IEEE Paper Template in A4 (V1)
advertisement
")
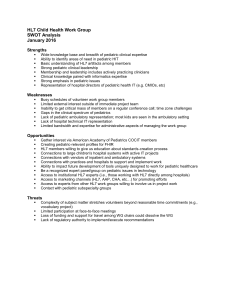
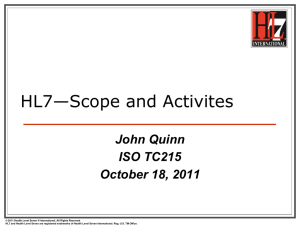
The use of HL7 in the domain of Medical Devices Fabrizio Pecoraro and Daniela Luzi Institute for Research on Population and Social Policies, National Research Council Via Palestro 32, 00185, Rome, Italy f.pecoraro@irpps.cnr.it d.luzi@irpps.cnr.it Abstract— The paper describes the approach used to design and develop a Medical device information system (MEDIS) focusing in particular on the description of the Domain Analysis Model (DAM) of medical devices as well as on the conversion of the HL7 RIM meta-model into a logical data model. Keywords—Medical devices, Clinical investigations, HL7, logical data model I. INTRODUCTION/BACKGROUND Progress in clinical research depends largely on the results of Clinical Investigations (CIV), i.e. any “study of human subjects that is designed to answer specific questions about biomedical or behavioural interventions (drugs, treatments, devices, or new ways of using known drugs, treatments, or devices)” [1]. CIVs are complex processes encompassing different steps, from specification and planning to execution and final result analysis. There is an increasing number of applications related to data and trial management systems (CDMS and CTMS) that support different aspects of trial design [2] (protocol authoring systems, Case Report Form generation) as well as its performance (electronic data capture for both data analysis and regulatory submission, patient recruitment, scheduling of clinical activities, site management, etc.) [3,4]. In this context challenges still concern the adaptation of data models on different clinical domains and pathologies as well as on various organizational frameworks. This makes it often necessary to develop tailored databases from scratch to manage new clinical studies. Moreover, the integration between these different legacy systems is still a crucial issue, considering, the variety of both data and knowledge to be managed, especially in multi-centric clinical studies [5]. Besides the achievement of interoperability within the framework of clinical research systems, there is an increasing interest in linking clinical research data to hospital and laboratory information systems as well as Electronic Health Records (EHRs). Within this scenario, a specific role is played by trial registries, defined [6] as “a database of planned, ongoing or completed trials, published or unpublished, containing details of the trial’s objectives, patient population, sample size and tested interventions”. The set of data contained in these registries as well as the process of acquiring them fulfils specific users’ information need and purposes. Nevertheless, the integration among national and international registries and/or between them and other e-health information system still represents a crucial concern. In Italy the National Research Council supported by the Italian Ministry of Health developed an information system, MEDIS (Medical Device Information System) that manages the approval process of CIV on Medical Devices (MD) and monitors its performance. In particular MEDIS supports both applicants in the submission of data and regulatory documents and the National Competent Authority (NCA) in the evaluation and monitoring of CIVs. A concise overview of the methods used in the design and development of a national registry is provided in paragraph 3, while the medical device domain analysis model is described in paragraph 4, and the conversion of the HL7 meta-data model into the logical data model of the MEDIS system is reported in paragraph 5. II. OBJECTIVES This paper describes the approach used to design and develop MEDIS focusing, in particular, on the description of the Domain Analysis Model (DAM) and how it has been transformed into a logical data model. The novelty of our approach resides on the development of a conceptual model describing MDs in framework of CIVs as well as on the application of HL7 DAM to develop a logical data model. III. METHODS Taking into account the necessity to interoperate with other systems, MEDIS design and development was based on HL7 v.3 standards following its methodology in the description of the use cases for the identifications of the actors involved and interactions between them. Moreover, the process description and the identification of both data and documents necessary for the evaluation of CIVs performed by NCAs are based on the European Directives, ISO standards and ICH Good medical practice guidelines. The analysis of the already balloted HL7 domains [7], and in particular the BRIDG project [8] was the starting point to define MEDIS domain analysis model and the relevant conceptual classes, attributes and data types. The BRIDG DAM focuses in particular on the process of a clinical investigation capturing concepts and data from the clinical