Large Bladder Mass in a 83-year old Man
advertisement

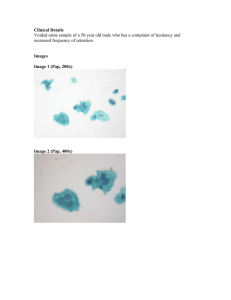
California Tumor Tissue Registry Case of the Month - Vol 7(9) June, 2005 “An 83 y/o Man with Hematuria” An 83-year-old man presented with a six week history of hematuria. Upon cystoscopic examination a bladder tumor was found which was 10 cm in greatest diameter, broadbased, smooth and somewhat lobular. The tumor was located in the left wall and obstructed the ureter. Imaging studies showed enlarged left iliac nodes. The tumor was curetted resulting in multiple fragments of friable tissue measuring 8.0 x 6.0 x 1.5 cm in aggregate and weighing 50 grams. Approximately two-thirds of the fragments contained an infiltrating high-grade malignant neoplasm consisting mostly of spindled cells (Fig. 1). There were, however, foci of delicate lace-like osteoid lined by oval to polygonal cells with scant cytoplasm and large hyperchromatic nuclei with prominent nucleoli (Fig. 2). Focal cartilaginous differentiation was also seen (Fig. 3). Other regions showed glandular and squamous differentiation (Fig. 4). The epithelial component showed immunoreactivity for cytokeratin and EMA, while the mesenchymal component was diffusely reactive for vimentin, alpha-1antitrypsin and lysozyme. S100, desmin and smooth muscle actin were negative. Diagnosis: “Carcinosarcoma of the bladder with components of high-grade papillary urothelial carcinoma and chondroblastic osteosarcoma” Wafaa Elatre, Fuoad Abdelhalim, Donald Chase Loma Linda University and Medical Center Department of Pathology and Human Anatomy Follow-up: The patient underwent radical resection of the bladder and prostate, and had an ileo-conduit. Although the surgery was uneventful the post-operative recovery period was complicated and the patient expired one month after surgery. Chondrosarcoma (CS) of the bladder is a rare tumor occurring late in life, usually in the 7th or 8th decade. It has a male preponderance and usually presents with hematuria. Like uterine CS, it has been linked to previous exposure to cyclophosphamide chemotherapy, however recurrent urothelial carcinoma is the most common antecedent. The mass is usually bulky, polypoid and contains both malignant epithelial and mesenchymal components. The epithelial component usually consists as a mixture of: urothelial carcinoma adenocarcinoma squamous cell carcinoma, or small cell carcinoma The Mesenchymal components usually includes one or more types of: CTTR’s Case of the Month June, 2005 1 chondrosarcoma leiomyosarcoma malignant fibrous histiocytoma osteosarcoma, or rhabdomyosarcoma Rarely has the tumor shown fatty or neural features. There is considerable confusion and disagreement as to the nomenclature and histogenesis of the bladder CS. The terms carcinosarcoma, sarcomatoid urothelial carcinoma, and malignant mixed mesodermal tumor (MMMT) have been used interchangeably. The term sarcomatoid urothelial carcinoma generally is used to define a carcinoma with a prominent spindle cell component which is cytokeratin positive. The terms CS/MMMT have usually been reserved for tumors with distinct mesenchymal heterologous elements such as bone (as seen in this case), cartilage, and muscle etc. The terminology distinction, however, seems irrelevant because currently there is no clinical significance in splitting. The presentation, treatment, and prognosis are similar. Most patients die within a few months of presentation. Grossly, both CS/MMMT and sarcomatoid urothelial carcinoma are seen as bulky polypoid or nodular tumors within the bladder. Microscopically the malignant epithelial and stromal components may be sharply demarcated or may gradually merge with each other. Treatment of CS/MMMT and sarcomatoid urothelial carcinoma is stage dependant, and is the main predictor of patient survival irrespective of treatment, histological subtypes, or gender. Most patients present with a high stage malignancy and the preferred modalities of treatment include cystectomy or transurethral resection with or without radiation therapy and chemotherapy. In a large series there seemed no difference between CS/MMMT and sarcomatoid urothelial carcinoma. 