard because of weight only, but who later
qualified for Standard insurance. The experience covers the period
since the removal of the rating.
Source: Metropolitan Life Insurance Company.
We presume that by now most readers have decided
upon a reducing program. If you have any medical problem, you will of course let your doctor diagnose it and
prescribe for you. But should you not also be equipped
to recognize the existence of the problem? You have
already been given a brief description of the common
disorders associated with obesity. It will not hurt, in
addition, for you to learn some of the danger signals, as
well as know something about the testing procedures.
We hope you will not, like some suggestible medical
46
students, adopt in turn each set of symptoms and make
them your own. And we should warn you against using
the tid-bits of Materia Medica in these thumb-nail
sketches to doctor yourself. Or else, paraphrasing the old
saw about lawyers, "you will have a darn fool for a
doctor and a bigger one for the patient."
You and your doctor will first want to rule out constitutional defects having their origin in the glands. The
two glands most involved are the vitally important thyroid and pituitary.
Among the functions of the thyroid is making the
hormone thyroxin containing iodine which regulates the
rate of food metabolism. Where there is an insufficiency
of hormone, we have a condition known as hypothyroidism, which can vary from the mild to a severe myxedema.
Hypothyroidism manifests itself in a slackening of
mental activity, a dry, coarse skin and a lessening of
sexual function. There are, inevitably, the layers of firm
fatty tissue under the skin. The diagnosis is easily made
and the treatment is usually effective and quite dramatic.
Brief mention was made elsewhere of the BMR and
other tests of basal metabolism. The BMR is a breathing
test which determines the rate at which we consume
oxygen in burning food. We can then calculate the number of calories per day required by the patient at rest.
This test, however, can become quite inaccurate because
of emotional reaction. It isn't easy to have a mask placed
over the face, or to hold a plastic something in your
mouth, with the nose clamped shut, and then follow the
directions to breathe calmly and evenly, as if relaxed.
The new PBI, or Protein-Bound Iodine test is much
simpler for the patient and has increasingly replaced the
BMR. This is a blood test which likewise determines
thyroid activity. A third test is the Iodine Uptake, more
exact, but not needed in the average case.
The pituitary gland is the tiny (.6 of a gram) director
of the entire glandular system. Through its secretions it
greatly affects our size and shape as well as sexuality.
47
Its malfunctioning may result in hypopituitarism, with
adiposity as an outstanding symptom. In the adult, the fat
is distributed throughout the body, while in children it
usually has a feminine distribution, with fullness of the
breasts, hips, thighs and lower abdomen. The grown
male shows a sparsity of the beard and axillary hair, and
the pubic hair similarly has a feminine distribution. As in
hypothyroidism, there may be mental backwardness.
We find various clinical types among its victims, of
which the most unmistakable are the Brissaud and the
Fröhlich syndromes. The Brissaud type is fat, chubbyfaced, sleepy and lazy, much like Dickens' character,
"Fat Boy."
The Fröhlich type is seen usually in children and
young adults and is characterized by large hips and
abdomen, stunted skeletal growth and small genitalia.
There is also found a loss of the secondary sexual characteristics such as hair distribution, voice change and
muscle development.
There exist other nervous and glandular conditions
which show themselves through obesity, but they are
comparatively rare. To repeat an earlier statistic, not
more than 5% of cases can be traced to the glands. Most
of us, therefore, can safely make our own diagnosis of
our overweight as due simply to wrong eating or overfeeding.
Many obese are at the same time severely anemic. In
such cases, a CBC, or Complete Blood Count, is called
for. Such persons usually complain of shortness of
breath and poor circulation and are prone to skin eruptions. They are also often poor eaters. That is, they eat
poorly of everything, like certain children, except sweets
and rich desserts.
The onset of diabetes is usually gradual and the early
symptoms so mild, the diagnosis is not made until a test
for sugar is given. The potential diabetic should look out
for excessive thirst and hunger, frequent and copious
urination, weakness and unexplainable loss of weight.
The FBS, or Fasting Blood Sugar test, is an aid to
48
diagnosis (usually the blood holds 80-120 mg. per 100
c.c). A more informative test is the Glucose Tolerance
test by means of which we learn how the body utilizes
its carbohydrates. A measured quantity of glucose is
taken by mouth and then blood is withdrawn at intervals
to discover how much glucose remains in the
circulation. The results, when plotted on a graph, are
very helpful ia diagnosing not only diabetes, but liver
and pancreatic disease and other disorders.
A word on insulin, whose inadequate supply by the
pancreas produces diabetes. When it was first
discovered in 1922, insulin became life saving for the
diabetic. It has since been mostly replaced by the
development of the anti-diabetic medicines (Orinase,
Diabinese, DBI). But diet and weight reduction remain
the essentials in the treatment of this disease.
In gout, the joints become inflamed. A severe (arthritic) pain involves usually the great toe, but other joints
as well, and the arthritis may become chronic and deforming. It is much more manifest in the male and usually shows its ugly effects in midlife. The diagnosis is
determined by a blood test showing the level of uric
acid (normal is 3-5 mg. per 100 c.c.).
Coronary disease may be first recognized, by a pressure on the chest or a feeling of overwhelming weight
there, or a "squeezing pain" under the breastbone, felt
more sharply after any exertion. There may also be
symptoms of profuse sweating, weakness and fainting
spells. This occurs when the arteries encircling the heart
muscle become narrowed or obliterated and the heart
muscle cannot function properly because it does not get
adequate nourishment or oxygen supply.
Since the heart blood vessels are "end arteries," with
no interconnections, any permanent blockage results in
damage to the heart muscle. The resulting scar tissue
cannot conduct an electric current and can therefore be
assessed by an electrocardiograph. Defects in the patterns of the electrical waves pinpoint the defective tissue
for proper diagnosis.
49
A stroke (apoplexy) is characterized by blood vessel
damage within the brain which can result in either a
transient or permanent paralysis, depending upon the
brain area. The attack is sudden and often quite unexpected, unless the victim has been warned about his
pressure. The doctor, himself, when confronted by an
unconscious patient who could be suffering from drug
poisoning, diabetic coma, alcoholism, etc., may have to
call upon a bit of clinical acumen to make his diagnosis.
We come, finally, to the controversial subject of
cholesterol. Let us seek some clarification.
So many patients nowadays, not all of them overweight, ask the doctor: "Do you think I need a cholesterol test?" Such testing is easy and harmless and may
reassure you. (The normal level in the blood is 150-240
mg. per 100 c.c.). But, let your doctor decide.
Cholesterol has become a scare word, yet it isn't all
menace by any means. Though an excess in the blood
stream may be a danger sign, this fat-like substance is
found in many valuable foods and is a vital constituent
of your body tissue where it is widely distributed in
fundamental organs.
We hear a great deal about saturated versus unsaturated (and poly-unsaturated) fats; what is it all about? In
a later chapter on Food Chemistry, we shall analyze fats
and saturation. Here it should suffice to say that
saturated fats are mostly meat and dairy fats which
remain solid at room temperature. While the unsaturated, containing vegetable and marine (fish) oils, usually stay liquid. There are, however, hydrogenated
(solidified) margarines which can be mostly unsaturated
if they are made from vegetable oils. (Read the wrapper.)
It is now generally accepted that diets high in saturated fats increase the blood cholesterol and blood fat
levels, whereas the unsaturated fats and oils either do
not affect them, or actually lower the levels. What is
disputed is the extent of their contributory effect on
50
arteriosclerosis and heart disease. You may find interesting a capsule history of the extensive, if recent, research
and experimentation which have led to our present
thinking on the subject.
Years ago it was believed that arterial deterioration
was a result of constant usage and that arteriosclerosis
were merely the toll taken by age. Then we learned it
can also be brought about by high blood pressure,
diabetes and gout. Only recently have we come to think
that it can be produced by the diet as a result of a faulty
metabolism of fats, especially of cholesterol.
This metabolic theory is bolstered by experiments
with animals in which arteriosclerotic changes have
been brought about by feeding them excessive fats and
cholesterol. Whether this holds true also for humans is
not yet known.
A great number of studies have led step by step to the
conclusions of the advocates of unsaturated fats.
Isidore Snapper, in "Chinese Lessons to Western
Medicine," was the first to suggest a correlation between
diet and arteriosclerosis. The low incidence of heart
disease among the Northern Chinese was related by him
to their diet of vegetable and fish oils.
L. S. Kinsell corroborated this view in a study that
showed a marked decrease in blood cholesterol levels by
the intake of vegetable oils. There thus developed the
concept of differences in fats, determined by the degree
of saturation.
A later study by B. Bronte-Stewart compared the
effects of saturated and unsaturated fats upon Zulus and
Europeans by an interchange of their diets. The Zulus,
who normally lived on a diet almost free of saturated
animal and dairy fats, and who had low blood
cholesterol and blood fats, developed higher levels on
the Western diet. Whereas the Europeans, ill with coronary disease, were reported to have experienced a drop
in their levels when fed the unsaturated Zulu diet, along
with a mitigation of their disease symptoms.
Ancel Keyes and his associates have made the great51
est contribution by their investigation of correlations between diet and vital statistics in about a score of countries. He discovered, for instance, that the natives of
Japan whose fat intake is composed exclusively of
marine oils derived from fish have, no coronary disease.
A related study of Japanese men in Japan, Hawaii and
in California, matched by age, weight and type of work,
showed a rise in cholesterol levels from 127 mg. in
Japan to 178 mg. in Hawaii, to 206 mg. in California, in
almost exact correspondence to the half-way American
diet in Hawaii, and the complete change-over among the
acculturated Japanese-Americans. With the dietary
change was revealed an increased tendency to coronary
disease.
A comparison of low-coronary Italy with England
which comes close to our own rate—the highest in the
world—gave further support to the theory. The last link
needed to relate saturated fats to heart disease was the
repeated finding of the atheromatous (fatty) plaques of
arteriosclerosis in the blood vessels of coronary victims.
In a series of other studies among different races and
groups, the incidence of high blood cholesterol and fats
in the body seemed roughly to parallel the statistical
incidence of heart disease.
One more elaboration of the theory and we shall conclude. Keyes believes that the high blood fats are also
instrumental in increasing the blood coaguability, thickening it so as to impede the clearing away of clots. This
leads, he thinks, to the formation of massive clots and to
thrombosis. He therefore argues for the substitution of
vegetable and marine (fish) oils, claiming that these are
more soluble and thereby lessen the possibility of not
only thrombosis, but of arteriosclerosis and heart
disease.
In summary, the proponents of the "cholesterol
theory" urge the substitution of fish for all meat dishes
and the total elimination of butter, cream and whole
milk from the diet, with fatless dairy substitutes. They
tend to label their opposition as die-hard conservatives.
52
It is a historic truth that each significant advance made
in science, from Galileo to Einstein, from Pasteur to
Salk—met with apathy or hostility before its universal
acceptance. Yet important men of research, among them
Frederick Stare of Harvard and Irvine Page of The
Cleveland Clinic, feel that any definitive conclusions on
cholesterol are as yet premature.
There are still questions to be answered. Is not cholesterol manufactured in the liver as well as taken in as
food? And why do many persons with normal levels
have arteriosclerosis or fall victim to heart disease?
Should we then revise our concept of "norm"? And what
of the fluctuations in the same individual at different
times as in diarrhea? For instance, we find a fall in
anemia and in acute infections and a rise in diabetes and
pregnancy.
What does medical common sense suggest, since the
purpose of this book is to give voice to it? The middleof-the-road medical consensus is well expressed by a
finding of a Rockefeller Group study: "It seems inadvisable at this time to ask the general public to eat more
or less fat of a particular kind . . . but it is reasonable to
act on an unproved hypothesis if the risk of doing so is
not great." (They make an exception for the lean person
who has no problem maintaining his weight.)
Further research is in progress and we shall watch it
carefully. In the meantime, weight control combined
with a limitation of saturated fats seems prudent, preventive and harmless. Certainly, for overweights, particularly if there is some family predisposition to heart
disease, such precaution is highly advisable. For this
reason, the high-protein diet we shall outline cuts down
sharply on saturated fats. We shall also suggest some
substitution of fish for the fatty meats which together
with starches preponderate in the diet of the obese. In
any case, since fats are high-caloric, limiting them will
help reduce overweight.
It is hoped that this rather technical chapter has given
you some small insight into the many medical problems
53
associated with obesity. We did not wish to instill fear
but rather an understanding of an existing menace. We
do wish to strengthen your resolution to keep yourself
nourished and slim enough to enjoy a longer and healthier life.
54
Chapter IV
NUTRITION—WHAT'S IN AN EGG?
were asked what is inside an egg, you might
think of the "which came first?" riddle and answer "a
chicken."
The question involved food values, yet you would not
be far off base. The egg does contain that chemical
combination in nature which holds the mystery of life
and needs but a fertilizing spark to vivify it. What is the
living stuff found in every egg from the single-celled
ovum to that of the ostrich or dinosaur? It is, of course,
protein.
This protein determines the body structure of the
growing organism and provides all its tissues and
organs. But to stay alive and develop, it needs heat and
energy which must also be found inside the egg. There
are two food sources for heat-energy, fat and
carbohydrate— which does the egg hold? Does it also
have vitamins, like the kind we grow in bottles?
Minerals such as we dig for underground?
The egg chose fat for its energy source and does
contain these other materials in varying quantities. It is
very nearly a perfect food—which makes the laid eggs
of certain species highly desirable for others. There
exist, we have learned, at least sixty nutrients and a perfect
food offering all of these could sustain life. The milk
manufactured in the female animal body is such a food.
Many millennia ago, long before biblical Goshen was
55
IF YOU
known as a land of milk and honey, men learned to domesticate animals so they could share the mother's milk
of the cow, goat, mare and other quadrupeds.
When a biochemist analyzes milk he learns the exact
proportions of all its constituent elements. The average
adult is urged to drink a pint daily. What is he taking into
his body? The food chart would read something like this:
Food ......................
milk
Quantity ................
1 pint
Calories..................
330
Food values
Protein ............... 17 grams
Fat ..................... 19 grams
Carbohydrate... 24 grams
Vitamins
A........................ 780 I.U.
D ........................
25 I.U.
C ........................
9 mg.
Thiamine ............ 0.18 mg.
Riboflavin .......... 0.84 mg.
Niacin ................. 4.6 mg.
Pyridoxine .......... 0.3 mg.
Biotin ................. 25 mg.
Choline ............... 70 mg.
Minerals
Calcium .............. 590 mg.
Phosphorus ........ 460 mg.
Iron .................... 0.35 mg.
Sodium ............... 250 mg.
Potassium........... 800 mg.
Magnesium ........ 70 mg.
Copper ............... 0.1 mg.
Sulphur .............. 145 mg.
Chlorides ............ 490 mg.
Words like vitamin and protein have become household currency—what do they mean? How do they and
other nutrients serve the human? How is each handled by
the body mechanism? And what results from an
oversupply or, more likely, from any deficiency? We
shall try to squeeze into these next chapters a brief
primer in food chemistry and some basic physiology.
56
They ought to awaken memories of school studies and
reveal new facets in that daily commonplace: the food
we eat.
Such a presentation in a book on diet is intended to
serve a two-fold purpose. It should teach you to measure
your honest dollar against true food values. You will,
perhaps, learn to look beneath the gay packaging of the
breakfast cereal "Nix" or "Crash," which promises (on
its sugared, high caloric and almost nutritionless chips,
pellets or flakes) to raise stalwart supermen.
You will come to see right through the expensive
marbled sirloin and chose a lean steak or an organ meat.
You may peek inside the giant vitamin-mineral capsule
which, you pray, will expiate the nutritional sins you
have committed against your defenseless body. And you
will eventually recognize the flaws in food faddism,
including reducing fads such as the recent safflower
silliness and the new-rage 900 calorie diet.
Even more valuable is knowing what happens to food
inside your body. If wrong eating is as responsible for
obesity as overeating is, then the composition of your
diet is of equal importance to the quantity. You will be
equipped to choose your foods for their specific contribution to a balanced diet. And as an overweight, you
will have learned, we trust, how to blend that proportion
of protein, fat and carbohydrate in a high-protein diet
which will help you reduce and will later maintain your
normal weight for optimum health.
Take a single bite of a meat sandwich and the wondrous body mechanism of many wheels within wheels is
set in motion. As the teeth pulverize the food, enzymes
in the saliva attack the bread starch to convert it into
complex sugars. This digestion process is partially continued in the stomach where the food is ground into a
mash, liquefied and acted upon by gastric juices.
However, the major work of digestion and absorption
takes place in the misnamed small intestine—a 20 to 30
foot pipe line. Here the liver and pancreas each pour in
57
up to a quart and a half of fluids daily to process the
food. The resulting products are then taken into the blood
stream to be distributed throughout the body. After a last
gleaning in the large intestine, the solid wastes and the
undigested debris are forced into the bowel for excretion.
All this tremendous activity, so sketchily presented
here, is gone through to produce body heat and energy,
but also to replace the tissue wear and tear by furnishing
fresh materials for reconstruction. Protein foods are the
only source of building materials for body replacement;
carbohydrates and fats both serve as body fuels. The
efficiency of the human machine, output measured
against intake, depends upon the proper balance of
nutritive elements in the diet.
CARBOHYDRATES
Let us start with the carbohydrates, universally present
in all plant life as fruits, vegetables and the cereal grains.
Carbohydrate is another name for foodstuffs containing
sugar or starch. We shall ask you to cut these to a
minimum, but that minimum must be there.
When they are burned in your body, their metabolism
releases the heat and energy needed for it to perform.
The heat is internal, permitting life functions to go on.
The energy in the form of glucose (blood sugar) is essential for the operation of your vital organs such as the
glands and brain, and for instantaneous muscle action
involving every movement you make.
The rate of this metabolism, as was mentioned elsewhere, is measured by the amount of oxygen the body
uses up in the burning of food. Your basal metabolism is
your fasting, at-rest rate. The heat liberated by a food in
the body is expressed in calories (heat units). Every food,
then, can be considered as a potential fuel containing a
certain number of calories. For the overweight, the
caloric value of a food is of great concern, since an
58
unburned calorie surplus can be converted by the body
into fat.
The key, therefore, to any weight reducing program is
creating a "calorie deficit" which will compel the body
to surrender its stored fat for burning. Calories do count
then, but don't count them. What is wrong with calorie
counting is that it so totally ignores the other nutritional
values of the food. The only food that gives nothing but
heat is pure, refined sugar, empty calories. The natural
foods containing sugars and starches offer in addition
valuable vitamins, fat and even protein.
Sugar is found in all fruits and vegetables in the form
of fructose (fruit sugar), sucrose (table sugar) and in
milk as lactose (milk sugar). These are readily absorbed
and made instantly available as glucose for muscle action. Starches must first be processed before they can be
utilized in the bloodstream. The processing is a lot like
the "cracking" of crude oil to obtain gasoline.