protocol, that is the source document that describes the planned investigation in detail. On the contrary, MEDIS DAM has to consider this process from a different perspective, taking into account the information needs of a National competent authority that has to assess investigation proposals as well as monitoring their performance. For these reasons the process to be described has to encompass also the submission and evaluation process, while data captured during the performed clinical investigation have to be used for monitoring purposes. Therefore, we adopted some BRIDG conceptual entities that can be easily mapped with our domain. For instance, we modeled classes describing actors considering: (1) E_Organization CMET that identifies an organization including its employees and its relationship with other organizations; (2) the Study Participation model that describes information related to the sites in which clinical investigations are conducted and investigators involved in each site as well as the information on the scientific, ethical, and regulatory committees. However, to capture particular aspects of our domain we had to develop a customized model such as medical devices, regulatory documents, adverse event reporting. A detailed description of the DAM is reported in a previous publication [9], while this paper focuses on the device domain model. Moreover, in order to design the MEDIS database we adopted a novel approach, which converts the DAM schema into a logical data model based on HL7 Reference Information Model (RIM) (see § 5). IV. MEDICAL DEVICE DOMAIN MODEL To model the description of the products involved in the whole clinical investigation lifecycle a set of characteristics of the MD domain has been taken into account. The variety of MD types (ranging from implantable to imaging devices) as well as their different application in the delivery of care (diagnostic, treatment, prevention) makes it difficult to have a MD comprehensive conceptual description. Moreover, in the framework of an approval process of a CIV the investigational device is described in detail in regulatory documents such as clinical protocol, risk assessment document and Investigator’s brochure. Other MDs are often mentioned in the regulatory documentation to prove for instance the safety requirements of the investigational MD based on the characteristics of a similar MD already commercialised. Another example concerns the case when a comparator is used in a CIV to measure the efficacy of the MD under investigation. Given this premise, the use of HL7 RIM resulted to be a valid means to develop a product conceptual model (fig. 1) that can be decomposed into the following conceptual areas: The static area represented by the RIM classes Entity and Role that describe a general artefact involved in a clinical investigation processes and, its role (i.e. an artefact has the role of a MD); The dynamic area represented by the RIM classes Participation and Act, that describe the different subprocesses of the clinical investigation lifecycle (i.e. Notification, Evaluation and Clinical Investigation) and how any artefact takes part in each sub-process (i.e. a MD participates as a investigational device in the activity of performing a clinical investigation). Figure 1. Medical Device DAM The static area entails only two Entities: ArtefactKind and ArtefactInstance. Using the Entity ArtefactKind it is possible to model a common description of any product, i.e. name, description, models. This class is related to a set of Role classes that are the basis to distinguish the different types of products involved in the clinical investigation and to specialize the description of each artefact. For example the Roles MD and Drug have a set of attributes that describe respectively the specificity of a medical devices class (such as risk class, national and international classification codes) and pharmaceutical products (such as drug active principle, drug classification). As highlighted in figure 1 this model considers data necessary to evaluate safety requirements of a device under investigation extracted from regulatory documents (see Evaluated MD box) as well as information used to track MD in the CIV performance (see Tested MD). The determinerCode of the RIM class Entity has been used to distinguish whether any given artefact stands for a specific object (determinerCode = Instance, i.e. an explicit stent implanted in a given patient) or an object description (determinerCode = Kind, i.e. the class of stent investigated in the clinical trial described in clinical protocol). This model creates an isomorphism in which the Roles related with the Entity ArtifactKind are mirrored in the Entity ArtifactInstance. The dynamic area allows defining the functions covered by each artefact in the whole clinical investigation lifecycle. Using the RIM stereotype Participation it is possible to distinguish, for