79% of CS patients died at a mean of 17.2 months (range 1 to 48 months) whereas 81% of patients with sarcomatoid urothelial carcinoma died at a mean of 9.8 months (range 1 to 73 months). The differential diagnosis of bladder carcinosarcoma includes urothelial carcinoma with pseudosarcomatous stroma, carcinoma with osseous or cartilaginous metaplasia, and primary osteosarcoma or chondrosarcoma of bladder. CS may also simulate myofibroblastic proliferations such as post-operative spindle cell nodule and inflammatory pseudotumor. Sarcomatoid urothelial carcinoma with osseous metaplasia is the main differential. In this entity clearly malignant osteoid production is present. The prognosis is poor with patients dying within 6 months. Urothelial Carcinoma with Pseudosarcomatous Stroma: Urothelial carcinoma may rarely possess a cellular stroma mimicking sarcoma or sarcomatoid urothelial carcinoma The stroma may be myxoid, containing stellate or multinucleated cells or consist of short intersecting fascicles of spindle cells. Cytologic atypia is usually minimal. The stromal cells show immunoreactivity for actin but are negative for cytokeratin. Squamous cell carcinoma of the bladder may also have a pseudosarcomatous stroma. CTTR’s Case of the Month June, 2005 2 Primary Osteosarcoma of Urinary Bladder is an extremely rare tumor with only seven reported cases in the world literature. The majority occur in older males. They tend to be large, bulky, and deeply infiltrative tumors. Microscopically, malignant cells are intimately associated with delicate lacelike osteoid. Urinary carcinosarcoma has shown 40 microsatellite markers from 19 human chromosomes. In some cases there is an identical LOH on chromosomal arms 9p, 9q, 8p, and 8q, corresponding to relatively early events in bladder carcinogenesis. Discordant losses between two alleles in the remaining chromosomes, associated with progression, have been seen in 9 tumors with a trend toward a higher incidence in the more advanced tumors (N1M1 and N1Mx). E-cadherin has been seen in the carcinomatous components (5 of 6), whereas most of sarcomatous elements have displayed absence of the protein product (4 of 6). These results indicate that both the carcinomatous and sarcomatous components of carcinosarcoma are derived from a common stem cell. Down regulation of E-cadherin may define one of the pathways responsible for conversion of epithelial cells to the sarcomatous phenotype. Suggested Reading: Lopez-Beltran A, Pacelli A, Rothenberg HJ, Wollan PC, Zincke H, Blute ML, Bostwick DG. Carcinosarcoma and sarcomatoid carcinoma of the bladder: Clinicopathologic study of 41 cases. J Urol 1998; 159:1497-1503. Lahoti C, Schinella R, Rangwala AF, Lee M, Mizrachi H. Carcinosarcoma of urinary bladder: report of 5 cases with immunohistologic study. Urology 1994; 43:389. Torenbeek R, Blomjus CM, de Bruin PC, Newlin DWW, Meijer CJLM. Sarcomatoid carcinoma of the urinary bladder. Am J Surg Pathol 1994; 18:241. Bannach B, Grignon DJ, Shum DT. Sarcomatoid transitional cell carcinoma vs pseudosarcomatous stromal reaction in bladder carcinoma. J Urol Path 1993; 1:105-19. Young RH, Eble JN. Unusual forms of carcinoma of the urinary bladder. Hum Pathol 1991; 22:948. Sigal SH, Tomaszewski JE, Brooks JJ, Wein A, LiVolsi VA. Carcinosarcoma of bladder following long-term cyclophosphamide therapy. Arch Path Lab Med 1991; 115:1049 Bigotti G, Coli A, Prisco LA, Spina C, Russo F, Castri F, Massi G. Rare presentation of carcinosarcoma arising in bladder diverticulum. Dept. of Pathology, Catholic University of Sacred Heart, Rome, Italy J Exp Clin Cancer Res. 2001 Jun;20(2):301-4. Baschinsky DY, Chen JH, Vadmal MS, Lucas JG, Bahnson RR, Niemann TH. Carcinosarcoma of the urinary bladder--an aggressive tumor with diverse histogenesis. A clinicopathologic study of 4 cases and review of the literature. Arch Pathol Lab Med. 2000 Aug;124(8):1172-8. Gonzalez-Carrero J, Nogueira March JL, Ojea A, Figueiredo L, Jamardo D, Guate JL, Cunqueiro R. Carcinosarcoma and papillary transitional cell carcinoma coexisting in the same bladder. Actas Urol Esp. 1990 JulAug;14(4):286-8. CTTR’s Case of the Month June, 2005 3 Li Y, Outman JE, Mathur SC. Carcinosarcoma with a large cell neuroendocrine epithelial component: first report of an unusual biphasic tumour of the urinary bladder. J Clin Pathol. 2004 Mar;57(3):318-20. Zuck erberg LR, Armin AR, Pisharodi L, Young RH. Transitional cell carcinoma of the urinary bladder with osteoclast-type giant cells: a report of two cases and review of the literature. Histopath 1990; 17:407. Young RH, Rosenberg AE. Osteosarcoma of the urinary bladder: Report of a case and review of literature. Cancer 1987; 59:174-8. Ro JY, El-Naggar AK, Amin MB, Sahin AA, Ordonez NG, Ayala AG. Pseudosarcomatous fibromyxoid tumor of the urinary bladder and prostate: immunohistochemical, ultrastructural, and DNA flow cytometric analyses of nine cases. Hum Pathol 1993; 24:1203. Perret L, Chaubert P, Hessler D, Guillou L. Primary heterologous carcinosarcoma (metaplastic carcinoma) of the urinary bladder: a clinicopathologic, immunohistochemical, and ultrastructural analysis of eight cases and a review of the literature. Cancer1998; 15(82)1535-49. Sarel Halachmi, Angelo M. DeMarzo, Nan-Haw Chow, Naomi Halachmi, Ann E. Smith, Jurgen F. Linn, Ofer Nativ, Jonathan I. Epstein, Mark P. Schoenberg, David Sidransky . Genetic Alterations in Urinary Bladder Carcinosarcoma: Evidence of a Common Clonal Origin. European Urology 2000;37:350-357. CTTR’s Case of the Month June, 2005 4