Let us sort out that meat sandwich bite, starting with
its bread. It is mostly starch, like all breadstuffs and
cereal products, but fruits and vegetables as well are
essentially starch foods. In a reducing diet you should
choose those starches which offer the greatest bulk and
the highest nutritional values at the lowest calorie cost.
When the glucose level in the blood becomes too high,
the surplus sugar is converted into glycogen and stored
in the liver and muscles. However, the liver can hold
only 50-60 grams of glycogen. The excess, obtained
through overeating and underactivity, is eventually
turned into body fat.
Normally, from 80-120 mg. per 100 c.c. of glucose is
always circulating in the blood. When the blood sugar
falls below this level, the liver responds by reconverting
some of its glycogen into glucose. It thus regulates the
blood sugar concentration, with the aid of insulin produced by the pancreas (plus other complicated mechanisms. )
While some carbohydrate is constantly needed, a little
is enough. Consider an average American breakfast of59
fering fruit or juice, cereal, breadstuff, perhaps with jam,
and coffee. With almost no protein or fat (from meat,
egg or milk) to slow down the digestion, there is a rapid
rise in the blood sugar (usually added to by refined sugar
in the cereal and coffee.) The pancreas is now stimulated
to pour forth insulin. At the same time the liver is
activated into withdrawing glucose to store it or, if
already well-provided, to convert it into fat. The
resulting irony of excessive sugar intake is a sharp drop
in the blood sugar level, with more or less grave consequences.
You may have experienced in the course of a day,
after such a breakfast, the mental lassitude and physical
fatigue, the slackening in work tempo, which come from
blood sugar inadequacy. If your lunch, plus candy nibbling or a coffee break, responding to the pangs of
chemical hunger, and perhaps even dinner, should offer
the same high proportion of carbohydrates, the glucose
pancreas-liver interplay could become increasingly
hectic and even disastrous.
A great insufficiency of blood sugar can bring on a
loss in muscle tone, subnormal temperature, at times
convulsions. At a very low glucose level, as in insulin
shock, there is a drop in blood pressure, loss of consciousness and possibly death.
This is not meant to scare you into eliminating carbohydrates from your meals, as a certain High-Fat dietist
seems to advocate. If you did, these same symptoms
would occur, though in lesser degree. We must have an
energy source instantly available when called upon.
Enough carbohydrate should be eaten to keep the blood
sugar level normal and readily replenished.
Another result of glucose insufficiency is the incomplete burning of fat. You may have been close to a child
ill and running high fever, thereby rapidly consuming all
its blood sugar. There is a peculiar odor to the breath,
like the smell of over-ripe apples. This is acetone produced by the body attempting to burn fat in the absence
of sugar.
60
It is medically well-known that a fat has to "burn in the
fire of a carbohydrate." Just as we cannot start a coal fire
by putting a match to it, but have to have a wood fire
going first. The feverish child has exhausted not only the
sugar in the blood but the stored glycogen as well and,
unable to take nourishment, is now trying to burn its fat.
The acetone and other dangerous acids formed by this
incomplete oxidation can lead to lethargy and coma.
Where there is a slow but persistent depletion of
carbohydrate as in starvation or in weight reduction, that
remarkable organ, the liver, helps itself by producing
glucose from fat in the body and also from protein tissue.
Shrunken skin, haggard and wrinkled faces are the result.
The aim of every reducing diet should be to compel the
body to draw upon its stored fat rather than its body
structure. The high-protein diet, instantly repairing any
destruction, will preserve your valuable tissues as well as
your appearance.
A final word on hidden calories. Too much of our carbohydrate intake is in calories lurking m soft drinks, each
glass holding a probable tablespoon of refined sugar, in
our jams, jellies and fruits canned in sugar, not to
mention high-caloric alcohol (the third or fourth nonmention). We are also being deluged with poor starch
foods (disguised sugars) such as refined breakfast cereals
and breadstuffs, from which most of the vitamins have
been milled out.
We can and should obtain all the carbohydrate we
need from fresh fruits and vegetables, and from whole
wheat bread and the whole grain cereals. A substantial
adjustment in our shopping patterns and menus is called
for. We shall be more specific in later chapters.
FATS
In the meat sandwich, the bread was made more palatable by "real" butter or perhaps by a pat of margarine
61
of equal caloric value. Fats are, like carbohydrates, an
energy source and like them are carriers of vitamins—
highly essential vitamins A, D and E are soluble only in
fat. So here again, as with carbohydrates, a reducing diet
which necessarily cuts down sharply on fats must nevertheless allow for a safe margin of fat intake.
They are eaten as animal fats in meat, fowl, eggs and
fish, as dairy fats in milk, butter, cream and cheese, as
vegetable fats in nuts, and margarine, and in olive, corn,
soybean and cottonseed oils. They are easily used and
almost totally absorbed, while excess starches have a
tendency to ferment in the large intestine and produce
gassiness.
Fat is a highly concentrated food with comparatively
little bulk and twice the caloric value of equivalent
carbohydrate. That pat of butter or margarine doubled the
metabolic effect of the slice of bread. Similarly, a baked
potato will have its calories doubled by the butter coming
with it. As against the larger bulk of carbohydrates, often
swollen in cooking like macaroni, the fats give a greater
feeling of satiety, have more staying power, particularly
for the hard-working individual.
The final choice between these two fuels, since the
overweight must often make the choice, is a matter of
taste. Certainly, some fat is indispensable to cookery but
should be used sparingly. In any case, since fat is found
widely distributed in protein foods, even in lean meat
(15%) and in skim milk, a fat deficiency on a high protein
diet is unlikely.
As for overeating of fat, common among overweights,
the results are painfully apparent. This fat in our arms,
thighs and abdomen, where did it come from? What does
it consist of? Body fat is manufactured by the liver mostly
from excess carbohydrate, but it also comes in part
directly from the fat we take in as food.
It has been shown experimentally that certain fats such
as mutton have appeared unchanged in the fat depots of
the body. The body fat had the same chemical
62
characteristics (number of double carbon bonds) and the
same melting point. While the conversion of sugar into
fat is less clearly understood, because we cannot
duplicate it in a test tube, we do know that the process
goes on. Most obese people deposit more fat than could
be derived from the fat they have eaten.
Fat normally makes up 12% of our body weight,
mainly in adipose tissue which is about 90% fat. The
adipose is in a semi-liquid state and is held together by a
sponge-like structure of connective tissue. This fat is not
all reserve energy. Some is required in various tissues to
maintain health. For example, the brain, lung, spleen and
heart fat is not lost even in starvation. The individual
body cells likewise contain fatty components; in the skin
protective fat enhances the appearance—particularly in
countries where the feminine plump is still pleasing.
Fats, chemically speaking, are combinations of fatty
acids with such substances as glycerine and choline (a B
vitamin). They are not soluble in water and may be
divided into phospholipids (lecithin), sterols (cholesterol) and neutral fats which constitute almost all our
adipose tissue. Food likewise contains mainly neutral
fats. These can be further subdivided into saturated and
unsaturated fats.
Recently, animal and dairy fats have become taboo;
butter is poison. And perhaps the taboo is too rigorous
and tinged with emotionality. The reason for their rejection is the growing preoccupation with the cholesterol
content of the blood (discussed in the preceding chapter).
The level has been shown to rise after eating saturated
fats and is either unaffected or can be lowered by unsaturated and poly-unsaturated fats. What is the chemical
nature of this saturation?
Atoms of any substance may link with one another to
form a compound, held together by an electric force. The
following diagram shows the configuration of a fat
molecule:
63
H H H
R—C—C—C—R
I I IH
H H
R stands for a chemical chain of atoms.
C
for the carbon atom.
H
for hydrogen.
We have here a complex chemical substance showing
3 carbon atoms. Each C atom in a fat molecule must
have 4 connecting lines or bonds. When all these bonds
are satisfied, because they link the G to another atom, we
call it saturation-found in meat and dairy fats.
If the formula were to read like this:
H H H
I I
I
R_C=C—C—R
H
We would have a pair of C atoms connected by 1
double bond. This represents an unsaturated fat as in
olive oil.
Finally, if the formula had more than 1 double bond,
we would have a poly-unsaturated fat, having the greatest anti-cholesterol effect as in fish oils and in most of
the vegetable oils.
H H H
I I I
R—C=C—C=R
What to do about saturation? While it is true that
beef and lamb fats are about half in saturated form,
there is no escape from eating some. Egg fat, which in
various guises is eaten almost daily, is highly saturated;
fowl is less saturated than beef; fish and other sea food
has only 15-25% of saturation.
We therefore repeat an earlier admonition. It would
seem advisable for most persons, and especially the
64
obese, to give fowl and particularly fish foods a more
prominent place in their protein diet. And one egg a day,
with a wary eye for commercial eggy cakes, crackers
and noodles, should suffice any adult.
As for the dairy fats, we favor the substitution, as far
as is feasible, of skim milk for whole milk (by the
adult), cottage cheese for the fattier varieties, and of
vegetable oils such as corn, cottonseed and soy oil, all of
them poly-unsaturated, for the butterfat used in cookery.
When it comes to butter for table use, as against certain
liquid oil margarine spreads, let palatability and
discretion guide you.
A final thought about that remarkable organ, the liver,
holding a note of reassurance on cholesterol. Not only
can it produce fat from glucose but it has other mechanisms for the juggling of fat. Fat is brought to it in food
as well as from the adipose depots. The liver can prepare
the fat for burning—but it has also been shown capable
of changing fat from a saturated into an unsaturated
form.
Our advertising agencies are promoting synthetic
vegetable fats which almost but not quite claim to ward
off or cure heart disease, hardening of the arteries, old
age, and whatever else you fear. The general public is
not aware that, though the vegetable oils make equally
good energy sources, they lack the essential vitamins A
and D carried by animal and dairy fats. It is therefore
highly desirable and the consumer should insist that
vegetable fats have these vitamins added—and not synthetic vitamins but the natural A and D found in cod
liver oil and other fish oils.
PROTEINS
The meat in that sandwich bite came from an animal
body which is mostly protein like our own: our skin,
muscles, internal organs, even the hair and nails. The
body in turn uses protein to manufacture its blood, the red
and white corpuscles, also its hormones and enzymes.
65
We are continually losing mucousy secretions; skin must.
be regularly replaced, tissues repaired. We are certainly a
complex and awe-inspiring creation. To be able to carry
on these remarkable functions, we have to have the
proper materials of high quality and in adequate supply.
Protein foods are therefore the prime essential of our
diet. It has been determined that we require about 70
grams of protein daily to replace the tissue losses incurred (Notice that protein is measured by weight rather
than calories). This may not sound like much—just 23
ounces—but in destitute nations the dreaded disease
Kwashiorkor is still prevalent among children. This condition, resulting from severe protein deficiency, is a
grave problem in Africa and in neighboring Central and
South America.
We in this country are fortunate. We don't have to
consider minimum requirements but rather ideal needs.
We are most of us able to afford high-grade protein. The
amount has been a subject of contention, but we believe
that the healthy adult can safely take and utilize 100
grams. In a high protein reducing diet we have successfully raised the daily intake to 125 and even 150 grams,
depending upon the overweight's level of activity. Obviously, an auto mechanic, who can get down a pound of
steak in the evening and a fish dinner for lunch, can
assimilate a lot more protein than the desk worker.
The quality of the protein is even more important than
the amount. Our digestive process breaks down protein
food into chemical combinations called amino acids.
There are twenty-two amino acids which serve our
tissues as building blocks for the thousands of
combinations they need.
Cells in the various organs differ in the amino acids
they have to find in the blood stream. All but eight of the
twenty-two can be produced by the cells from other
amino acids. These eight which cannot be synthesized
must be furnished in the diet for the maintenance of
health. They are therefore called the essential amino
acids.
66
A food protein is said to be of high biological value or
complete if it contains all the amino acids. A protein
lacking essential amino acids is incomplete, not a firstclass protein. Meat, eggs, fish, and milk with its derivatives, are all complete proteins rich in essential acids;
meat has the highest biological value of any food.
Vegetable proteins, including nuts and the germ of
cereals, lack essential acids and are therefore of lower
efficiency. The proteins of legumes, refined cereals and
milled flour have a very low biological value—they
cannot support life. Vegetarians over the centuries have
managed to survive on their diet for one physiological
reason. Two or more incomplete proteins, if eaten together, can be combined in the body to form the missing
essential acids. This takes a great deal of know-how
applied with the zeal of the true believer, or one falls a
victim to his self-deprivation. (Unless he cheats by eating milk and eggs or, as was widely rumored about that
sturdy vegetarian, Bernard Shaw, takes liver extract.)
Even for the meat eater, mixtures of different vegetables are better than any single vegetable protein,
though no. combination can equal the efficiency of a
complete protein like milk. In a well-balanced diet, a
proper blending of proteins sufficient for all body needs
is achieved. Whether or not you have a weight problem,
check for protein adequacy per meal per day.
We are indeed trying to influence your food habits,
without turning you into an Eskimo who can stash away
eight pounds of meat a day. You need have no fear of
taking in an excess. If a surplus is supplied to the body,
it is burned as fuel (which is why proteins, too, have a
calorie value). The advantage is that by substantially
exceeding the minimum you may be fulfilling your optimum requirement.
There is a high correlation between your health and
what is known medically as your nitrogen balance. The
protein amino acids have an NH2 constituent which,
when broken down in digestion, releases nitrogen. Protein (nitrogenous) substances are continually being lost
67
from the body in the stool and urine. The ratio between
the nitrogen intake from the amino acids and the nitrogen
loss is called the nitrogen balance. When intake exceeds
output, you are in positive balance. Your diet must
preserve this positive balance for good health.
Proteins were not always as well regarded in dietetics
as they are today. Not long ago, persons suffering from
Blight's disease or high blood pressure were advised
against eating eggs or meat which were thought to tax
the kidneys. We know today that the sick particularly
need an abundance of good protein. What may have
saved many in those days was that the recommended
milk solids were not then considered as the proteins they
are.
There are millions of Americans who can afford the
best proteins, yet stuff themselves oh the cheaper carbohydrates and fats. Too many older persons and young
children are found to suffer from a protein deficiency.
The protein requirements for a growing youngster have
never been determined. There is no such thing as too
much—and too little can cause a lowered resistance to
infection, pallor, easy fatigue and gastro-intestinal symptoms. A gram of preventive protein is worth a bottle of
pills.
There is a final advantage of protein over other foods:
its specific dynamic action. This is not scientific gobbledegook. All food entering the alimentary canal has a
stimulant effect on the metabolism, because digestion
requires a good deal of work (expends heat). Protein
stimulates the metabolism by about 20%, the effect lasting for three to four hours—as against only a 5%
increase for carbohydrates and fats. Thus, the protein we
eat consumes 15% more of its caloric value than do other
foods.
What does this mean for the high-protein reducing
diet? The phenomenon of specific dynamic action is another substantial argument for taking in an excess of
protein. If you are in the habit of estimating your
calories, you can allow a 20% markdown for the ex68
pended protein. In addition, the greater satiety we
noticed in fatty foods applies equally to many proteins.
Nothing sticks to the ribs better than a chunk of meat.
As for the objection raised against the high-protein
diet as being too expensive, there seems to be a confusion here between food values and market value, between high quality protein and a porterhouse. Liver,
truly a miracle food, and other organ meats are within
reach of the lowest budget. Fish in season or iced is
available even to inland communities at far lower prices
than beef (and has about half the calories.) Inexpensive
(skim) milk, eggs and (cottage) cheese can serve as a
base for your daily protein intake.
You don't drink milk, you say? You can't stand liver?
You find most fish dull, eggs and cottage cheese
insipid? Then you will inevitably have to compensate
for protein deficiencies with even more insipid and far
more costly food extracts, concentrates and
supplements. Or you can simply learn to like what is
good for you, made appetizing by the art of cookery.
There is no excuse for protein impoverishment in
America.
VITAMINS
To furnish the body with its energy and protein requirements is not enough. Accessory food factors are
equally necessary for normal health and growth, for life
itself. These are the vitamins and minerals. We shall
round out our discussion of nutrients by summarizing
the significant data about these two nutrient groups.
Vitamins are complex substances whose composition
is now pretty well established—with some remaining
gaps. By the grace of radio and television vitamins are
also well publicized. They are today multi-million dollar
big business, exerting a great influence upon our eating
habits.
One too frequently hears, "Oh, my diet is fine! I'm
taking vitamin pills. Do you think these are O.K.?"
Vitamins and minerals should be gotten where they
69
belong, in foods where they are naturally present and are
more easily absorbed by the body. I£ you eat the proper
foods in a well-balanced diet (a big "if," undeniably),
you probably need not take pills—unless your doctor
approves. Fortunately, any excess is detrimental only to
your purse, with the exception of vitamins A and D.
This section may prove a bit technical for sight reading and easy memorizing, but it is of general interest and
can serve for ready reference on this very vital phase of
your nutritional needs. The vitamins are divided into two
groups, the fat soluble and the water soluble.
Fat Soluble Vitamins:
Vitamin A—found in fats of animal origin such as
halibut and cod liver oils, liver and beef fats, eggs, milk
and its derivatives. It is not present in vegetable fats such
as olive oil and margarine. Yellow vegetables, though
they contain no vitamin A, are rich in carotene, a
substance the body can convert into this vitamin.
Its inadequacy predisposes the individual to infections.
It can produce night blindness and various changes in
the skin and mucous membranes. The skin appears dry,
scaly and prone to eruptions. The tear glands may stop
functioning so that the cornea, losing its moisture,
thickens and becomes diseased. This condition, called
Xerophthalmia, is curable (medically) by the same Vitamin A.
Lack of this vitamin also affects the intestinal tract, the
respiratory system and the central nervous system, either
causing or greatly contributing to a variety of disease
conditions. Before we were ever aware of the existence
of vitamins, cod liver oil was used in the treatment of
various diseases, including tuberculosis.
The vitamin A nutritional factor is therefore of utmost
importance in the body's resistance to disease, though its
lack may not be the sole contributory cause. You should
be able to satisfy your minimum requirement without
70
any supplements. Do not in any case be misled into
taking massive doses of vitamin A which can produce
severe toxic manifestations.
Vitamin D—found in fish liver oils, egg yolk and in
animal fats. It too is virtually absent from vegetable fats
and margarine. It can be made synthetically by the action of ultra-violet rays on ergosterol (a constituent of
yeast and ergot). Recent research has shown that vitamin
D is actually a composite of several closely related
chemical substances (of which the vitamin D2 from
ergosterol is only one). For this reason, in discussing fats
we urged that the vitamin D added to foods like
margarine should come from a natural source containing
the whole D group. Or you yourself can go to the food
source to be assured of adequacy.