example, whether a MD described in the static area is an Investigational, a Comparator or a Similar device. This approach is also used to describe a drug that can be either dispensed by a MD (Pharmaceutical product) or used as a Comparator during a clinical investigation. Finally, the stereotype Act has been used to model the three main subprocesses of the clinical investigation lifecycle: Notification, Evaluation and Clinical Investigation. V. LOGICAL DATA MODEL The integration of the HL7 standards in healthcare information systems need to map the HL7 RIM and more specifically the RMIM (Refined Message Information Model) classes with the tables of the database schema. This task is very complicated due to the heterogeneity of data models, schema structures and query language they support [10]. Moreover, the association of the HL7 RIM to a database table requires the identification of the multiple relationship that link HL7 classes. For this purpose different mapping techniques are used [10,11], but usually they do not provide satisfactory results. Generally, automatic tools that map HL7 still require human intervention as well as a profound knowledge of both HL7 and the domain of application. Moreover, these tools developed by middleware applications are usually timeconsuming and expensive parts of in the design and development of interoperable information systems. In this paper we propose a novel method to design a logical data model based on the DAM to develop the MEDIS relational database. The purpose of this technique is to create a logical data model that closely matches the RIM logical meta-model so that the mapping between HL7 messages and the database is straightforward. Similar approaches are proposed in the literature. Eggebraaten [12] uses both the entity-relationship (ER) and the entity-attribute-value (EAV) methodologies to map the RIM classes into tables of the physical data model. The EAV model is applied in particular to RIM Observation class to capture different data types of the attribute value, while ER model is used to map the other RIM classes. Based on Eggebraaten approach, Yang et al. [13] map the RMIM and CMET classes into a physical database in the domain of ambulatory encounters. HL7 has established a working group (RIMBAA, RIM Based Application Architecture) focused on the use of the RIM model to design clinical application and databases, promoting the development of HL7 version 3-compliant applications. RIMBAA proposes a technology matrix that contains all possible “roadmaps” to transition between the persistence layer and the serialized representation (e.g. XML messages) of the data [14]. Our approach took advantage of the RIM meta-model - thus privileging an ontological point of view - to represent a domain where data and data types had to be identified almost from scratch being the standardisation in this domain still at an initial stage. Therefore, compared to other approaches, our mapping concerns the high level RIM classes to define both the multiple association between the objects of the MD domain and the rules that represent their behaviour. Similarly with the RIMBAA reference implementation [15], we used Hibernate framework to map Java objects into a relational database. In figure 2 a portion of the MEDIS logical data model showing the MD representation is depicted. It is divided in two different conceptual areas: The instance area that exactly transforms each DAM class into a table of the database. These tables store all information collected during the whole clinical investigation process. Moreover, this area also explicitly maps the six base classes of the HL7 RIM backbone. The rule area that represents the logic governing the relationship allowed between the instance area tables as well as the business process of the clinical investigation lifecycle. In the instance area for each class of the DAM a separate table is created containing all the attributes for that specific class as well as those inherited for its parent classes. Furthermore, each DAM tables is associated with a RIM table as a generalization depending on its stereotype, for instance the table ArtifactKind is associated with the table Entity. Moreover, the clinical investigation sub-processes are stored in the instance area in the Notification, Evaluation and Clinical_Investigation tables. In our approach the relationship between these tables is stored in the Act_Relationship table that tracks the evolution of the business process of a single CIV proposal. In this way it is possible to identify all steps of the entire process as well as the state reached by each CIV proposal. Figure 2. MEDIS logical data model The rule area is composed by a set of tables that store the different type of the instance objects depending on their stereotype, for example the Act_Type table contains the different category of the CIV sub-processes tables (i.e. Notification, Evaluation