Guy`s and St Thomas` stroke service referral form
advertisement

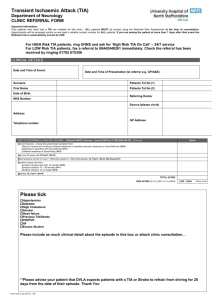
Lambeth / Southwark TIA Referral Form Clinical Referral email: gst-tr.gsttstrokereferrals@nhs.net St Thomas’ Clinical Fax Referral: 0203 2998504 King’s Date / Method of Referral: Date of referral __/__/____ Patient details Name: Address: Date of birth: __ / __ / ____ Tel Home: Mobile: Tel: Fax: Hemiparesis / leg weakness Loss of sensation Loss of speech Vertigo Double vision Loss of co-ordination Present Right Left Heart failure Diabetes AF PVD C = Clinical Features D = Duration of Symptoms D = Diabetes History of Treatment / Other Relevant Information / Smokes Obesity Previous Stroke/ TIA Migrane Other True aspirin intolerance: Yes No ABCD2 Score A = Age B = BP Other Blood Pressure Date of symptoms: Duration of symptoms to complete resolution: Past medical history / Vascular risk factors Hypertension Hyperlipidaemia Isch. Heart Disease Patient GP Details Name: Address: Clinical features Hemiparesis /arm weakness GP Score >60 >140 Systolic and/or 90 Diastolic Unilateral Weakness Speech disturbance w/o weakness Other >60 minutes 10 – 59 Minutes < 10 Minutes Diabetes Current Medications *Give patient stat dose 300mg aspirin daily, unless contra indicated (e.g. on warfarin) and provided all symptoms have resolved Patient Score Patient Advice 1 1 Tell the Patient: 2 1 -He or she should not drive until he or she has been assessed at hospital or clinic 0 2 1 0 1 -If there was a witness to the event, that person should accompany the patient to the hospital or clinic 2 -If the patient experiences any further event he or she should go immediately to A&E Total ABCD Score Referral Information Guy’s and St Thomas’ NHS Foundation Trust King’s College Hospital NHS Foundation Trust Send to St Thomas’ A&E if any of the below apply: ABCD2 Score ≥4 ≥ 1 TIA in a week On Warfarin or in AF (Atrial Fibrillation) < 50 yrs, with prominent neck pain / headache Send to King’s A&E if any of the below apply: ABCD2 Score ≥4 ≥ 1 TIA in a week On Warfarin or in AF (Atrial Fibrillation) < 50 yrs, with prominent neck pain / headache Refer to GSTT TIA Clinic via email if ABCD2<4 and TIA suspected (Monday P.M. & Thursday A.M.) If no to all of the above, call TIA Nurse/ stroke on call registrar for next day admission to PIU (Patient Investigation Unit) and fax referral form. Team Secretary (appointments, chase referral) 0207 1882515 TIA Referral email: gst-tr.gsttstrokereferrals@nhs.net Stroke Team via St Thomas’ Switchboard 0207 1887188 (bleep 1765) Prof Rudd, Dr Bhalla, Dr Birns. Refer to King’s TIA Clinic via fax, if symptoms occurred > 72 hours earlier (Tuesday A.M.) TIA Nurse: 07528977503 TIA Referral Fax: 020 3299 8504 Stroke Registrar via King’s Switchboard: 020 3299 9000 IF SYMPTOMS PERSIST THROUGH CLINICAL ASSESSMENT THEN BLUE LIGHT TO NEAREST A & E.