Vitamin D promotes absorption of calcium and phosphorus and is very important for the proper development
of the teeth and bone structure. A deficiency produces
rickets, a disease of the infant and child characterized by
soft deformed bones, and osteomalacia, a disease of the
adult, resulting similarly in bone softening.
People have the feeling that if a little is valuable, a
great deal is a panacea. As with vitamin A, an excess
can cause severe body damage. Before the toxic effects
were known, arthritis was treated by massive doses of
150,000 units. Today, vitamin D cannot be sold in units
above 25,000 without a prescription.
Vitamin E—found in vegetable oils, wheat germ and
green leaves. It has been called the fertility vitamin
because it has been demonstrated as necessary for normal fetal development.
Vitamin K—the last of the fat soluble vitamins. It is
essential for blood to be able to clot normally and is
found naturally in cabbage, soy beans, egg yolk and
spinach. It can also be produced synthetically, and inside
the body by intestinal bacteria.
These four fat soluble vitamins are fairly stable substances which are not destroyed by the heat of cooking
or by the preparation of their foods. All other vitamins
71
are water soluble and include the B complex group, not
all of whose factors have yet been isolated.
The B Complex Vitamins:
These are found in liver and eggs and in whole grain
breads and cereals, where they are contained in the germ
and bran. Refined white breads and cereals offer very
little since most of the vitamins have been removed in
the milling. (There is a vitamin B complex sold in paste
form which is nothing more than rice polishings.) These
vitamins cannot be stored in the body as the fat-soluble
generally are, therefore they need to be replenished
daily.
If vitamin B complex is absent from the diet, normal
growth and tissue repair are interfered with. There is loss
of appetite, constipation, a slowing down of the progress
of food in the intestinal tract, fermentation and
putrefaction of retained food materials. There may also
result changes in the normal brain metabolism as well as
neuritis, damage to the heart and circulation—and more.
The B vitamins are crucial and are the ones most frequently found deficient in the diet even of persons able
to afford the best in food. They include:
Vitamin B1 (Thiamine), essential for proper utilization
of carbohydrate and for normal intestinal functioning. It
is the "appetite vitamin," is used to treat the disease
Beriberi, and is responsible for normal metabolism in the
brain.
Vitamin B2 (Riboflavin), necessary for growth. It prevents certain eye infections and is involved in tissue
respiration.
Niacin (Nicotinic Acid), the anti-Pellagra factor. Pellagra, still common in the south, is manifested by a
severe and characteristic skin rash, painful diarrhea and
mental disturbances.
Vitamin B6 (Pyridoxine), related to fatty acid and
protein metabolism. It is involved in antibody production indispensable in fighting infection.
72
Choline, a body growth factor, also related to fat
metabolism.
Pantothetic Acid, involved in protein metabolism as
well as in various enzyme processes.
Vitamin B12, which can increase the growth of physically retarded children. Its main use is in the treatment
of pernicious anemia, for which reason this condition is
no longer considered pernicious. It is also useful in the
treatment of neuritis.
Inositol, which increases gastro-intestinal motility
(peristalsis).
Biotin, a growth factor.
Para-aminobenzoic acid, essential for bacterial
metabolism. An effective medicine in certain infectious
diseases.
Folic Acid, essential for the metabolism of the bone
marrow cells and for the production of blood cells.
Adenylic Acid, which may have something to do with
the healing of mucous membrane ulcers.
Filtrate factor: This is a group of substances whose
chemical composition and action in the human are not
known. Some of their elements seem to be related to
blood building.
The remaining water soluble vitamins are vitamins C
and P.
Vitamin C (Ascorbic Acid) is present in fresh fruit
juices particularly in the citrus fruits, and in vegetables
and raw meat. It is destroyed by heat as well as by
drying, so that cooked or dry preserved foods have lost
this vitamin. It is required for normal growth of teeth
and bones and helps maintain normal gum structure.
Recently, claims have also been made for vitamin C as a
resistance factor in colds. Medicine cannot yet say the
final word on this.
Vitamin P (Rutin) is found in fresh fruit juices and
especially in lemon rind and buckwheat. This vitamin
increases the strength of capillary blood vessel walls.
73
MINERALS
The term minerals should preferably be inorganic
constituents, since iodine, chlorine, fluorine and phosphorus are generally included in the list of essential
minerals. The actual minerals are calcium, sodium, zinc,
copper, potassium, manganese and cobalt, and finally
sulphur, really a non-metallic element. These may occur
bound up in complex organic molecules or as simple
inorganic substances.
Here again, we still do not know the complete story of
the functions of all the minerals in the body and intensive research continues. We do know they are essential
to maintain life and that many phases of cellular activity
cannot be carried out without their presence in proper
proportions. They, like the vitamins, can all be found in
natural (unrefined) foods.
Calcium is essential for growth and maintenance of
teeth and' bones. It helps control the irritability of the
nervous system and is needed for clotting of the blood.
Milk is the most reliable source. Non-milk drinkers must
find adequate substitutes in milk derivatives.
Phosphorus is essential in tissue building, especially
of bone and teeth, and is a constituent of every cell in the
body. It also aids in the metabolism of fat and
carbohydrate.
Iron is contained in every cell nucleus, is essential for
production of the hemoglobin in the red blood cells
which transport oxygen to the body cells. A deficiency
produces anemia.
Copper is present in enzymes and assists in the manufacture of hemoglobin.
Iodine is necessary for the proper function of the
thyroid gland (use iodized salt).
Sodium helps maintain the proper water and acid base
balance in the body. It is found in common salt.
Overweights are usually cautioned against taking too
74
much salt; however, this is only valid in certain disease
conditions, not for the average.
Magnesium is important in regulating nerve and
muscle activity; it also balances the action of certain
enzymes in the body.
Chlorine is important as the partner of other metallic
elements in maintaining the body fluids at proper concentrations. It is also necessary for the formation of
gastric juice (hydrochloric acid) vital for digestion.
Sulphur is necessary for proper development of hair
and nails and is an important factor in protein metabolism.
Cobalt is essential for normal growth. It also has a role
in carbohydrate metabolism.
Fluorine decreases the caries in the teeth.
Mineral deficiencies are difficult to diagnose, except
for calcium, iron and iodine. You don't have to go prospecting for the specific minerals (or vitamins) in special
foods. All are present in meats, vegetables and other
natural foods in adequate amounts to cover normal
needs. If you eat fish and/or meat daily, liver once a
week, milk and fresh fruit or juice daily, whole wheat
bread and whole grain cereals, green and yellow vegetables daily or every other day, you are unlikely to suffer
any deficiency in either minerals or vitamins—even if
you must cut out other foods in your weight reduction
program.
75
Chapter V
MAGIC MYTH AND MEDICINE
A BRIEF CONVERSATION with a non-medical friend
concerning this book may be worth repeating.
"What gimmick are you giving them?" he asked.
"None," we said, "except the truth. Important truths—
a knowledge about their most precious possession, their
bodies."
"Truth?" said this hard-headed gentleman. "They
won't buy. People want to believe, not to know. Give
them an easy magic formula. It's faith that makes them
flock to Brand X, or try the latest reducing diet, or give
their lives in battle."
"We're not in the Middle Ages," we said. "This is the
age of sputnicks, of a great scientific era. Medicine is
making daily strides forward. . . ."
We each stayed unconvinced but the exchange set
one's thoughts on the continuing battle science must
wage against easy magic formulas. Medicine has made
greater progress in the sixty-odd years of this century
than in all our previous history. Doctors no longer need
to hide their ignorance behind a Latin prescription—we
know so much more today. Only we haven't let the
layman into our sacred preserves, which is the purpose
of this book. And so he makes easy prey for charlatans.
This week's front page of The Times, Feb. 4, 1962, has
two items in adjoining columns. One is headed: "Contact
with Worlds in Space Exploration by Leading
76
Scientists." It tells of a conference sponsored by the
National Academy of Sciences at Green Banks, W. Va.,
location of a great astronomical observatory, "to explore
the possibility of communication in outer space."
The second item, "Line-up of Planets Stirs Hindus,"
says: "Uneasiness gripped India tonight at the beginning
of a period that, according to astrologers, could bring
doom to much of humanity. Five planets moved into the
constellation of the House of Capricorn . . ."
Centuries ago, astrology became with Copernicus and
Galileo the science of astronomy. Yet its beliefs persist
into our day, and not only among illiterate Asiatics.
Many an American college woman will not date a man
born under an uncongenial star. And there are Wall
Street speculators who do not undertake their next coup
before they consult a horoscope chart. Similarly, scientific medicine which grew out of "white magic" in the
dim and distant past has to exist side by side with its
survivals. We still find witch doctoring on all the continents, and among our own people a pseudo-scientific
quackery that abuses our faith and credulity.
In each of us lurks a primitive being who believes in
myth and magic. We doctors understand this and work
with faith as a force in the healing process. We recognize the emotional value of a "bed-side manner"; we
occasionally prescribe a sugar-water placebo to pacify
the patient who needs (psychological) medicine.
Yes, faith will move mountains—and will it remove
the tiny hillock on your abdomen? If voodoo can kill,
rattlesnake bite is far more deadly, against the strongest
faith of our mountaineer cultists who usually die when
they refuse anti-toxin. Snake worship is rare in America,
but food cultism has millions in its grip.
It takes two shapes: in fads sponsored by highly
respectable advertising media, a part of our cultural
mores, and in the nutritional fakery of "miracle foods"
which promise to ward off diseases from chilblains to
cancer, and to insure good health as well as sexual
stamina. The two are equally pernicious.
77
Webster says a fad is "a custom, amusement, etc." also
"a craze." Food fadism that glorifies blackstrap molasses
or safflower oil swings into the crazy stage. Let us,
however, look first at a milder phase: "dietetic foods."
Enter a food market and you see whole sections devoted to low-calorie foods—more expensive than their
regular equivalents and offering less value. This department sells everything from sodas, salad dressings, sugarless cakes and preserves to slenderizing breads. If you
must eat such foods, these at least contain fewer empty
calories, but should they replace the natural foods you
were brought up with? Will they keep you slimmed
down without having to fuss over your diet? They
almost claim to. They cry out: "Eat well, cut calories,
look marvelous!"
We are being brain-washed. Marketing experts have
surveyed our yearnings and analyzed which packaging
will best impel us to buy. It is labeled to that specific
effect. Eating specialty foods is certainly easier than
crash dieting and is less dangerous, but just as
ineffectual for lasting weight reduction.
Another fad has developed around protein-enriched
foods. There is "fortification" in most of the 68 breakfast
cereals recently counted by Consumers Research. Yet,
despite the merchandising propaganda, enriched cereals
and breads remain predominantly starch, often with
hidden sugar calories. The term high-protein is used,
implying Grade A protein. The 11% protein in white
flour is good, but not complete, as is the superlative
protein offered in meat or fish, or even the subsidiary
sources in cheeses and legumes. While cereals have
their place in a reducing diet, they need no protein
enrichment. You would not in any case want to draw
much of your 100 grams of protein from the cereal
foods.
Exactly the same caveat holds for "vitamin enrichment" of milled products which reads so very impressively. A truer picture would be given if the vitamins
filched from the grains and not restored were listed on
the bread or cereal wrapper. To the extent your diet
78
allows, eat whole grained wheat, whole grain rice or
grits and whole wheat bread, each offering a full complement of B vitamins.
Thus far, all of the claims made have been on the
'legit" side. Far more wide-spread and exploitatory is the
quackery involved in the promotion of food supplements
with magical properties and the wonder-working
vitamin products. Its victims are mostly older persons,
frantically seeking and clinging to panaceas. They also
include the overweights, deluded by a promise of
slimness and health easily gotten from safflower oil, 900
calorie diets, or what-have-you.
Food and Drug Commissioner Larrick gave the government view succinctly: "A vast mythology of nutrition
is being built up by a pseudo-scientific literature in
books, pamphlets and periodicals. Millions of people are
attempting self-medication . . . Self-styled nutritionists
prescribe various food items ..."
On Jan. 23, raids by government agents caused quite a
flurry in the news. They seized 58,000 capsules which
did not contain heroin and 1600 books that were neither
subversive nor under-the-counter pornography. What
sent both medical and book circles into a dither was that
the books were copies of "Calories Don't Count," the
best-seller written by a medical doctor.
According to The Times of Jan. 24, "the complaint
filed by the Food and Drug Administration contended
that the promotional material accompanying the sale of
safflower oil capsules, including the book, was 'false
and misleading.' The capsules supply 5.5 grams of oil
daily which was described (by the government) as insignificant for any purpose.'"
Whether the seizure was justified on the grounds of a
"promotional tie-in" may have to be determined in the
courts, but its action thrust the case into the public
domain of thought and discussion. We will not shirk our
responsibility to render a medical judgment on the highfat reducing diet expounded in the book. We shall
79
therefore return to the author's claims later—but two
other government raids bear mention here.
On Jan. 7, according to the A.M.A. News, the Food and
Drug Administration had seized another book, this one
by a non-medical nutritionist and radio personality, "Eat,
Live and Be Merry," on "charges that a dealer was using
the book to make false claims for the medical value of
vitamin and mineral supplements."
Several months earlier, a very expensive vitaminmineral tablet with a fabulous sales success across the
land was likewise seized. The charge here again was:
"false and misleading labeling." Its literature was said to
describe it as treatment for 27 listed ailments, "including
impotency and frigidity."
The government is not trying to censor our reading nor
to curb our freedom to buy as we fancy. Its mandate is to
insure that a product is correctly described for the buyer.
Yet, undeniably, an underlying aim is the education of
the public. K. L. Milstead, Director of the Bureau of
Enforcement of the Food and Drug Administration has
expressed this with a Churchillian ring: "Our purpose is
to challenge food faddists and nutritional quacks on all
fronts—in the courts, in the press, wherever they appear.
. . ."
We share his purpose for we know that weight reduction can be a destructive process unless there is a knowledge of nutrition, an insight into food values that can
evaluate fads and free-wheeling gimmicks. Let us ourselves now assess a few of the favorite "miracle foods"
of nutritionists.
One of the most reputable among them, who herself
warns against food faddists and crackpots, urges the use
of blackstrap molasses for its calcium, iron and vitamin
content. Yogurt is the most extravagantly praised of all
nutritionist stand-bys with millions of devotees. Gelatin
is being pushed as a protein base for a reducing diet.
What is the true worth of each?
Molasses is an end product in the production of sugar.
The darker the molasses, the more refinements the origi80
nal syrup has gone through and the more impurities it
contains. Aside from remaining sugar, all it has is these
impurities, which include some iron. Blackstrap has no
magical properties. It is no source for any supplement
not available in better form in more natural foods. You
can lead a full life without ever touching the stuff. Taking blackstrap is the least valid and silliest of all the
food rituals.
Yogurt has adherents the world over. It is protein, all
right, but nothing more than whole or skimmed milk
which has been used as a culture medium for the lactíbacillus germs. If you like it, it's good for you. And it
may be medically beneficial if you require the bacterial
action of the germs in your intestines where it can help
prevent gas formation. Then don't buy the commercial
yogurt which is usually pasteurized, killing off most of
these desirable germs.
Better still, make your own—it isn't difficult. Take
one quart of skim milk or the cheaper dry milk powder.
Add two tablespoons of bought (plain) yogurt. Allow to
stand for three hours until the milk thickens, then refrigerate. To start the next batch use two tablespoons of this
made yogurt, continuing the culture indefinitely. You
can flavor to your taste.
Gelatin has been touted as a fast pick-up protein
source, which it is. It is usually prepared from animal
tendons and bones by steam cooking. It can be used
flavored, in desserts, and plain, to be mixed with fruit
juices, etc. The ladies make some pretty things with
gelatin but it should not be taken as a complete protein.
It lacks a number of valuable amino acids including
tryptophan and tyrosin, two essential acids, and is thus
much inferior to the Grade A proteins. It is advertised as
"enhancing the vitamins of the foods used with it"—
meaning: Don't depend on gelatin to stand alone.
We could go on in this way with other food supplements enshrined in the nutritionist holy writ. There is
yeast, which can blow up your insides like a balloon.
And wheat germ and bran, which belong in the grains
81
they are taken from. . . . But let us end this pitch to end
all pitches by a final glance at the most popular and
costliest quackery of all—the vitamin myth.
The public has been taught that so long as they take a
vitamin pill containing several times the recommended
"daily requirement" they are fully insured against nutritional deficiency. What did people do before we robbed
food of its vitamins to seal them inside a pill or learned
to synthesize them—before we ever knew of their existence?
Don't be misled by the mystification surrounding unknown and freshly discovered vitamin values. True, our
knowledge is still incomplete. It is, nevertheless, probable that the most prevalent and serious deficiency conditions are already known. It is also logical to assume
that the unknown factors are as well distributed in a balanced diet as the known are. Therefore, can we not assume that the proper diet will adequately provide all the
accessory food factors?
Should everybody take vitamin pills? Vitamins, si,
pills no—well, maybe. As has been said before, vitamins
and minerals ought to be gotten off your plate. It is true
that most Americans suffer from a lack of some nutrients
including these—but you can best correct the deficiency
when you know your nutritional needs. Vitamin-mineral
supplements may have a temporary use while you regulate your diet. They can also benefit the individual
whose body cannot absorb or store the requisite
amounts. Your doctor will help determine your deficiency.
When a physician prescribes vitamins or other drugs,
he often recommends known brands of reputable pharmaceutical houses, though they are usually more expensive. He has not been bribed or brain-washed, despite the
constant propaganda barrage by the pharmaceutical
houses (and the samples). He wants to be sure the bottle
contains what is claimed on the label. A case in point
that came recently to our personal attention is worth
recounting.
82
A healthy young boy was brought to the family physician by his alarmed parents. He had lately developed a
female-type figure with rounded hips and inordinantly
large breasts. The suddenness of the change led to a
diagnosis of probable female hormone intake. Detective
work inquiry by the doctor pointed to the recent addition
to the boy's diet of a vitamin supplement. Chemical tests
showed that this vitamin pill was saturated with
hormone extract. It was subsequently discovered that a
batch of vitamins had been mixed in a vat which
previously held hormone—someone had not cleaned out
the vat.
The boy was brought back to normal. And the company? A slap on the wrist—a fine of three hundred dollars. The Food and Drug Administration is kept awfully
busy trying to protect you, but Federal law is easily circumvented. The department doesn't have the necessary
funds or manpower to do the job they would like to do.
A partial solution would be a careful scrutiny of all
advertising and self-discipline by the media of radio, TV
and the press themselves. The final check on the merits
of food nostrums is a knowledgeable buying public.
It isn't easy to see through the clever propaganda of
quackery. It usually starts with a true statement of fact
(Yogurt is good for you; blackstrap contains iron). It
then develops this theme with faultless logic until the
individual is convinced. Then, imperceptibly, the truth is
bent—at a very slight angle. This angle then becomes
doctrine blown up into a tenet of faith for all true believers. Clever? Terrifying!