and Clinical_Investigation). Moreover, the Allowed tables store the rules that express the allowed relationship between the instance area tables as modeled in the DAM (for example the Allowed_Role_Entity table express that the relationship between the Artifact_Kind and the MD_Kind is permitted). Moreover, the tables of the rule area are used by the business logic layer of the MEDIS system to determine the functionalities active in a given time. This makes it possible for example to prevent CIV applicant to notify a serious adverse event before the clinical investigation has started. Despite these benefits, some limits appear evident in respect of the complexities of the overall database schema realized, both in terms of the expression of complex queries as well as the computational costs of the execution of the queries themselves. Given the central role played by regulatory documents in the framework of NCA approval of CIVs, our next step is to analyse clinical protocols and risk analysis documents in order to identify their structure and information content using CDA representation. VI. CONCLUSION AND FUTURE WORKS This paper describes the use of HL7 standards to design and develop an interoperable system in the CIV on MD domain. This is an important issue considering that the interoperability is going to be fundamental in this domain due to the exponential increasing of both clinical investigations and MD deployment. The adoption of HL7 RIM to represent MDs allowed us to describe their characteristics and in particular the use of stereotypes makes it easier to highlight the different artefacts involved in a CIV as well as their role in the process. Moreover, the proposed approach to develop a logical data model simplifies the development of a tool that easily converts the data stored in the database in HL7 standard messaging. Given that regulations in this domain frequently change and MDs are continuously evolving in terms of their technological complexity, this approach makes it also possible to update and modify the database schema as well as the rules governing it. REFERENCES ACKNOWLEDGMENT This study was supported by the Italian Ministry of Health through the MEDIS project (MdS-CNR collaboration contract n° 1037/2007). [1] [2] [3] [4] [5] [6] National Institute of Health, Glossary & Acronym List. Available at: http://grants.nih.gov/grants/glossary.htm Oliveira GA, Salgado NC, (2006). Design aspects of a distributed clinical trials information system. Clinical Trials, 3, 385-396. McDonald DW, Weng C, Gennari JH, (2004). The multiple views of inter-organizational authoring. Proc. of the 2004 ACM Conference on Computer Supported Cooperative Work, Chicago, Illinois, USA, pp. 564-573. Durkalski V, Zhao W, Dillon C, Kim J, (2010). A web-based clinical trial management system for a sham-controlled multicenter clinical trial in depression. Clinical trials 7 pp. 174182. Shankar RD, Martins SB, O’Connor MJ, Parrish DB, Das AK, (2006). Toward Semantic Interoperability in a Clinical Trials Management System. Lecture notes in Computer Science, 4273, pp 901-912. Moja LP, Moschetti I, Nurbhai M, Compagnoni A, Liberati A, Grimshaw JM, Chan A, Dickersin K, Krleza-Jeric K, Moher D, [7] [8] [9] [10] [11] [12] [13] [14] [15] Sim I, Volmink J, (2009). Compliance of clinical trial registries with the World Health Organization minimum data set: a survey. Trial 10 (56). DOI: 10.1186/1745-6215-10-56, available from http://www.trilasjournal.com/content/10/1/56. Health Level Seven version 3. Available at: hl7.org/v3ballot/html/welcome/environment/index.htm Fridsma BD, Evans J, Hastak S, Mead CN, (2007). The BRIDG Project: A technical report, JAMIA, 15, pp 130-137. D. Luzi, F. Pecoraro, F.L. Ricci, G. Mercurio, (2009). A medical device domain analysis model based on HL7 Reference Information Model. In: Medical Informatics in a United and Healthy Europe. Proceeding of MIE 2009, IOS Press, pp 162-166. Gul M, Afzal M, Hussain M Alam M, Latif K, Ahmad HF, (2010). Interactive Mapping Tool for HL7 RIM-to-Relational Database Using Knowledge Game. IHIC Conference, Rio De Janeiro, Brazil. Umer S, Afzal M, Hussain M, Ahmad HF, Latif K, (2009). Design and implementation of an automation tool for HL7 RIM-To-Relational Database Mapping. IHIC Conference, Kyoto, Japan. Eggebraaten TJ, Tenner JW, Dubbels JC, (2007). A health-care data model based on the HL7 Reference Information Model. IBM Journal of Research and Development. 46(1) pp 5-18 Yang, W.-Y., Lee, L.-H., Gien, H.-L., Chu, H.-Y., Chou, Y.-T., and Liou, D.-M. (2009). The design of the hl7 rim-based sharing components for clinical information systems. World Academy of Science, Engineering and Technology, 53 HL7. The RIMBAA Technology Matrix. Available at http://www.ringholm.de/docs/03100_en.htm HL7. A Java-based RIMBAA Reference Implementation. Available at http://www.ringholm.com/docs/03110_en_HL7_RIMBAA_Jav a_Reference_Implementation.htm