Against this the public must develop a counterweapon of skepticism, buyer resistance. Why pay 9
cents for a "protein" pill which is only powdered milk?
Why buy safflower oil in capsule or in liquid form when
the more common and cheaper corn oil is just as good?
A daily spoonful as salad dressing plus fish foods will
provide all the highly unsaturated oil you will want.
Let us make a slight digression to a food myth not
created by advertising but very prevalent among cultists.
83
There is a belief and a great concern that our food comes
to us deficient, because of commercial fertilizers, and
contaminated by insecticide sprays. There are people
who send off to California for lettuce and apples which
are worm-eaten, in order to have "organic, uncontaminated" food. Yet tests made at various U.S.
plant, soil and nutrition laboratories show there is no
difference in the composition of crops whether from
natural or chemical fertilizers. Our agricultural
technology is held in the highest esteem by the rest of
the world. They copy our methods, buy our seed, use
our know-how to get better crop results.
Chemicals used in food spraying (though they unfortunately injure bird and wild life) have been proved safe
for us as well as efficient. The worm-eaten apple
referred to above recalls the old-time gag our younger
readers won't be familiar with: "What is worse than
finding a worm in an apple?"
Answer: "Finding half a worm." The young will not
have heard this because a wormy apple is such a rarity
today nobody even bothers to look. Whatever laxity has
been shown in the past, government supervision and
control have become increasingly strict and efficient in
protecting our food supply.
We are now prepared to examine the magic and myth
in crash dieting. A typical reaction to obesity, found particularly in the adolescent, is a violent revulsion against
food. He, or far more often she, thinks: If eating has
made me this ugly, to the devil with it! Actually, there is
a rejection of the fattening body, implying: "If you have
done this to me, 111 get even." She ignores that it was
she who "did it" to her body and is now about to punish
it further.
The self-inflicted damage of teen-age dieting can undermine life-time health. One high-school girl, plumpish
with what she called her baby fat, with heroic resolution
had been starving herself. No breakfast, half her sandwich for lunch, a picked-over dinner, and in between,
she later confessed, heavy smoking and coffee drinking.
84
Speaking to the doctor, she dignified this self-abuse by
the title: "coffee and cigarette diet." She had certainly
lost weight in her shrunken internal organs and was already developing symptoms of severe deficiency diseases.
In a certain college for girls the "cigarette and coffee
diet" was combined by a group, not all of them fatsos,
with lack of sleep and dexedrine pills, too freely prescribed by a local doctor. An onslaught of gastric irritations, incipient ulcers and "breakdowns" (a prelude to
the colitis and mononucleosis that have replaced tuberculosis as student diseases) provoked such havoc that the
resident physician and the dean had to undertake a
vigorous campaign of nutritional education. These are
instances of frank starvation dieting—but all crash reducing is in varying degree a starvation process (described below), its ravages varying only with the selfdestructive wish of the reducer.
There are many kinds of trick reducing. One, popular
for a while, was the "sawdust diet," in which bran and
water-retaining cellulose (wood) extractions swell in the
stomach to give a feeling of fullness. More common is
the use of pills (or sometimes injections), all sorts of
pills working in different ways to curb the appetite, or to
increase the metabolic rate, or simply as laxatives and
purgatives.
The
appetite
depressants
(amphetamines,
phenmetrazine, etc.) do dull your hunger but also make
you nervous and tense. They can produce insomnia,
headaches, dizziness and nausea. These symptoms are
the early signs of starvation but the drugs in themselves
have side effects. Physicians, therefore, prescribe them
cautiously and are warned by the manufacturer not to
give them in cases with cardiac disease or high blood
pressure.
Experience with patients has shown that many develop
gastro-intestinal disturbances. There is an overstimulation when taken for some time, as with benzedrine,
and a danger of addiction—in that one becomes
85
dependent upon them for this stimulation because of a
let-down feeling when the drug is stopped. The artificial
mental pick-up always followed by a "low," true of all
stimulants, eventually leads the patient to increase the
dosage. Many a young woman has as a result been hospitalized because of fainting spells and even physical
collapse.
It is claimed that the newest appetite depressants have
fewer side effects. Clinical experience with these is as
yet inadequate for proper appraisal. If your physician
feels you need their help at the start of weight reducing,
abide by his instructions. Do not juggle dosages on your
own. And remember, you cannot depend solely on the
crutch of the depressant. What happens when the pills
are stopped? Do you want to be taking them for the rest
of your life? There is no magic formula, no quick and
easy way—only diet control through self-control.
We come to the seemingly reasonable, quasi-scientific
approach to crash reducing. People say: "If milk is the
food par excellence, what's wrong with the skim milk
(or cottage cheese) diet? Or a milk plus orange juice
(bananas, etc.) diet? Or the 900 calorie diet which "has
everything?"— Will you lose weight through each of
these? Yes, but . . .
Two things are wrong with all of them. As with pilltaking, they are a pattern which you can follow for a few
weeks and no more—provided you have not fallen ill in
this period. None of them is conducive to proper eating
habits as a way of life. They are forms of penance after
which one inevitably regresses to the old sinful patterns.
Like the alcoholic who periodically "goes on the wagon"
yet ends up with cirrhosis.
Aside from being morally wrong, they are dangerous.
A too rapid and unphysiological weight loss produces
profound disturbances in the body mechanism. Fortunately, we are able to withstand an unbelievable amount
of punishment and still repair the damage done. Yet,
sometimes, the body repair is not complete, particularly
after repeated attempts at crash dieting.
86
We can learn the effects of the partial starvation produced by your favorite gimmick diet when we study the
body during actual starvation. We continue to require
energy—the basal energy that keeps life going. It takes
approximately 1700 calories to maintain normal temperature, lungs breathing, kidneys filtering the blood
plasma, intestines performing—all the big and minute
activities of body function even when completely at rest.
To obtain this energy, the body lives on itself.
It is somewhat like the fable of the boat with fuel
exhausted whose captain has to decide what to throw
into the boilers to keep moving. First, in goes the cargo
(the body fat); then the furniture (muscle protein) is
sacrificed; finally the spars and planking (the protein of
vital organs)—after which the boat and the human body
go under. The marvelous complication of the body,
however, demands a far more detailed description.
During the first few days, the glycogen stored in the
liver and muscles is used up, though never completely
because the liver will continue to produce some from
whatever source is available. Enough sugar must always
circulate to maintain a blood level concentration of 80120 mg. per 100 c.c. The comparatively unessential
muscle protein is drawn upon first to be converted into
this necessary glucose. The tell-tale nitrogen balance is
now being upset through an outgo without any protein
intake.
The main energy source, however, remains the stored
fat. So long as it is available, it spares the excessive
ravaging of the vital protein in fundamental organs.
Body fat may likewise be divided into disposable adipose, called the élément variable, and the vital fat, necessary to cellular structure and called the élément constant. When the body surrenders the variable element
from under the skin and between the muscle fibers, it is
mobilized by the liver, its fatty acids are changed into
unsaturated fatty acids, and these are then returned to
the tissues for burning.
The burning of fat in the absence of carbohydrate is
87
usually incomplete (See last chapter). The body automatically tries to correct the menacing acidosis. Breathing becomes deeper and more frequent; less carbon
dioxide is given off, since it is being used by the blood
to neutralize the disturbing acids. The wonderful instrumentality within us strives to make every conceivable
adjustment to save itself during starvation or crash dieting. But the body can take only so much. If not death,
permanent damage may be sustained.
The constant element or the cellular fat of the heart,
lungs, kidney and brain remains unchanged to the last.
This fat is incorporated into the cellular structure in
complex molecules of cholesterol and lecithines. Only
when the cell has been damaged by injury or a toxic disease (like diphtheria) will the fat appear as visible
globules, separated out from the homogenous protoplasm. This condition is known as fatty degeneration,
familiar to the pathologist.
Destruction of body protein has meanwhile gone on
because of the daily tissue breakdown, red blood cell
degeneration and mucous loss in the intestines. There is,
in addition, the continuous loss of the protein changed to
glucose. This is first broken down into amino acids
which are brought to the liver where they are acted
upon, exactly as if they had come from normal absorption. Aside from the glucose, urea is formed. Excreted in
the urine, it can be used as a measure of tissue destruction during starvation, or in a low-protein regime.
If and when the adipose fat and the muscle protein
tissue and the never-surrendered constant fat remain, we
have reached the danger point. The essential organs are
the last to be sacrificed. Muscles, spleen and liver lose
extensively, while the brain and heart keep their protein
bulk. But the process has now become irreversible.
Death follows rapidly.
Since this gloomy description is intended again to
point up the need for high-protein in a reducing diet, a
question arises. Can a limited amount of protein, exclusively, be taken for weight reduction? Say, the amount
88
bound to be used up in diet-starving the body. We have
recommended 100 grams per day. Why not a crash diet
containing nothing but this amount of protein—no fat or
carbohydrate?
Let us see why not. Assume the individual requires
2400 calories per day. The 100 grams of protein supply
about 400 calories, leaving a deficit of 2000 calories to
be gotten from body tissue. Some body fat will be
mobilized to make up the deficit, but along with it much
protein will be consumed to provide the essential glucose. It has been calculated that the ratio of body protein
to fat used in starvation (or crash dieting) is about 1
gram to 2.5 grams of fat. This means that in any such
rigorous dieting program, valuable body tissue must go.
If, on the other hand, we include a limited amount of
carbohydrate and fat in our high-protein diet, then normal function can be maintained without tissue breakdown. These spare the protein. As the body fat is utilized, with sufficient protein replacement and with exercise, new and healthy muscle tissue is developed in
place of the adipose. There are no short cuts, not even
through high-protein.
Yet short cuts continue to be offered. The 900 calorie
fad is sweeping the country like wildfire (or a virus). It
is being sold in drug stores and in all food markets. Perhaps soon, in a logical climax, it will be served up in
restaurants as manna to obviate all eating. We already
find it in umpteen different brands, shapes and forms—
as liquid in containers, in cans and powdered, and as
wafers to be taken with water.
One must bow in awe before the power of the advertising fraternity. Almost overnight the 900 calorie diet
has been made to sweep the country. For years various
foundations, city health departments, the national Nutrition Council and the Department of Agriculture have
labored to inform the public on food and diet. And nobody stands in line for mostly free and excellent pamphlets on food values, menus and shopping suggestions
issued by these organizations. If we could only use the
89
promotional techniques of big business in teaching nutrition!
Most of these 900 calorie diets do have a fairly good
distribution of carbohydrate, fat and protein and contain
the necessary vitamins and minerals. They are usually
made up of milk products, sugar, starch, corn oil,
coconut oil, yeast, plus flavoring. If you insist on a drastic liquid diet, against all our persuasion and the clamorings of your body, you can make up your own mix containing equivalent nutrients, at about one third of the
cost.
Place in an electric blender about 7 ounces of non-fat
powdered milk, q ounces corn oil and enough water to
make a quart. This will provide 70 grams of protein and
900 calories. Flavor, mix and drink—and then?
We offer this formula to show you it holds no magic
—and we warn against it. It is actually well-balanced—
from a purely theoretical point of view. How long can
you stay on it? Is it a normal way of living? Or are people just too lazy to diet properly? They simply open a
can and pour.
Because of the lack of bulk in these low-residue diets,
constipation is a common occurrence. Despite the variety of flavors, many persons complain of the taste. More
important, one gets a bloated feeling (not denied by
company literature), gassiness, belching and upper abdominal discomfort.
In fact, 900 calorie drinking diets are starvation
rations (whose effects have already been fully described). They do not offer the body adequate liquids.
Even a solid crash diet of the same food values is better,
or not as bad, because it at least gives adequate bulk.
The teeth get the necessary exercise, and the digestive
juices receive their almost-normal stimuli for proper
function.
Again, to expose the total inadequacy of the liquid
diets, we present below their equivalent in a typical 900
calorie semi-starvation eating diet, offering about 70
grams of protein.
90
Breakfast: 1/2 grapefruit; 1 egg; 1 slice thinly buttered
toast; coffee or tea.
Lunch: 2 ounces lean meat; 1 slice bread; 1 serving
vegetable salad; 1 glass skim milk.
Dinner: 3 ounces lean meat; 1/2 cup 5% vegetable; 1
medium tomato; 1/2 cup 10% fruit.
Snack:
1 glass skim milk.
And once again, we advise against it. You may recklessly choose to disregard the internal effects of drastic
dieting with its too rapid weight loss. But for cosmetic
reasons, at least, it is best to lose weight slowly—to
prevent that haggard look, the flabby arms and legs,
loosened breasts and an abdominal wall hanging in folds.
We promised to return to an evaluation of the high-fat
diet proposed in "Calories Don't Count." What magic
does it hold, what myth does it propagate, can its claims
bear analysis?
The New York Post, Jan. 25, quotes a medical colleague, Dr. Morton B. Glenn, an expert on obesity with
the New York Health Department. According to the Post,
Dr. Glenn "supports the government crack-down . . .
described the current eat-fat-to-lose-weight diet as a
worthless fad."
Yes, there are conflicts within medicine and the "highfat" doctor can be wrong—even a group of doctors can
go astray. Only a few years back, an experimental medical group under the awe-inspiring aegis of the Rockefeller Institute for Medical Research (the ne-plus-ultra of
medical conservatism), evolved a low-protein diet. Their
logic-stood-on-its-head theory was that by limiting the
proteins vital to the body, its appetite could be controlled,
actually throttled by a bulky supply of starches, sugars
and fats.
This diet did "cause a fairly consistent reduction of
appetite" plus, one wonders, what other depression of
body impulse. The final report, however, contained a virtual repudiation of the plan: "All patients, when re91
leased from supervision, modified their diet in the direction of previous patterns"—luckily for their health. Yes,
doctors and scientists are not infallible.
The high-fat diet, however, is still being defended in
full page ads for the book and therefore demands closer
scrutiny. On the positive side, there is some psychological value in being told by the author: "On a high-fat diet
you can eat as much as you want, as many steaks and
chops as any hungry man could ask for." This must
bring release from long-accumulated guilt to many
obese persons—and may result in less compulsive
eating.
Then there is the high satiety of fats, greatly increased
by frying them in oil—ugh! One patient, we have been
informed, told to eat a dozen fried scallops could barely
get down seven without nausea. Perhaps, then, a weight
loss might be achieved as a result of a calorie deficit.
Because, inexorably, every reducing diet must create
such a deficit to succeed.
The book describes weight reduction in cliffhanger
style, with safflower oil in the heroic role outwitting
pyruvic acid in the villainous role. "Pyruvic acid acts as
an inhibitor of the ability to get rid of fat."
The pyruvic acid indictment is not without basis. It
has long been known that excess carbohydrate can be
converted to fat via pyruvic acid. But this holds only for
an excess. The normal carbohydrate cycle does not include this acid formation. And in a reducing diet there
will be no excess carbohydrate.
"Carbohydrates," we are further told, "contain no
essential substances . . . Many of us could subsist without eating any carbohydrates at all." This is misleading
advice. What about vitamins, especially C found only in
fruits, vegetables (and in raw meat)? And even more
disturbing, what of the danger of burning fat without the
presence of carbohydrate?
It is true, as is claimed, that the "body can burn an
unlimited amount of fat." Provided it is burned in a
carbohydrate fire and that there is sufficient work done
by the body to burn up the stored as well as the added
92
fat—and this would take superhuman exertion. Our
high-protein diet is by no means hostile to some fat
intake—even lean meat has a goodly percentage. Grilled
beefsteak, for example, consists of 25.2% protein and
21.6% fat; lean roast beef has 26.7% protein and 15%
fat.
The use of fat in weight reduction is not new. Long
before "Calories Don't Count," in the late nineteenth
century the physician and nutritionist Ebstein used it
with good results. His patients, however, were kept in
private sanitoria on a rigorous regime, with limited
calorie intake. Ebstein also allowed some fresh fruits
and vegetables but relied mainly on fatty meats for their
high satiety value. This was before we became wary of
fats on the score of cholesterol, and before we understood saturation. What has been added in this newest
high-fat diet is the abracadabra of safflower oil.
The book also contains a series of arguments against
low-calorie diets which must be refuted here, since our
proposed high-protein diet is of necessity low-caloric.
1. We are told that low-calorie diets are not effective
for weight reduction. They are in fact the only effective
physiological way of losing weight produced by an excessive energy intake. The reason they so often work out
badly is that they are usually too rigid, not properly
balanced, not a way of life. A high-protein, well-balanced diet, limiting the energy foods, will be successful.
2. A low calorie diet is "not harmless." One can more
readily say this of the high-fat diet. High-protein is on
the contrary not only harmless but beneficial since all
the body requirements for protein, vitamins and min
erals are met.
3. It is "temporary." Here we heartily agree. The management of obesity entails an arduous grind on the part
of the reducer until a new pattern of eating habits
evolves. Satiating high-protein plus an understanding of
foods will permit a gradual easing of the restraints.
4. It is "based on incorrect ideas." I believe we have
shown in the course of this book the correctness of a
basically high protein low-calorie diet.
93
5. It "does not affect the cause of obesity." This is
redundant. No diet will affect the cause when it is other
than overeating. Even the faddists accept as fact that
overweight in 95% of all cases is caused by a calorie
excess.
Obesity requires a watchfulness of your food intake,
an adjustment of the amount and types of food to the
individual you. And you won't have to walk about with a
caliper or scale, or, for that matter, a food chart. Common sense backed by some knowledge and resolution
will help you lose weight in a medically safe and sane
way. You will become not only slim but a healthier and
happier person.
94
Chapter VI
HIGH LIFE ON HIGH-PROTEIN
AFTER so many questions put and answered for you
with so much argumentation and array of fact, you may
yourself wish to ask a tired question: "Since a reducing
diet needs carbohydrates and fats along with protein,
why not just take some of everything? Why not, in fact,
stay with calorie counting?"
We have no prejudice against calorie counters—some
of our best patients are or rather were among them. We
have also observed them over the years in restaurants
and cafeterias,, choosing their foods with utmost concentration (on calories while ignoring nutritional values)
and ending up malnourished and ill.
In a certain hospital cafeteria for the medical staff, as
the lunch line approaches the food table there is a
segregating out of the sexes. The men usually head for
the blue plate dinners, a choice of meat or fish; the
women waver between the salads and the sandwiches
which they may supplement with a soup.
Behind the gleaming chrome and tile the sickly salads
stand: corrugated chunks of blanched-out lettuce topped
with a few slices of egg and pulpy, whitish tomato or
with a 2-ounce scoop of cottage cheese. Next come the
cellophane-wrapped sandwiches, mostly of white bread,
holding razor-thin fatty ham or thicker baloney (the
cafeteria is expected to show a profit). Then, set temptingly near the coffee urn, are the desserts. Here the
95
dietician comes into her own, though she appears to have
confused palate with palette in offering a riot of colorful
jellos in red, orange, green, and blended colors, followed
by alabaster custard, snow-white yogurt, cherry and
lemon pies, even cuts of a seven-layer cake.
A gentleman on the line, elderly but trim and with
good (natural) coloring, quickly chooses the meat dish,
served with two vegetables, and is satisfied with a slice
of bread, butter and coffee. The lady next to him is only
slightly rotund, yet her face gives an odd impression of
fleshy gauntness with puffy cheeks, hollows at the jaw
line, sagging chin and sunken eyes. Quite obviously a
calorie counter, she takes the almost nutritionless
(starchy) soup with soda crackers, then vacillates between the salads and sandwiches, in the way the very
poor must check their purse before making a purchase.
She asks for the salad, its only food value in the few
pennies' worth of cheese, hesitates before taking up a
slice of bread, abandons the butter and advances for her
drink. So far she is all right, with some slight edge of
starch over protein, but it will be easily remedied if she
takes milk. She orders black coffee, instead, and views
the desserts with stony resolution until her eyes fasten on
the seven-layer cake, oozing with colored syrupy paste.
She has long steeled herself and her brow now furrows
with the problem—she is a lightning calculator: Oh, to
eat one's cake and have the slimness too!— But stronger
than arithmetic is the call of her blood (the low blood
sugar of chemical hunger). "It looks so delicious," she
says to the counter girl as she reaches for it. Then, with
an uneasy laugh: "I'm living it up today."
The lady had her direction wrong—she was most
decidedly living it down. Perhaps she discovered this in
the afternoon with her increasing fatigue and troubling
irritability which she probably could not explain; perhaps at some later date in graver symptoms that invariably result from a continuing high-carbohydrate diet.
Really "living it up," zestful living on high-protein
96
during and after weight reduction, is the theme of this
chapter.
Was our health picture of the lunching lady, seen
through makeup and clothing, exaggerated? We believe
not. One can safely generalize that her craving for
sweets was a chemical hunger due to low blood sugar,
caused in turn by a protein-deficient breakfast. And that
the lavish starches and sugars in her luncheon, despite
or perhaps because of calorie counting, further tipped
the imbalance. There is no more vicious physiological
circle than this one of blood sugar. The immediate consequences were described in the last chapter. But there
is one cumulative resulting condition that deserves
going into at greater length.
Every physician has seen cases of hypoglycemia, a
disorder indicating a sub-normal blood sugar level. It
may derive from organic diseases such as pancreatic
tumor and liver or glandular disorder. For simplicity's
sake, however, we shall limit ourselves to the functional
condition, in which the symptoms result from the body
chemistry in an otherwise healthy individual. From a
wealth of cases in our files let us review two, in the
hope that some readers may recognize themselves at an
early stage in these case histories.
Mrs. Smith, a housewife forty years old and about
fifteen pounds overweight, complains of extreme fatigue
and continuous hunger with pain in the pit of her stomach. She is certain she must have an ulcer. She has lately
become easily excitable, has a sense of anxiety with no
definite cause. She suffers at times from profuse sweats
followed by chilliness; her hands and feet are always
cold.
A physical examination revealed no obvious defects.
A CBC, BMR and electrocardiograph were within normal limits. The fasting blood sugar was at 76, slightly
below the normal 80-120. A gastro-intestinal x-ray
series showed a normal stomach, though with overactive
contractions; the small intestine was likewise normal but
97
emptied very rapidly. These were the only clues. A glucose tolerance test was then undertaken.
Mrs. Smith was given 100 grams o£ glucose with water; blood tests were to be taken at half-hour intervals to
determine how her system handled carbohydrate. About
twenty minutes after drinking the glucose she started to
tremble, became pale and complained o£ feeling faint.
She was helped to a cot and broke into a profuse sweat,
saying she was nauseated. She then seemed bewildered
as to her whereabouts and spoke incoherently.
Blood was withdrawn for testing and a hypo of adrenalin was administered, quickly bringing her around. The
remainder of the glucose test was abandoned, for
analysis showed that her blood sugar had shot down to
an extremely low level of 44 mgs., far below normal.
The reaction to the glucose explained all her previous
symptoms.
Her condition was due to the too rapid absorption of
carbohydrate in her intestine, thereby sharply raising the
blood sugar level. The pancreas responded by a rush of
insulin to help convert this surging glucose into glycogen. Some of the insulin got used up in the process but
an excess remained—acting to produce a type of insulin
shock. This accounted for the disturbing symptoms,
including the continuous (chemical) hunger, and also
pointed to a simple cure.
Placed on a high-protein (reducing) diet, Mrs. Smith
has been symptom-free with no recurrence since. A highprotein low-carbohydrate diet will prevent hypoglycemia as well as milder or graver complications in
two ways. The digestion of the protein slows down the
release of sugar into the blood; excess protein is even
more slowly and evenly converted into glucose. Since
the body is never suddenly flooded with sugar, the
pancreas secretes its insulin in small and sufficient
amounts.
We must learn, as the rotund stranger in the cafeteria
hadn't yet, not to shock our bodies with zig-zagging
98
sugar highs and lows, creating an internal spasticity. We
need to supply our blood sugar with the steady batterylike, "booster" effect gotten from protein.
The second case was a Mr. Jones, who came for a
physical examination because of recent fainting spells.
The latest had occurred at a wedding banquet, but he
associated several incidents with Sunday dinner when he
and the family ate out. The fainting was accompanied by
sweats and usually took place in the middle of the meal.
There was no pain and he would reassure everyone, but
a few minutes later abdominal cramps and diarrhea
would ensue.
Mr. Jones was a stocky man in his late forties, overweight and approaching obesity. He claimed he could
eat anything; his bowel habit was normal. Was this a
heart case? Psychosomatic, perhaps, related to some
secret guilt about eating elsewhere? Nothing like this
ever happened at home.
Physical examination revealed the patient to be a
highly sensitive person. He appeared tense, stuttered
slightly in conversing and actually blushed while undressing. An electrocardiograph was normal; so was
every other index but one. A glucose tolerance test
showed a low fasting blood sugar level with very low
values thereafter.
Questioning exposed the culprit in the Sunday afternoon dinners as the gala cocktail taken after a meager
breakfast, followed by a hungry nibbling on bread and
rolls while waiting to be served—usually a meal rich in
carbohydrates. Apparently, the extreme sensitivity of his
nervous system, recently heightened by his growing anxiety, when beset by high-carbohydrate would react
with violence, disturbing the delicate regulatory mechanism of the blood sugar.
A high-protein diet, adhered to even when dining out,
has precluded any further fainting spells. Mr. Jones
doesn't nibble any more. This does not mean that you
must stop eating breadstuffs or enjoying your cocktail
(after you have reduced to normal weight). Still, per99
sons with the excessive liability of these two patients
have reason to remain wary. It is also probable that their
hair-trigger sensitivity was itself produced by the constant gyrations in their blood sugar caused by a carbohydrate-protein imbalance. The remedy is clear.
Thus high-protein has time and again proven its value
in the human diet. In weight reduction it becomes indispensable, to insure adequate body repair and function
while you are under the stress of a caloric deficit. We
have previously recommended 100 grams of protein as
optimum in maintaining a proper nitrogen balance.
Unlike a carbohydrate and fat excess which, if not
absorbed, may produce indigestion and diarrhea, or else
is transformed into body fat, a protein surplus holds no
danger. It acts as a safety factor and, in the dietary
absence of carbohydrate, is converted into glucose and
burned as energy.
In addition, however, to being very palatable and satiating, high-protein foods offer an advantage far beyond
that of satisfying our physical appetite, the series of
stomach contractions which we recognize as hunger
pangs. They also destroy the chemical hunger, produced
by low blood sugar, with its unpleasant feeling of abdominal emptiness coupled with actual weakness and
fatigue, of dulling out and mental agitation.
The blood sugar, we repeat and it demands a loud and
ringing reiteration (people just don't know), is best
supplied by the presence of protein among other foods,
or by its substitution as a glucose source in a low-caloric
reducing diet.
One of the most trite of truisms tells us there is nothing new under the sun. Certainly, while the food chemistry and physiology we have been outlining are of rather
recent origin, the concept of diet is an old one, going as
far back as the recorded history of man. Among the early
Hebrews, dietary laws (still adhered to ritually)
prohibited in a Jehovian "Thou shall not!" the eating of
certain foods and the mixing of others. It is to be expected, too, since much of Western science flows from
100
the fountainhead of Grecian thought, that Aristotle and
Hippocrates should have offered advice on diets.
Let us leap across a few millennia to precisely one
hundred years ago. In 1862, a Mr. Blanting used and
wrote about the reducing diet which bears his name,
prescribed for him by a certain Dr. Harvey. It was
exceedingly rigid in the quantities of food and liquid
allowed.
Patients were starved on 27 ounces of dry food per
day, half of which was meat (i.e.: high-protein) and the
fluid was limited to 35 ounces. For normal function the
body requires at least 52 fluid ounces, which is about
what is given off in urine and respiration. Fats and proteins were not well balanced—their values were not
understood then—and constipation and malnutrition
resulted.
A while later came the Ebstein diet, already discussed
in connection with the book "Calories Don't Count."
Though Ebstein is not credited for it by the author
(Blanting being substituted for him as godfather of highfat), he was the first to suggest the satiety value of fatty
foods in a reducing diet. He urged, too, that sugar,
potatoes and other carbohydrates be curtailed, with the
exception of 32 ounces of bread.
Breakfast consisted of black sugarless coffee with two
ounces of buttered toast. The noon meal comprised a
meat soup or broth, 4 to 6 ounces of boiled or roasted
(not fried) fat beef, with meat gravy, etc. . . . •We have
learned a great deal since Ebstein—or have we?
The Oertel System was a forerunner of present day
high-protein theory. Oertel doubled the intake of animal
food allowed by Ebstein and halved the fats. Interestingly, he broke ground in insisting on the value of vigorous exercise and recommended mountain climbing: He
wrote:
"Since the force required to raise the body through a
great height entails the destruction of large quantities of
fat, the above exertion will also lessen the fat accumulation, on condition that we give less fat and carbohy101
drates in the food than are used up in the work done."
The reasoning marked another step forward in its
suggestion of the need for creating a calorie deficit.
There followed variations on the Oertel high-protein
regime in the Schweninger System, the Chambers System, etc. In the gay nineties and at the turn of the century
various rival dietary systems each had their vogue. They
drew a growing clientele to the watering places scattered
across Europe. Reducing salons and cures were featured
in the routines of resorts like Vichy in France, Baden in
Austria, and Baden-Baden, Germany. These retreats
have not lost their popularity. In the United States,
today, down-at-the-heels Saratoga Springs, Sharon
Springs and other once celebrated spas recall for us their
own halcyon days.
At such tourist spots, offering perhaps a "magic mountain" for climbing or walks in lovely gardens with band
concerts and other divertissements, the leisure class
would face up to its obesity—at least for a few weeks of
the year. Here they submitted more or less gracefully to
the penance of weight curtailment and graded exercises.
Life was regimented but pleasant and salving to the
bourgeois conscience. It wasn't very different from a
present-day stay at an American milk farm, though our
activity is not as tightly regulated.
It may be of some antiquarian interest as well as
instructive to skim over the more successful high-protein
reducing systems, each of them contributing to our
nutritional knowledge.
The Schweninger System, based on Oertel, was highprotein with a vengeance. It included:
8:00 A.M. Meat, eggs or milk; a walk.
10:30 A.M. (The second breakfast) Meat or fish and a
glass of white wine; another walk, a long one.
1:00 P.M. Meat, vegetables and fruit compote.
7:00 P.M. Meat and fruit compote or salad. A glass of
white wine. No other fluid was allowed. Bread was
given sparingly.
102
German See deserves mention for opposing the
limitation of fluids. People were getting sick, became
bedridden as a result. He argued that, on the contrary,
fluids were valuable in weight reduction. He prescribed
a diet of protein and fats, with limited carbohydrate, but
insisted that patients drink gallons of water and hot tea.
Alcohol was prohibited. Today, we impose no fluid
limitation in reducing diets.
The Chambers Reducing System was a bit of a lulu.
He restricted sleep to 7 hours and used Turkish baths
extensively. His program is best described by himself
(in a brief excerpt):
"Day's Regimen for a Three Weeks' Course
Rise at 7:00. Rub the body with horsehair gloves,
have a cold bath, take a short turn in the open air.
Breakfast at 8:00 on the lean of beef or mutton with dry
toast, biscuit or oatcake, a tumbler of claret and water or
tea without milk or sugar, or in the Russian manner with
a slice of lemon. Between meals, exercise as a rule in
the open air, to the extent of inducing perspiration, must
be taken. Running is the best form . . ."
Weir Mitchell found his own unique variation on the
high-protein theme. He relied mainly on rest, an almost
total immobilization of his patients while on a diet of
skim milk, gradually increased to replace other foods
until after a week they lived exclusively on it. Patients
were kept quiet in bed for up to two weeks and afterwards confined to their room, most of the time upon a
couch. This must not have been very difficult since the
regime was so enfeebling one could do little else but lie
around.
Passive exercise in the form of massage was performed
once or twice a day at first; subsequently, the more active
Swedish movements were applied to the extremities. After
4 to 6 weeks the diet was gradually liberalized by the
addition of lean meats and fish, though skim milk still
played a leading role. Mitchell himself conceded
103
that his dietary management was not adapted to persons
leading active lives, or to those unable to devote the
several months required by his restricted regime. He
might have put it that nobody but the idle rich need
apply—also that they had better be of the masochistic
type. (He was a very successful doctor.)
There were others including Doctor Yeo, the famous
nutritionist, who each advanced our thinking about highprotein and dietary procedures. . . . These historical
flashbacks have been offered as evidence that highprotein is indeed not new. Like all fundamental concepts
it has evolved slowly, by experimental trial and error,
and moved forward tiny step by step. Our purpose in this
book has been to integrate these significant data into a
composite theory in the light of modern nutrition. There
remains, however, a last question, an old wives absurdity
about kidney and heart disease, that remains to be
cleared up. Is high-protein harmful?
Hardly. Vilhjalmur Stefansson, the Arctic explorer,
stayed for about nine years on a meat diet. Because he
found it healthy and because no other food was available
to him. He ate huge meals of caribou meat and frozen
fish, mostly raw. His sense of physical and mental wellbeing was at its height during this period. He reported
that not a single case of constipation was observed
among 600 exclusively meat-eating Eskimos over a period of three years. He later wrote books and barnstormed the country on lecture tours to persuade others
of what he had learned. High-protein not only had no
adverse effects, he claimed (and lived by his teachings
into a vigorous old age), it was in fact the key to a truly
healthy and active life.
His findings were strongly confirmed by Dr. William
A. Thomas, a member of the Macmillan Arctic Expedition, after a medical survey of the Eskimos of Northern
Labrador and of Greenland. This report appeared in the
Journal of the American Medical Association of May 14,
1927, excerpted as follows:
"There is no edible vegetation. Their diet includes
104
the meat of whale, walrus, seal . . . numerous sea birds .
. . and finally fish, all eaten usually raw. Contrary to
general opinion, the Eskimo eats relatively little fat or
blubber. This portion is used for its oil in lighting and
warming the domicile . . . With an inadequate supply he
eats everything—including entrails. . .
"These people lead a life of great physical activity . . .
They remain for hours and days in their kaiaks,
separated from the icy water by only a membrane of
sealskin. They frequently alternate between feast (when
they eat to capacity) and famine. In view of this,
together with their extraordinary strength and
endurance, the men often traveling 24 and 36 hours
continuously without rest or food, there can be no other
conclusion than that, under their conditions of life, an
exclusively carnivorous diet does not predispose to renal
or vascular disease."
By renal or vascular he meant: no kidney or heart
ailment; the italicizing of "little fat" was ours, since
high-fat enthusiasts often describe the Eskimos as fat
eaters. A final few words on their raw meat diet. Dr.
Thomas points out, from his own observation and a
close questioning of Danish physicians, that there was
no evidence of any vitamin deficiency, no rickets or
scurvy —the raw meat supplied the necessary vitamins.
One may add sadly that only among the "mission
Eskimos/' taught by civilization to cook their meats, and
with no vitamin-carrying fruits or vegetables available,
do we find these nutritional diseases ravaging the
children.
Are we trying to sell you on high-protein? Avowedly
yes, for we know that its great value for life makes it the
essential base of the human diet, and particularly in
weight reduction. Since it safeguards body tissues while
food is being curtailed, it is the only safe plan. And by
controlling the low blood sugar that creates chemical
hunger, it is the only sure way of reducing—with additional benefits from the 20% bonus of its Specific
Dynamic Action.
Furthermore, though we can point to no statistical
105
show of hands, we believe that the great majority of
American physicians share our conviction of the
primacy of protein in all diet, normal or reducing. What
is a subject of contention is the minimum protein
requirement. We reaffirm our slogan: an optimum of 100
grams for every healthy adult! The reducing diets which
follow will range from a little below 100 up to 175
grams. And no medical argument can be sustained
against this.
We may best approach weight reduction through a
discussion of normal diet, of which the reducing diet is
only a modification, a restriction. Have you ever thought
of getting a normal diet from your doctor, as you would
an ulcer diet? Don't shrug it off. If you have a weight
problem, you almost certainly have a food problem. A
normal high-protein diet should resolve your food imbalance for the remainder of your life, will maintain
your weight after reducing and also your health gains.
A well-balanced diet ought to accomplish the following: preserve and repair your body tissue, furnish sufficient energy for your needs and keep you in good
health. Which is another way of saying it must contain a
proper distribution of protein, primarily, with fat and
carbohydrate, vitamins and minerals, in foods that taste
good and are easily digestible. We have been discussing
food values as abstracts with only a passing glance at the
food sources. But you don't buy, prepare and eat protein
and vitamins. You buy and eat liver (we hope).
Equipped to evaluate their nutritive content, we are now
ready to examine the foods themselves.
There are four basic food groups: milk and its derivatives; meat, including fowl, fish and eggs; vegetables
and fruits; breads and cereals. These are sometimes
presented as the seven food groups, with a separation of
fruits from vegetables, breads from cereals, and a special
place for butter and vegetable fat. This division is made
so that you can work with a rule of thumb in composing
your daily menu, whether for reducing or
106
maintenance: Take some food each day from each of these
seven categories.
The variation from normal in a high-protein reducing
diet lies in its curtailment of sugars, starches and fats and
in the increase of proteins. Which foods shall we sacrifice,
which cut down, which ought we keep or increase? Let us
examine each group in turn to see its place in a normal
diet as well as how it fits into a reducing schedule.
The milk group: This includes all forms of milk, plus
yogurt, cheese, ice cream etc. The daily adult requirement
is one pint, comprising all the forms in which it is taken. If
it is drunk as skim or buttermilk, the allowance can be
doubled or tripled. In a reducing diet, skim milk and
fatless cheese are the easiest, cheapest and most valuable
way of boosting the protein intake. (You may simply say
"cheese" to show your teeth when you're being
photographed, but—) When you buy, make the delightful
discovery of white non-fat cheeses other than "cottage," in
the shape of Ricotta, Brindze, Camembert, skim-milk
Gouda, etc.
The meat group: In a normal high-protein diet there will
be two or more servings each day, including one egg (high
in saturated fat) 3 or 4 times a week, meat and fish daily.
Meats include beef, lamb, veal and pork, fowl and variety
meats. Beef and pork are today too prominent in the
American diet. Learn to favor fowl, cheaper and with less
saturated fat, liver (at least once a week) and other organ
meats like kidneys and sweet-breads. The meats should be
lean, with all visible fat removed, and preferably eaten
broiled or roasted, rarely fried (never, in a reducing diet).
If you wish to stew or pot the meat, refrigerate after
cooking and skim off the congealed fat.
Fish is interchangeable with meat as a Grade A
protein source and it demands a bigger role in your
diet. Fish and all sea food are highly unsaturated. They
can be used fresh and smoked, pickled or canned. The
dieter should be wary of fish canned or prepared with
107
oil. In cooking, it can be boiled, broiled or baked, should
rarely be fried (never, in a reducing diet). Most fish has a
much lower calorie value than equivalent meat and can
be eaten less sparingly.
Vegetables: Part of your daily vegetable allowance
should be eaten raw. Low-calorie raw vegetables which
offer good bulk to the dieter are today available in all
seasons. Make a simple salad using herbs instead of oil;
when "normal" again, you can toss with vegetable oil.
The choice and quantity of cooked vegetables will be
limited by the severity of your diet. Include, if possible,
one green and one yellow vegetable daily. Eat legumes
(peas, beans and lentils) for their high-protein; avoid
high-calorie root foods and tubers while reducing, except
for carrots and, occasionally, potatoes. Braise vegetables
or cook speedily in a minimum of water which must not
be poured off since it contains the natural salts. Pressure
cooking is preferable—do not add fats while you are
reducing.
Fruits: These should be served fresh, or baked, with
no sugar added. At least one citrus fruit or juice daily.
Fruit juices should likewise be left unsweetened. If you
feel you must, use saccharine or sucaryl (millions have
learned to take their fruits as well as their beverages
without sweetening, real or artificial). The calorie values
of the common fruits and vegetables are shown in the
Appendix, where they are listed in percentage groups.
This will enable you to make substitutions in menu-making. Obviously, a cup of a 5% fruit or vegetable is equal
to a half cup of any 10% group, and so on.
Breads and cereals: A normal diet should allow for
several (2-4) slices of bread or its interchangeable
equivalent in cooked cereals. These should be whole
wheat and whole grain rather than "enriched" or "restored." There are obese persons who claim they eat little
bread but who more than compensate by nibbling on
crackers, wafers, zwieback, etc. This staff of life is a
pretty wobbly crutch—don't lean on it. Besides, bread by
any other name is starch. Even "very thins" are no
108
reducing aid. As for gluten breads, unless you are diabetic you do not need them. Though they claim to be
high-protein, it is not of high biological value. They can
cause diarrhea and are known to be trouble makers in
certain intestinal conditions.
Desserts: In reducing, these are strongly tabooed in
the shape of ice cream, pastries and such. Since "something sweet" does serve a digestive purpose at the end of
a meal, eat fresh or baked fruit. Once on your maintenance diet, puddings and cakes with low-fat, lowsugar frosting may be restored to the menu. Vintage
cheeses too can be taken back, but as they are concentrates of whole milk use only occasionally and sparingly
—a soupcon is as good as a bite.
Seasonings: These are usually without caloric value
and can be used freely. There is no need to limit salt in a
reducing program. The weight thus lost is fluid, not fat;
drying out the body serves no purpose. You will not
need rich sauces and-gravies when you know how to use
herbs on meat, fish and vegetables. Garlic salt, vinegar,
mustard, paprika, basil, thyme, curry, dill and nutmeg,
each adds its distinctive flavor to cookery. The pleasure
you have derived from eating need not be sacrifìed
during weight reduction. Seasonings help.
Snacks: If you are used to snacks, you may have
bouillon, clear defatted consommé, tea or coffee (without sugar). You can save a fruit or some raw vegetables
from your daily allowance. Fruit or tomato juice is always refreshing.
Alcohol: is (absolutely) prohibited during weight
reduction; once "normal" again, you can release the
brake in moderate imbibing. Wine or a cocktail adds
zest to a meal. But recognize it as part of your "food"
intake, as the alcoholic does whose body craves less and
less food as alcohol comes to replace it. If you have a
tendency to obesity stay shy of alcohol, for its rapid and
almost complete absorption makes you very vulnerable.
Dietary Do's and Don’ts: To most dieters alcohol is
109
less dangerous than the innocuous-appearing soft drinks.
Avoid sugary sodas, colas, pop and all foods containing
hidden sugar such as prepared (dry) cereals and canned
fruits (except dietetic fruit). Eat no rolls, biscuits, etc.
usually containing sugar and fat. Don't wreck your
reducing schedule by "coffee and" breaks and by careless lunching. Eat slowly, make your food last, take
small bites and drink plenty of water. This concludes
our food pointers, a good deal of which you probably
knew before. Reading it as part of a reducing program,
however, may be of some value.
110
Chapter VII
PICK YOUR OWN DIET
WE ARE finally on top of our problem: how to
compose a reducing diet. We suggested earlier that,
given an understanding of nutritional values and the
necessary data in food tables, you yourself could make
up your diet. Let us see how one goes about it.
The key to our high-protein diet is to find and blend
that combination of foods which will give us the
greatest protein value at the lowest caloric cost. How
many food calories do you need? Are you a man or
woman, what is your age, occupation and your basal
metabolism? Your caloric requirement is the sum of
your energy expenditure at work and in recreation, plus
the internal energy consumption of your life process.
In a sense, there is no such thing as a normal diet,
though we have been talking about it. There is only your
normal diet and, consequently, your reducing diet. Yet,
as with all so-called norms, we can set up a mythical
average man and woman. And we say: the average man
requires 3,000 calories; the average woman requires
only 2,400. You will be shown how to find your own
variation from this norm so you can fix on a reducing
diet that meets your special needs.
To help you pick your diet we present not a single
formula but three, offering a wide range in protein content and caloric value.
Diet I contains somewhat under 100 grams of protein
111
and from 1000 to 1200 calories (notice our caloriecounting vagueness). It is recommended for those requiring the severest restriction in their food intake
because of sedentary occupation, lack of exercise, or
their low rate of food-burning. It makes an ideal starter
for the inactive woman.
Diet II contains from 125 to 135 grams of protein and
1350 to 1550 calories, averaging at around 1400. It is
suitable for the more active female, the moderately
sedentary male and the inactive teen-ager who requires a
reducing schedule.
Diet III raises the protein intake to 150 to 175 grams
and the calories to 1700 to 1900, averaging 1800
calories. It is intended for the physically active male and
the active teen-ager who requires only a slight food restriction.
Which of these three dietary plans should you follow
—how long ought you stay on it—how will you make
your own adjustment? Any one of these allows you
fewer calories than you now expend, unless you have
been starving yourself. How big a calorie deficit you
must create depends upon how much weight you need to
lose and at what rate.
Glance once again at the two weight charts. You
should aim to reach normal standards and then go below
them as close as you can come to your ideal weight. Let
us say that this entails a loss for you of 30 pounds.
To guard your health and to be able to perform your
daily job, you ought not lose more than two pounds a
week. Your weight reduction schedule should therefore
extend over not less than 15 weeks. Put up a weight
chart next to your bathroom scale, weigh yourself at
weekly intervals (in the beginning, at least) to check on
your progress. If you are losing weight too rapidly on
Diet I, or on II, switch upward in the protein-calorie
range; if not fast enough, restrict yourself further. Find
that diet which gives you the most desirable rate of
weight loss.
112
It has been estimated that a gram of fat is equivalent
to 9 calories; thus, 450 grams (one pound) equals approximately 4100 calories. To lose two pounds of body
fat a week, you must create a deficit of around 8200
calories.
Let us suppose that you are the average working man
and require 3000 calories per day. If you were to place
yourself on the 1800 calorie Diet III, you would be setting up a daily deficit of 1200 calories and a weekly
deficit slightly exceeding the 8200 calories. Your body
would then mobilize its fat to provide the deficient
energy and you would thereby lose two pounds. You
certainly wouldn't feel starved on your food ration.
There are no special gimmicky foods to buy, it is easily
memorized and experience has shown it to be satisfying.
If you are an average woman, you require about 2400
calories per day. Following the most severe Diet I
would result similarly in a 1200 calorie daily deficit and
in a weekly two-pound loss. This may sound too pat but
it isn't just paper theory. It works—on one condition —
that you work along with it.
Diet II is designed as a compromise and a stepping
stone between the two extremes, for moderately overweight women who don't need to lose too much (and for
the more active ones), and for sedentary men who find
Diet I too restrictive. It should give these persons the
same weight loss of around two pounds.
We start with Diet I. Below are given the daily allowances expressed in terms of the seven basic food groups
in a normal diet. Proteins are kept as high as is allowed
by the calorie restriction. Fats and carbohydrates have
been reduced but minimum requirements are met. To
permit you a variety of fruits and vegetables, substitutions are suggested. In the Appendix you will find fruits
and vegetables arranged in calorie percentage tables, in
groups so that one serving of List A approximately
equals 1/2 serving of List B, or 3 serving of List C, or w
serving of List D.
113
Daily Allowances in Diet I
1. Skim milk or buttermilk or yogurt
2. Meat (lean), poultry or fish
3. Bread
or
4. Cereal (substitution for 1 slice)
5. a) Vegetables, yellow, "List B"
1 pint (2 cups)
10 ounces, raw,
or: 8 ounces, cooked
2 slices
1/2 cup, cooked
1/2 cup
Vegetables, green, "List B"
1/2 cup
(Substitute, as desired, List A, C, or D,
according to percentage values— see Appendix)
c)
Vegetable salad with non-fat dressing
at least 2 servings
(as much as desired)
6. Fruit "List B"
2 servings
7. Butter
1 small pat
or
Unfortified, unsaturated margarine
1 teaspoonful
b)
It will be simple to remember if you think of fruit
juice, toast, cottage cheese or egg and coffee for breakfast; meat or fish, a vegetable salad and a slice of bread
for lunch; meat, vegetables and fruit for dinner; plus
skim milk for a snack—unsweetened coffee or tea is not
restricted.
Diet I is fully outlined on the following page. In the
Appendix we offer a week of Diet I sample menus to
serve you as a guide. You may follow all or any of them
or use them to adapt your own menus. You should not,
however, take a breakfast from one day and a lunch or
dinner from another. Foods have been intentionally
blended so that, for example, any one lunch may cost
more in calories than another, but the daily calorie totals
are approximately the same. You can freely make your
own substitutions of fruits and vegetables, using the
percentage tables.
Diet II goes up moderately in calories, due solely to its
higher protein allowance. If you have maintained
yourself for a time on Diet I and wish to advance to Diet
II, notice that it offers an additional 4 ounces of meat and
one tablespoon of cottage cheese (or their protein
equivalents).
114
DIET I
1000-1200 Calories
Protein—90-100
Grams REDUCING DIET WITH SEVERE CALORIC RESTRICTION
BREAKFAST:
Cottage cheese
or Egg (medium)
Bread, whole grain
Butter or Fortified Margarine
Skim milk
Coffee or tea
No sugar
Use milk ration here, if you so
desire
Citrus fruit juice
2 tablespoons
1
1 slice
1 small pat
1 glass
as desired
1/2 cup
LUNCH:
Meat or Fish
Vegetable Salad
No dressing except vinegar and
herbs
Bread
Coffee or tea
1 serving (4 ounces cooked)
4" x 3" x 1/2"
(roughly the size of a
slice of white bread)
large serving
1 slice
as desired
DINNER:
Meat or Fish
Vegetable Salad
Hot Vegetable
1 serving as at lunch
(4 ounces cooked)
1 large serving
1/2 cup green
Fruit
1/2 cup yellow
1/2 cup cooked
Coffee or tea
OR 1 small raw
as desired
BED-TIME SNACK
Skim milk or yogurt
1 cup
How to know when to make the change-over from
Diet I? When" you discover you are losing more than
two pounds a week. Or if you feel that Diet I is inadequate (you're constantly hungry). Or when you are
115
DIET II
1350-1550 Calories
Protein—125-135 Grams
REDUCING DIET WITH MODERATE CALORIC RESTRICTION
BREAKFAST:
Cottage cheese or its equivalent
Bread, whole grain
Butter or Fortified Margarine
Skim milk
Coffee or tea
No sugar.
Use milk ration here, if you so
desire
Citrus fruit juice
3 tablespoons
1 slice
1 small pat
1 glass
as desired
1/2 cup
LUNCH:
Meat or fish
1 serving (4 ounces cooked)
4" x 3" x 1/2" (roughly the
size of a slice of white
bread)
Vegetable salad
Bread
Coffee or tea
large serving
1 slice
as desired
DINNER:
Meat or fish
Vegetable salad
Hot vegetable
·
2 servings as at lunch
(8 ounces cooked)
large serving
1/2 cup green
1/2 cup yellow
1/2 cup cooked
Fruit
OR 1 small raw
Coffee or tea
as desired
BED-TIME SNACK
Skim milk or yogurt
1 cup
10-15 pounds away from your ideal weight and want to
slow down your weight loss.
Diet II is shown on the following page and a week of
suggested dietary menus based upon it appear in the
Appendix.
Diet III, for the physically active male and the teen116
ager can also serve anyone requiring but a slight restriction in their food intake. We have added here (to Diet II)
an extra slice of bread and another 4 ounces of meat. It
also permits dietary variations, including a heavier
breakfast or a good-sized dinner, as you may see by the
sample menus in the Appendix. For both men and
women who have been following a
DIET III
1700-1900 Calories
Protein—150-175 Grams
REDUCING DIET WITH MILD CALORIC RESTRICTION
BREAKFAST:
Cottage cheese or its equivalent
Bread, whole grain
Butter or Fortified Margarine
Skim milk
Coffee or tea
No sugar.
Use milk ration, here if you so
desire
Citrus fruit juice
3 tablespoons
1 slice
1 small pat
1 glass
as desired
1/4 cup
LUNCH:
Meat or fish
1 serving (4 ounces cooked)
4" x 3" x 1/2" (roughly the
of a slice of white
size
bread)
Vegetable salad
Bread
Coffee or tea
large serving
2 slices
as desired
DINNER:
Meat or fish
Vegetable salad
Hot vegetable
3 servings as at lunch
(12 ounces cooked)
large serving
1/2 cup green
Fruit
1/2 cup yellow
1/2 cup cooked
Coffee or tea
OR 1 small raw
as desired
BED-TIME SNACK:
Skim milk or yogurt
1 cup
117
more severe diet, it can be a stepping-stone to a normal
non-restricted high-protein diet. The protein allowance
is more than ample. If you have come close to your ideal
weight, you can afford this liberality. You are now only
600 (female) or 1200 (male) calories short of the average 2400 or 3000 calories requirement. With your
weight record as meal ticket, these extra calories are
henceforth carte blanche, as you desire them.
We have not calculated any of the diets on a strict
calorie basis, you may have noticed, but neither have we
lost sight of their values. Nor should you, though you
are not expected to weigh food or count calories. These
diets are designed for practical use. Simply follow
through with household or eye measurements. Adhere to
your chosen diet with firmness yet without rigidity. If
you at any time require extra food, increase the protein:
the skim milk, cottage cheese, fish or meat. The more
steadfast, however, the faster you will see those
rewarding body changes.
No meal-skipping, please! Don't try short cuts. Fasting
is no way to lose weight. From our discussion of starvation you may recall one physiological argument against
it. If too long a time elapses between meals, your body
will live on its stored fat, all right, but also on your
muscle protein. During sleep this does not take place as
the energy requirement is minimal..
Another consideration is that the liver is put under
stress to keep a proper blood sugar level. Also, due to
the mobilization of body fat and its incomplete oxidation, the kidneys are overworked to eliminate toxic
substances. Finally, the metabolic heat which helps in
burning body fat is actually reduced by fasting. Don't.
Short-cutting undermines the whole psychology of scientific weight reduction.
You are now armed to undertake your campaign. Dc
not underestimate that sly and slippery enemy—fat Your
diet is your beachhead—but remember as you sail) forth
that you are in a two-front engagement. We have
118
repeatedly urged you towards vigorous exercise. Let
us now run through some of its pros and cons.
It is estimated that replacing one sedentary hour per
day, spent in reading or TV watching, by an activity
such as brisk walking will expend about 300 calories.
Tennis, swimming, horseback riding, etc. almost double
this calorie loss. You can see, mathematically, that over
the period of a month you may lose several pounds
through exercise alone. Of even greater value to you,
you will be replacing lost fat with new muscular tissue.
An optimum replacement is considered to be one pound
for each five pounds of lost weight.
This being said in our role of nutritionist, medically
we must warn you of certain dangers. If you are a
woman working at a desk, a homebody without stairs to
climb and old-fashioned housework to do, or a man
whose only carrying and lifting is figures onto paper—
and if you are somewhere past adolescence (say, around
40)—be careful.
Muscular exercise makes enormous demands on the
heart and blood vessels as well as on the respiration. In
strenuous exertion the heart, which normally pumps
about three quarts a minute, may have to raise its working rate to as high as twenty quarts. The lungs which
ordinarily supply about a cup (8 ounces) of oxygen per
minute must now provide over a gallon (128 Ounces).
The body fulfills the demands upon it by deeper and
more rapid respiration, by a faster heart beat, by a
greater amount of blood pumped per heart stroke, by an
increase in blood pressure and by complex nerve reactions. The rate of fuel burning is of course greatly accelerated.
The human body has to be conditioned for violent
exercise. A boxer, considered old at thirty, undergoes
rigorous training to be able to take the strain on his heart
and lungs during a ten-round bout. We do advise, then,
the most strenuous exercise compatible with your age,
general activity level and your present health. Do not
become a Sunday athlete.
119
You who may be unfit for cycling or mountain climbing, don't take to a rocking chair. There is a lot you can
do without becoming over-fatigued or short-winded. Try
long walks, gardening, bowling, golf, or graded settingup exercises such as are given on radio and TV. Even
simple deep-breathing exercises are beneficial. Start
with a few minutes of any activity and gradually prepare
your body to take an increasing work load. Do it daily
—don't over-do.
You are not only consuming calories. Both the circulatory and respiratory systems will increase their
efficiency. You will through this develop and maintain a
reserve strength which may one day pay off handily in a
large dividend. You will become better able to withstand
any possible overload on the heart, lungs and blood
vessels during illness, a physical emergency, or when
necessary, under surgery. Finally, your improved health
can make the aging process a slower, more graceful one.
To return to the reducing diet itself, imagine happily
that you have come within sight of your ideal weight—
what is next? You now feel comfortable, slim and
healthy. Your body has reached a balance point and you
are now ready to normalize your eating. This is the
critical time. You may have won the battle and yet fritter
away the victory. Weight reducing, like war, is dramatic
but the drama is over and life begins again. How will
you stand up under it?
We believe that you will have built up the necessary
self-discipline to maintain your weight loss through
good nutrition, along with the essential know-how to
choose foods for their true values. You will also have
established eating and exercise patterns as a way of life.
Now that your weight is A-OK, increase your daily allowances but keep the high protein base. Make sure to
eat daily of the seven food groups outlined under Diet I.
You will, as a matter of habit, continue to balance the
daily meals of your maintenance diet without having to
think about it.
We have a few final suggestions. One significant re120
form you can make is to give a larger place to breakfast.
Your morning meal should offer you about one-third of
your daily protein and calories—does it now? We presume you have been hearing about the value of a good
breakfast and have probably, like most persons, ignored
it. There is a perverse Gresham's Law operating in the
market place of ideas. So much cheap clap-trap passes for
currency, it drives the few valuable ideas into hiding.
Why do we insist upon a substantial breakfast? Experimental studies have been repeatedly carried out
among University groups. We have learned that student
(working) efficiency is greatly increased by a high-protein
breakfast for a period lasting up to five or six hours. The
greatest efficiency followed a breakfast including two
eggs or beef and skim milk. We needn't repeat here the
physiological meaning of this in terms of blood sugar
levels.
The downgrading of breakfast among us starts in
childhood. Studies of school children in Pennsylvania and
other states show that about one child in three had .
skipped at least one breakfast that week, and that only two
in five had enjoyed a good breakfast. What a waste this
must represent in school learning across the nation.
Granted that, more than any other people, we live by
the clock. If you simply don't have the time for a large
breakfast at home, allow for a second breakfast (not a
coffee snack) to supplement the first. If you have no
appetite in the morning, it only indicates that you probably overate the night before. Most persons save their
appetite for the dinner hour when they eat everything. The
trouble is that your body just doesn't work in that way.
Our mothers and grandmothers, if they were raised on a
farm, knew the value of a high-protein breakfast. In the
Scandinavian countries and in Holland (at least up to our
last visit there—American industrial rhythms are being
exported everywhere), breakfast is composed of an
appetite-exciting variety of smorgasbord and wurst meats,
respectively. While in countries like France and
121
Italy, where the negligible continental breakfast is
served, dinner is traditionally eaten and enjoyed in a
mid-afternoon break. Only here do we starve our bodies
throughout the day and overload them at night.
Proper preparation, seasoning, cleanliness, eye appeal
and pleasant surroundings are also important to good
nutrition. What the eye sees, the stomach senses. We
have previously touched rather hastily on what happens
to a ham sandwich bite. Let us expand a little on the
fascinating subject of the human gut.
Imagine man as a complex tube with an outer layer of
skin and appendages and for the inner lining the mucous
membrane of his intestinal tract. We frequently keep the
upper end of this tube wide open and the lower end
insufficiently so. Food in passing through the tube is
broken down by digestive secretions of various enzymes
into its constituents, which are then taken up by the
blood and lymph capillaries in the process of assimilation.
Food remains for 4-6 hours in the stomach where it is
prepared by its juices for floating down the alimentary
canal. About four hours later, the food-intestinal juice
mixture or chyme reaches the end of the small intestine
where it remains for about an hour. During this entire
time, absorption from the small intestine into the blood
stream takes place. What remains now enters the large
intestine or colon. The entering fluid starts a churning
back and forth, water is absorbed and, finally, soft solid
waste forms.
The entire colon keeps secreting mucus which acts as
a lubricant. The stool has thus started to form about nine
hours after eating. It will take about another nine hours
for it to pass through the bowel into the pouch-like
rectum. When distended, this sends a message to the
brain interpreted as an urge to evacuate.
The various secretions and movements are all automatic, without our direct control. Still, we do have a
small say-so, for the timing and amounts of secretion are
in part influenced by more or less external factors
122
subject to our intelligence. They vary with our
emotional stress at the moment, how rapidly the food is
eaten, how it tastes, and our environment.
Apparently, the only place where we have full control
is at the upper end of the digestive tube, in the foods we
eat. Let us put in valuable and good tasting things at the
proper time and in a congenial atmosphere, so that the
body will find along the way what it needs for
functioning, with an adequate residue left over to satisfy
the lower end. In a word—eat sensibly to keep fit.
A few summing-up suggestions on sensible eating
may be in order:
1. Set the mealtime aside as a time for relaxation.
2. Don't eat when you are emotionally upset.
3. Eat in clean, pleasant surroundings.
4. Develop good food habits—eat on schedule,
slowly; chew your food.
5. Eat nothing too hot or too cold. Remember how
the young mother is taught to test the baby bottle on her
own skin. Your insides are tender too. Take nothing in
so
hot or icy you couldn't keep your finger in it.
6. Eat moderately, even after you reach
normal weight, if you want to stay slim and healthy.
7. Apply, for the rest of your life, the knowledge you
have gained through weight reduction.
The rewards are great. Every word you have read here
sums up to this conclusion. It is always a joy to see
"youngsters" in their seventies and eighties, who not
only had the foresight to pick the right genes but who
have maintained their stamina, still dancing, golfing
and, often working. One cannot help but admire their
alive interest in everything, their mental and physical
durability.
A high-protein diet will help you to this spirited health
that persists into old age. How shall we define such
health? It is primarily expressed in vitality, a zest for life
in a well-functioning and handsome body, with little
fatigue or irritability under stress. There are few
disturbing symptoms. There is effective resistance to
123
infection or disease and rapid recovery. It assures a
prognosis of blessed longevity.
High-protein produces these effects by offering the
body the raw materials it needs for its tissues and processes. It is the body's blood bank upon which it draws
daily to produce its red and white cells. It is the storehouse from which disease-fighting antibodies are drawn.
It makes possible daily well-being and working efficiency.
Whether you are young with the need to grow, aging
and wish to maintain your body structure, sick and went
to recover your strength, normal and hoping to stay that
way, thin and ought to gain weight—or overweight and
have to lose poundage healthily, protein is your dish.
Try it and see.
124
Chapter VIII
CHEMICAL HUNGERALCOHOLISM—BACKSLIDNG
WE SAID earlier that we need offer no reducing gimmick or magic formula because the truth about highprotein was in itself wonderful enough. In this brief concluding chapter let us re-state and fill in this significant
truth: A high-protein diet is the only safe reducing
program because it protects the body tissue. It is the
only sure program because it kills the false appetite of
chemical hunger.
Excluding the hidden psychological or emotional factors, why do you overeat and on what? You are left
unsatisfied at the table; an emptiness gnaws at your
insides. You need coffee breaks for a lift and the cruller
helps. Your sweet tooth aches for a chocolate bar. You
get a sudden yen for a soda, that pint of ice cream (or
fifth of scotch.)
But why—because you're plain hoggish? No more
than the undernourished child at school is stupid or lazy.
Or the alcoholic is morally depraved.
The analogy with alcoholism (between overeating and
overdrinking) is tight enough to warrant some exploration for the light it can throw on obesity. Alcohol is a
molecule composed of carbon, hydrogen and oxygen,
the very elements that compose sugars and starches.
Overeating and alcoholism may each serve various
psychological ends. In both, the craving for food or for
alcohol
125
substitutes for an unsatisfied craving for love—the infantile oral (feeding) satisfaction replacing adult sexual
gratification.
Alcoholism is essentially psychological, according to
psychiatrist Charles H. Durfee. It represents a flight from
reality of a maladjusted personality. Dr. Durfee also
discusses the role that habit plays in the routine drinking
of the problem drinker—paralleling the habitual
overeating of the typically obese.
The question remains: why does individual A seek an
escape in drink and become its victim while B, under
similar stresses, bites her nails or becomes a bridge
fanatic? The past two decades have seen a growing
tendency to lay aside the psychological causes and to
treat alcoholism as a physical disease, deriving from a
metabolic or glandular imbalance.
Dr. Roger H. Williams, director of the Biochemical
Institute of the University of Texas (who discovered
pantothetic acid), first urged the use of vitamins in the
treatment of alcoholism. Successful cures have since
been reported in various quarters from massive dosages
of vitamins.
The glandular view is upheld by leading authorities,
several working closely with the AA. They assert that
alcoholism is produced by a deficiency of certain hormones, possibly related to a malfunctioning pituitary.
They and others have claimed phenomenal cures following the injection of hormone extracts such as cortisone.
Dr. E. M. Abrahamson broke fresh ground in his
valuable study "Body, Mind, and Sugar." His theory of
alcoholism is that its underlying condition is a "chronic
partial blood sugar starvation. The alcoholic craving may
be for sugar . . . the immediate effect on the body of a
dose of alcohol is essentially that of a dose of pure
sugar."
He notes that the alcoholic's let-down feeling is induced by a drop in his blood sugar and that immediate
relief is given by the first drink. In his treatment he
126
found amazingly that a diet change which raised the
blood sugar level cured the alcoholic. "When the drop in
blood sugar was eliminated, he was able to resist the
urge."
Notice the close parallel of alcoholic thirst, related to
blood sugar starvation, with chemical hunger (a craving
beyond normal animal appetite) likewise caused by low
blood sugar. We are not disregarding the psychological
factors in overeating. But their treatment is hazardous
and may entail a substantial overhaul of the personality.
It is far more feasible (as in alcoholism) to treat directly
the symptoms that lead to overeating and obesity, the
blood sugar chemistry.
Our blood sugar level is maintained at a balance by
the interplay of insulin secreted in the pancreas, which
converts excess glucose into glycogen, and the adrenal
cortical hormones which reconvert the glycogen (stored
in the liver and muscles) into glucose as it is needed.
And it is needed continuously by the brain, serving as its
only food; and by the muscles, or we feel body fatigue;
and in the blood stream where its lack is translated by
the brain as hunger.
We earlier saw in the hypoglycemia cases of Mrs.
Smith and Mr. Jones how an oversensitive blood sugar
mechanism, pouring excessive insulin, can be stabilized
by the slow-feeding of the essential glucose in a highprotein diet. These patients were thereby able to reduce
successfully while recovering their health. The highprotein, in addition, made dieting easier by curbing their
pangs of chemical hunger.
There is a final problem we ought to face before
signing off, for it is the Achilles' heel of many a
reducing program-backsliding. We are convinced that
once self-discipline has been asserted over the early
dietary period of habit formation, your re-educated palate
will let you live with your new schedule. And you will no
longer feel a need to overeat. It is common knowledge
127
that at normal blood sugar levels the excessive craving
for food, especially for sweets, usually disappears.
And still . . .Dr. W. Hamburger of the Dept. of
Psychiatry of Strong Memorial Hospital warns that
obese patients tend to rebel against any reducing regime.
They backslide particularly when "they feel blue,
sexually frustrated or apprehensive."
The temptation to eat of the forbidden fruit which once
exiled man from Eden lies deep in our psyche. The mind
also tends to hug the memory of a pleasure that has been
experienced. The tabooed food by its very repression
may come to loom large in the imagination. This may
build up tension which is detrimental to healthy
reducing. Question: Should the dieter resist at all costs or
surrender gracefully?
We find (as expected) two opposing views of dietary
discipline. Dr. Norman Jollifïe, Director of the Bureau of
Nutrition of the N.Y.C. Dept. of Health, argues that even
"very small lapses . . . lead to difficulty. Many cheaters
reduce at greater cost to will power and self-denial."
There are individuals who can turn their backs upon a
vice without regret. For others, and we see this often in
alcoholism and in juvenile or adult delinquency, there is
the danger that a single fall from grace may bring on a
feeling of worthlessness and a kicking over of the traces.
This is the guilt-shame syndrome. Having "sinned" by
taking that chunk of chocolate cake or the first drink, he
must choke down his remorse by gorging himself on the
rest of the cake or of the bottle. And farewell to reform!
Our own view of backsliding is a more relaxed one. If
a disallowed food tempts you to break your regime, eat
and don't be damned. You'll probably find it didn't taste
a bit as delicious as you imagined it. And you will suffer
only a minute setback, so long as you return quickly and
safely to the fold.
Most of you will discover that, without the gnawing in
your gut of chemical hunger, you can stare down the
128
seven layer cake or banana split (and maybe that bottle
of bourbon) without flinching. We can therefore predict
with fair assurance that your reducing diet will be
successful and your weight maintenance without peril.
Reducing is no fun but it can be painless, and it ought to
be a memorable and rewarding experience. And now —
though we rely on science rather than on chance—we
wish you good luck in your adventure.
129
APPENDIX
DIET I Menu for Sunday
BREAKFAST
Honeydew
1/8 small
Egg, soft-boiled
1
Oatmeal, cooked
1/2 cup
Skim milk
1 glass
Coffee or tea
as desired
LUNCH
Chopped liver
Lettuce and tomato
slices
Bread (whole grain)
Clear vegetable soup
Tea (no sugar)
DINNER
Tomato juice
Steak, broiled
Tossed salad
Broccoli
Zucchini squash
Grapefruit sections
Coffee or tea
large ball
large portion
1 slice
1 serving
as desired
4 ounce glass
small portion (4 "x 3" x 1/2")
large portion with 1/2 table
spoon French dressing
3 stalks
1/2 cup
1/2 cup
as desired
133
DIET I
Menu for Monday
BREAKFAST
Orange juice
Egg, poached
Bread (whole wheat)
Butter
Skim milk
Coffee or tea
LUNCH
Filet of Sole, broiled
String beans
Carrots
Bread
Buttermilk or yogurt
DINNER
Chicken, broiled
Asparagus
Cauliflower
Vegetable Salad
Apple, raw or baked
Coffee or tea
BED-TIME SNACK
Skim milk
1/2 cup
1
1 slice (toast or plain)
1 small pat
1 glass
as desired
small portion (size of slice
white bread)
1/2 cup
1/2 cup
1 slice
1 cup
1 quarter (21/2 lb. chicken)
1/2 cup
1 cup
large portion (herb dressing, no oil)
1 medium
as desired
1 glass
134
DIET I
Menu for Tuesday
BREAKFAST
Grapefruit juice
Cottage cheese
Bread (whole grain)
Skim milk
Coffee or tea
1/2 cup
2 level tablespoons
1 slice
1 glass
as desired
LUNCH
Broiled beef patty
Cole slaw
Peas and carrots
Bread
Coffee or tea
1 large
1/2 cup
1/2 cup
1 slice
as desired
DINNER
Fish roll-ups in Creole
Sauce
Collard greens
Potato, baked
Butter or Fortified
Margarine
Salad greens (Bleu
cheese dressing)
Skim milk or
buttermilk
135
5 ounces of fish
1/2 cup
1/2 large
1 small pat
1 portion
1 glass
DIET I
Menu for Wednesday
BREAKFAST
Wheatena, cooked
Skim milk
Egg, shirred
Tangerine
Coffee or tea
1/2 cup
1 glass
1
1 large
as desired
LUNCH
Cold cuts
3 slices (4" x 3" x 1/8")
Size of slice white bread
Salad: radishes, sour
pickle, lettuce,
tomato
Bread (whole wheat)
Apple
Coffee or tea
large portion
1 slice
1 medium
as desired
DINNER
Clear broth
Roast beef
Cucumber salad
Spinach
Brussels sprouts
Fresh fruit cup
Coffee or tea
1 cup
1 slice 4" x 3" x 1/2"
large serving
1/2 cup
1/2 cup
1/2 cup
as desired
BED-TIME SNACK
Skim milk
1 glass
136
DIET I
Menu for Thursday
BREAKFAST
Pineapple juice
Lean meat cold cut
Bread, whole grain
Skim milk
Coffee or tea
1/3 cup
1 slice, 1/8" thick
1 slice
1 glass
as desired
LUNCH
Farmer cheese
Hot vegetable plate:
spinach, collard
greens, carrots
Egg, soft-boiled on
greens of vegetable plate
Potato, mashed
Skim milk
DINNER
Liver, broiled
Vegetable salad
oil or mayonnaise
String beans
Mushrooms
Strawberries, fresh,
unsweetened
Coffee or tea
4 ounces
1 large serving
1
rounded tablespoon
1 glass
1 slice 4" x 3" x 1/2"
large serving
1 teaspoon
1/2 cup
1/2 cup
1 cup
as desired
137
DIET I
Menu for Friday
BREAKFAST
Grapefruit, unsweetened
Cottage cheese
Bread, whole wheat
Skim milk
Coffee or tea
1/2
2 level tablespoons
1 slice
1 glass
as desired
LUNCH
Salmon, canned, waterpack with lemon
and parsley
Garden salad (lettuce,
tomato, cucumber,
radish, green pep
per, celery)
Bread, thinly buttered
Coffee or tea
4 ounces
large serving
1 slice
as desired
DINNER
Clam and tomato juice cocktail
equal parts tomato
juice and clam juice
4 ounces
Codfish steak, broiled
1 portion 4"x4"x1/2"
Tomato, broiled
1
Turnip greens
1/2 cup
Broccoli
3 stalks
Pineapple, fresh
1/2 cup cubed
Coffee or tea
as desired
BED-TIME SNACK
Skim milk or yogurt
138
DIET I
Menu for Saturday
BREAKFAST
Orange, medium
Omelet
Bread, whole wheat
Coffee or tea
1
1 egg, use skim milk
1 slice
as desired
LUNCH
Chicken or turkey,
sliced
Tossed salad
Bread
Coffee or tea
1 portion 4"x4"x 1/2"
1 large portion
1 slice
as desired
DINNER
Clear broth
Roast beef
Eggplant, baked, sea
son to taste
Kale
Cauliflower
Applesauce
Coffee or tea
BED-TIME SNACK
Skim milk
1 cup
1 slice 4"x3"x2"
1 cup
1/2 cup
1/2 cup
1/2 cup
as desired
1 glass
139
DIET II
Menu for Sunday
BREAKFAST
Orange juice
Egg, poached
Bread, whole wheat
Butter (or margarine)
Skim milk
Coffee or tea
1/2 cup
1
1 slice (toast or plain)
1 small pat
1 glass
as desired
LUNCH
Chef salad
Mixed cold cuts
Bread
Skim milk
large portion
3 slices 4"x3"x1/8"
1 slice
1 glass
DINNER
Turkey, roast
large portion (4 slices
4"x3"x 1/4")
Hearts of lettuce,
herb dressing
Carrots
Zucchini
Fresh fruit cup
Coffee or tea
large portion
1/2 cup
1/2 cup
1/2 cup
as desired
140
DIET II
Menu for Monday
BREAKFAST
Grapefruit juice
Buckwheat groats
Farmer cheese
Skim milk
Coffee or tea
LUNCH
Eggs, hard-boiled
Garden salad
Yogurt
Berries, frozen or fresh,
unsweetened
Bread
Coffee or tea
1/2 cup
1/2 cup cooked
2 ounces
1 glass
as desired
2
1 large serving
1 cup
small portion (to go with
yogurt)
1 slice
as desired
DINNER
Liver, broiled
Kale
Asparagus
Tomato, broiled
Grapefruit
Coffee or tea
2 slices 4"x3"x1/2"
1/2 cup
1/2 cup
1
1/2
as desired
BED-TIME SNACK
Skim milk
1 glass
141
DIET II
Menu for Tuesday
BREAKFAST
Pineapple juice
Cold cuts, lean meat
Bread
Skim milk
Coffee or tea
LUNCH
Cottage cheese
Fruit salad containing
2 peach halves, with
large amount of lettuce
Bread
Butter (or margarine)
Buttermilk
DINNER
Filet of sole, broiled
Tomato aspic
Mustard greens
Cauliflower
Applesauce
Skim milk
1/3 cup
4 slices (4"x3"x1/8")
1 slice
1 glass
as desired
3 tablespoons
1 serving
1 slice
1 small pat
1 glass
1 large serving (1/2 to 3/4 lb.)
1 serving
1/2 cup
1/2 cup
1/2 cup
1 glass
142
DIET II
Menu for Wednesday
BREAKFAST
Grapefruit
Cottage cheese
Bread
Butter (or margarine)
Skim milk
Coffee or tea
1/2
3 level tablespoons
1 slice
1 pat
1 glass
as desired
LUNCH
Meatballs
6 average (5 ounces raw
meat)
Spaghetti or macaroni
Tomato sauce
Lettuce and tomato
salad
Skim milk
1/2 cup, cooked
2 tablespoons
large portion
1 glass
DINNER
Chicken, broiled
Tossed green salad,
herb dressing
Peas and carrots
Brussel Sprouts
Apple
Coffee or tea
half of 21/2 lb. chicken
large portion
1/2 cup
1/2 cup
1 medium
as desired
143
DIET II
Menu for Thursday
BREAKFAST
Orange
Egg, scrambled
Bread
Butter (or margarine)
Skim milk
1
1
1 slice
1 pat
1 glass
LUNCH
Codfish, steamed
Lemon and parsley
dressing
Spinach
String beans
Bread, thinly buttered
Coffee or tea
1 slice (4"x2"xl")
1/2 cup
1/2 cup
1 slice
as desired
DINNER
Pot roast, defatted
gravy
Potato, baked
Carrots
Turnip greens
Tossed salad
French dressing
Coffee or tea
8 ounces meat
1/2 medium
1/2 cup
1/2 cup
large serving
1 tablespoon
as desired
BED-TIME SNACK
Skim milk
1 glass
144
DIET II
Menu for Friday
BREAKFAST
Tomato juice
Oatmeal, with 1 pat
butter
Pot cheese
Skim milk
Coffee or tea
1/2 cup
1/2 cup cooked
3 tablespoons
1 glass
as desired
LUNCH
Lobster meat
Vegetable salad
Mayonnaise
Bread
Skim milk
Coffee or tea
4 ounces
1 large serving
1 teaspoon
1 slice
1 glass
as desired
DINNER
Haddock steak, steamed
Vegetable salad
sour cream dressing
String beans
Broccoli
Ice milk
Coffee or tea
¾ lb.
large serving
2 tablespoons
1/2 cup
1/2 cup
1 average scoop
as desired
145
DIET II
Menu for Saturday
BREAKFAST
Grapefruit
Lean meat, cold cut
Bread
Skim milk
Coffee or tea
1/2
2 slices (4"x3"x1/8")
1 slice
1 glass
as desired
LUNCH
Frankfurters, griddle, grilled
Sauerkraut, raw or cooked
Bread
Tea
DINNER
Broth, clear
Steak, broiled, lean
Mushrooms
Carrots
Coleslaw
Orange and grapefruit sections,
unsweetened
Coffee or tea
BED-TIME SNACK
Skim milk
3
large portion
1 slice
as desired
1 cup
10 ounces raw
1/2 cup
1/2 cup
1/2 cup
½ cup
as desired
1 glass
146
DIET III
Menu for Sunday
BREAKFAST
Grapefruit
Eggs, scrambled
Butter
Ham, lean, grilled
Bread, whole wheat toast
Coffee or tea
LUNCH
Tomato juice
Cheese and tomato sandwich,
open face grilled
Fresh garden salad
Skim milk
1/2
2
1 pat
2 slices
2 slices
as desired
4 ounces
1
large serving
1 cup
DINNER
Roast beef, lean
Carrots
Broccoli
Tossed salad
Apple, medium
3/4 lb.
1/2 cup
1/2 cup
1 serving
1
BED-TIME SNACK
Buttermilk
1 glass
147
DIET III
Menu for Monday
BREAKFAST
Orange
Cottage cheese
Bread, whole wheat toast
Butter
Skim milk
Coffee or tea
1
3 tablespoons
1 slice
1 pat
1 cup
as desired
LUNCH
Salmon, canned (oil drained)
Fresh mixed garden salad
Bread
Skim milk
Coffee or tea
6 ounces
large serving
2 slices
1 cup
as desired
DINNER
Beef, boiled
Tossed green salad, garlic
dressing
Turnip greens
Carrots and peas
Fresh fruit cup
148
¾ lb.
1 serving
1/2 cup
1/2 cup
1/2 cup
DIET III
Menu for Tuesday
BREAKFAST
Grapefruit juice
Eggs, poached
Bacon, crisp
Bread, whole wheat
Skim milk
Coffee or tea
1/2 cup
2
2 strips
1 slice
1 cup
as desired
LUNCH
Cold cuts
Lettuce and tomato salad
Bread
Coffee or tea
4 slices 4"x3"x1/8"
large serving
2 slices
as desired
DINNER
Chicken, roast
Fresh vegetable salad
Oil and vinegar dressing
Asparagus
String beans
Ice milk
Coffee or tea
1/2 of a 21/2 lb. chicken
large serving
1 teaspoon oil
1/2 cup
1/2 cup
1 #12 scoop
as desired
149
DIET III
Menu for Wednesday
BREAKFAST
Orange juice
Buckwheat groats
Butter or margarine
Farmer cheese
Skim milk
Coffee or tea
1/2 cup
1/2 cup
1 pat
2 ounces
1 cup
as desired
LUNCH
Haddock steak, steamed
Tartar sauce
Spinach
Cauliflower
Potato, mashed
Skim milk
Coffee or tea
1/2 lb.
1 tablespoon
1/2 cup
1/2 cup
1/2 cup
1 cup
as desired
DINNER
Liver, broiled
Mushrooms
Carrots
Macaroni, cooked
Tomato sauce
Leafy green salad (lettuce,
escarole, chicory)
Honeydew
Coffee or tea
150
1/2 lb.
1/2 cup
1/2 cup
1/2 cup
1 tablespoon
1 serving
1/8
as desired
DIET III
Menu for Thursday
BREAKFAST
Grapefruit
Cold cuts, lean
Bread, whole wheat
Skim milk
Coffee or tea
LUNCH
Beef stew, defatted gravy
Bread
Lettuce and tomato salad,
herb dressing
Coffee or tea
1/2
4 slices
1 slice
1 cup
as desired
4 ounces meat
1 slice
1 serving
as desired
DINNER
Lamb chops, broiled
Potato, baked
Brussels sprouts
String beans
Tossed salad
Watermelon, diced
Coffee or tea
2 medium
1/2 medium
1/2 cup
1/2 cup
1 serving
1 cup
as desired
BED-TIME SNACK
Skim milk
1 glass
151
DIET III
Menu for Friday
BREAKFAST
Orange juice
Cheese omelet (2 eggs,
2 oz. cheese)
Bread, whole wheat
Skim milk
Coffee or tea
1/2 cup
1
1 slice
1 cup
as desired
LUNCH
Fish cake
Tomato sauce
Lettuce wedge with lemon
Muffin, 2" diameter
Skim milk
Coffee or tea
1 large
1 tablespoon
1 large
1
1 cup
as desired
DINNER
Poached fish fillet
Newburg sauce, hot
Swiss chard
Beets
Bread
Ice cream
Coffee or tea
¾ lb.
1 tablespoon
1/2 cup
1/2 cup
1 slice ,
1 #12 scoop
as desired
152
DIET III
Menu for Saturday
BREAKFAST
Pineapple juice
Oatmeal, cooked
Skim milk
Chip beef
Bread, whole wheat toast
Coffee or tea
LUNCH
Cottage cheese
Chopped cucumber, radishes and
chives, herb dressing
Bread
Skim milk
Coffee or tea
DINNER
Steak, lean, broiled
Potato, baked
Cole slaw
Zucchini
String beans
Strawberries, fresh
1/3 cup
1/2 cup
1 cup
4 ounces
1 slice
as desired
3 tablespoons
1 cup
1 slice
1 cup
as desired
3/4 1b.
1/2 medium
1/2 cup
1/2 cup
1/2 cup
1/2 cup
153
FOOD COMPONENTS
DAIRY PRODUCTS
%
CarboFood
hydrate
Butter, fresh
trace
Buttermilk
4.8
Cheese, American
trace
Cheese, Cottage, dry 4.3
Cheese, Cream
trace
Cheese, Dutch
trace
Cheese, Gruyere
trace
Cheese, Parmesan
trace
Cheese, Roquefort
1.0
Cheese, Swiss
1.3
Cream
2.3
Egg
0.0
Ice cream
17.5
Milk, skimmed
4.8
Milk, whole
4.6
Yogurt, defatted
4.8
%
Protein
0.4
3.4
24.9
21.0
3.2
28.1
36.8
34.4
22.6
27.6
1.8
11.9
3.9
3.4
3.3
3.4
%
Fat
85.1
0.2
34.5
0.2
86.0
16.8
33.4
29.7
29.5
24.9
42.0
12.3
13.2
0.2
3.7
0.2
%
Water
13.9
90.2
37.0
75.0
10.0
46.3
21.9
28.0
30.0
31.4
53.0
73.4
62.8
90.2
87.0
90.2
Calories
per
ounce
226
10
120
28
232
77
131
118
110
132
116
46
60
10
19
10
BREAD
Rye
Corn (Johnny cake)
White
Whole wheat
Zwieback
53.2
47.1
54.3
49.7
73.5
9.0
7.9
8.0
9.7
9.8
0.6
4.7
1.4
0.9
9.9
35.7
38.1
35.2
38.4
5.8
78
80
80
75
130
CEREALS
Barley, boiled
Oatmeal, cooked
Tapioca
Wheatena, uncooked
Macaroni, boiled
27.6
8.2
95.0
76.3
23.7
0.6
1.5
0.4
11.0
3.6
2.9
0.9
0.1
1.4
0.6
69.6
89.1
11.2
10.9
72.2
37
14
111
111
34
24.0
22.3
26.8
46.0
15.0
12.3
' 20.0
58.5
58.4
149
66
64
25.2
33.3
21.6
8.2
50.5
56.6
86
61
17.0
29.6
6.7
7.3
39.6
611.
38
54
MEATS
Bacon, streaky, crisp 0.0
Beef, corned
0.0
Beef, sirloin, roast, lean 0.0
Beef, steak, broiled,
lean
0.0
Beef, boiled, lean
0.0
Chicken, boiled
(with bone)
0.0
Chicken, roast
0.0
154
FOOD COMPONENTS
MEATS (Cont.)
Food
Chicken, roast
(with bone)
Duck, roast
Ham, boiled, lean only
Lamb, chop, lean only
Lamb, roast
Liver
Sausage, beef
Sausage, pork
Sweetbreads, stewed
Tongue¡ stewed
Veal, roast, filet
%
Carbo- %
hydrate Protein
0.0
0.0
0.0
0.0
0.0
0.0
0.0
9.8
0.0
0.0
0.0
FISH
Bass, steamed
0.0
Bloaters, grilled
0.0
Catfish, steamed
0.0
Clams
5.2
Cod, steamed
0.0
Cod, grilled
(with added fat)
0.0
Crabmeat, boiled
0.0
Flounder, steamed
0.0
Flounder, fried
6.5
Haddock, fresh,
Steamed
0.0
Halibut, steamed
0.0
Lobster, boiled
0.0
Mackerel, fried
0.0
Oysters trace
Salmon, fresh, steamed 0.0
Salmon, canned
0.0
Sardines, canned
(drain oil)
0.0
Scallops, steamed trace
Shrimps
0.0
Sole, steamed
0.0
Sole, fried
5.4
Trout, steamed
0.0
Whiting, steamed
0.0
%
Fat
%
Water
Calories
per
ounce
16.0
22.8
23.1
12.4
25.0
16.5
18.2
8.8
22.7
18.0
30.5
3.9
23.6
13.4
8.2
20.4
8.1
19.7
28.8
9.1
24.0
11.5
33.0
52.0
55.8
25.2
52.4
73.3
55.2
50.7
65.6
56.9
55.1
29
89
62
36
83
41
77
98
51
84
66
19.5
22.6
20.4
10.6
18.0
5.1
17.4
3.7
1.1
0.9
73.3
55.6
73.6
80.8
79.2
36
73
34
23
23
27.0
19.2
19.4
17.0
5.3
5.2
1.7
12.9
64.6
72.5
76.6
61.5
45
36
27
61
22.0
22.7
21.2
20.0
10.2
19.1
19.7
0.8
4.0
3.4
11.3
0.9
13.0
6.0
75.1
70.9
72.4
65.6
85.7
65.4
69.9
28
37
34
53
14
57
39
20.4
22.4
22.3
17.6
20.1
22.3
19.9
22.6
1.4
2.4
1.3
18.4
4.5
0.9
50.7
73.1
62.5
78.9
53.8
70.6
76.9
84
30
32
24
78
38
26
155
FRUITS—3-5%
LIST A
Cranberries Gooseberries Lemon Loganberries Rhubarb
FRUITS—5-10%
LIST B
Apricots, fresh
Blackberries
Currants
Damson Plum
Gooseberries, ripe
Grapefruit
Melon, cantaloupe
Melons, yellow
Mulberries
Oranges
Peaches
Plums, cooking, raw
Quince
Raspberries
Strawberries
Tangerines
FRUITS—10-15%
LIST C
Apples Cherries
Figs, green Green Gage
Plums Nectarines Orange
Juice Pears
Pineapple, fresh
Plums, Victoria
FRUITS—10-20%
Apricots, dried, stewed, or canned
Avocado
Banana
Fruit Salad,
canned Grapes
Peaches canned
Pears, canned
Pineapple, canned
Prunes, stewed
156
LIST D
FRUITS—21% and over
LIST E
Apricots, dried, raw
Dates
Figs, dry, raw
Figs, dry, stewed
Loganberries, canned
Olives
Peaches, dried, raw
Prunes, dried, raw
Raisins
VEGETABLES—2-3%
Beans, French, boiled
Beans, string
Broccoli
Cabbage
Cauliflower
Celery
Chicory
Cucumber
Endive
Lettuce
Marrow
Mushroom
Mustard and cress
Onions, boiled
Sea-kale
Spring greens
Tomato
Turnip, boiled
Turnip tops
Water cress
LIST A
VEGETABLES—4-6%
LIST B
Artichokes
Asparagus
Brussels sprouts
Cabbage, red, raw
Carrots
Eggplant
Leeks
Onions, raw
Pumpkin
Radish
Spinach
Turnips, raw
157
VEGETABLES—10%
LIST C
Beans, broad, boiled
Onions, spring, raw
VEGETABLES—15%
LIST D
Beet root
Horseradish
Parsnips
Peas
VEGETABLES—20% and over LIST E
Beans, baked
Lentils
Peas, dried, boiled
Peas, canned
Potatoes
Sweet potatoes
SUBSTITUTIONS
BREAD (1 slice is equivalent to):
Cereal, cooked
Rice, cooked
Macaroni, cooked
Noodles, cooked
Potato, white, boiled
Potato, sweet
Corn
Crackers
graham
saltines
soda
Margarine
Oil
French dressing
Mayonnaise
Sour cream
1/2 cup
1/2 cup
1/2 cup
1/2 cup
1/2 cup
1/4 cup
1/3 cup
2
5
3
BUTTER (1 teaspoon is equivalent to):
1 teaspoon
1 teaspoon
1 tablespoon
1 tablespoon
2 tablespoons
FRUITS AND VEGETABLES
See lists of fruits and vegetables which are arranged
according to the percentage of carbohydrate content.
1 cup of List "A" is approximately equivalent to 1/2 cup
of List "B," etc.
158
HIGH-PROTEIN FOODS
Grams
Food
Portion Protein
Beef, corned
4 oz.
25
Beef, roast, lean
4 oz.
30
Beef, steak, broiled
4 oz.
29
Beef, boiled
4 oz.
38
Chicken, boiled (with bone) 4 oz.
19
Chicken, roast (with bone) 4 oz.
18
Ham, boiled, lean
4 oz.
26
Lamb, chop, broiled, lean 4 oz.
30
Lamb, roast
4 oz.
28
Liver, broiled
4 oz.
19
Veal, roast
4 oz.
35
Fat Carbohydrate
17
0
14
0
24
0
9
0
8
0
4
0
15
0
20
0
23
0
9
0
13
0
Fish, canned
Fish, steamed
Sardines, canned
3 oz.
4 oz.
4 oz.
17
25
23
5
1
26
0
0
0
Buttermilk
Cheese, cottage, dry
Cheese, whole milk
Egg
Milk, skim
Milk, fresh
8 oz.
4 oz.
1 oz.
1
8 oz.
8 oz.
8
25
7
6
8
8
1
trace
9
6
1
9
11
trace
trace
0
11
159
11
YOU'LL
ENJOY
THESE
OTHER
LANCER
BOOKS
THE CAREER OF DAVID NOBLE. Frances
Parkinson Keyes reveals the influence of a small New
England town on the lives of two lovers. 50¢
SHE by H. Rider Haggard. SHE is the immortal classic
of exotic adventure and timeless romance by one of the
world's master story tellers. 50¢
THE STRUMPET SEA by Ben Ames Williams. A
whaling captain, a dedicated missionary, his lonely
wife—in the South Seas. 50¢
LOVE by Guy De Maupassant. A Frenchman writes
about love of many kinds in this extraordinarily
penetrating collection of short stories. 50¢
THE HEARTH AND EAGLE by Anya Seton. The
best-selling authoress spins a superlative story of history
and romance in New England. 60¢
WHAT BECAME OF ANNA BOLTON by Louis
Bromfield. She became the most desirable woman in
rich and decadent pre-war Europe. 40¢
Lancer books are sold at most newsstands. If not available, send
price of book and five cents to LANCER BOOKS, 26 W. 47th St.,
New York 36, N.Y.