Lopez - Direct Blood Pressure Measurement
advertisement

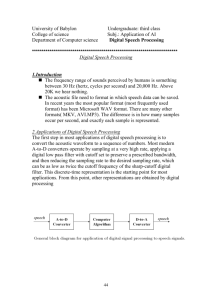
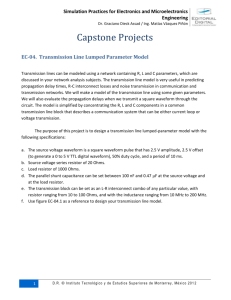
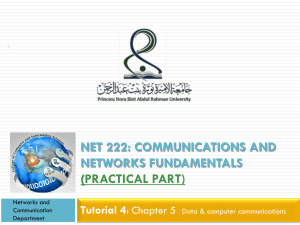
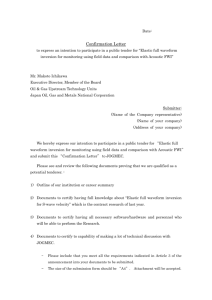
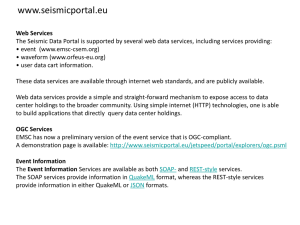
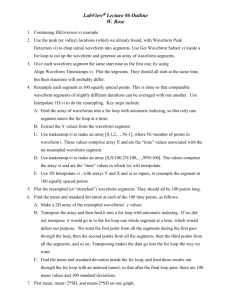
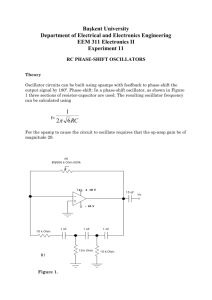
1 Direct Blood Pressure Measurement Raquel Lopez, Candidate for M.A.Sc.- Clinical Engineering, Institute for Biomaterials and Biomedical Engineering Abstract— Direct blood pressure measurement is critical for the treatment, diagnosis, and monitoring of critically ill patients. The system investigated herein to measure direct blood pressure, is a catheter-transducer system comprised of: a catheter (fluidfilled sensor), pressure transducer, amplifier, analog-to-digital converter, and a processor with display. The dynamic response components (natural frequency and damping coefficient) of this damped, second-order system define the pressure waveform accuracy. Studies conducted, namely by Gardner and Van Genderingen, determined the relationship between dynamic response components and accuracy. It was found that for patients with a normal resting heart rate, the absolute minimum natural frequency of the system leading to an accurate waveform was 7Hz, occurring at a damping coefficient of 0.5. For patients with high resting heart rates, such as neonates, the absolute minimum natural frequency of the system is 4Hz, also occurring at a damping coefficient of 0.5. To ensure that the dynamic response components do not fall out of the accurate damping range, the following procedural steps need to be addressed during the setup and operation of the catheter-transducer system: priming and monitoring of system components, zeroing, leveling, and dynamic response testing. Index Terms— invasive blood pressure measurement, arterial pressure waveform, dynamic response components I. INTRODUCTION T HE most accurate method of measuring blood pressure is by its direct measurement via an intravascular sensor device. For routine physical exams, this method is not practical due to its invasive nature however, for treatment, diagnosis, and monitoring of critically ill patients, invasive blood pressure measurement is inherent. In particular, arterial pressure (AP) is monitored as it correlates to system perfusion and consequently, it is an excellent indicator of the response to a treatment or surgical procedure. Further, an AP waveform provides continuous information on the pumping action of the heart, such as valve closure and systolic and diastolic arterial pressures. Since the accuracy of this AP waveform is more so limited by the dynamic response of the hydraulic system (tubing, stopcocks, and catheter) than by the electronic equipment of the system (amplifier, processor), the need to control the hydraulic system is more prominent. The purpose of this report is to present the optimal dynamic response components (natural frequency and damping coefficient) of the hydraulic system that ensure waveform accuracy. It further aims to discuss factors influencing these components and clinical methods to address such factors. II. BACKGROUND A. Catheter-Transducer System Direct blood pressure is typically measured by means of a catheter-transducer system (Figure 1). The catheter serves to provide access to the artery and also detects the pressure waves generated therein by cardiac contraction. It may be a fluid-filled or solid pressure probe. Solid probes, although less subject to error, are more difficult to implant and more expensive. Consequently, fluid-filled catheters are more commonly used. Within these, the pressure wave is transmitted via fluid-filled tubing and stopcocks to the sensing diaphragm of the pressure transducer. The transducer converts this mechanical signal into an electrical one. In blood pressure monitoring, the transducer has a silicon wafer diaphragm which when deformed, produces an alteration in electrical resistance. The altered resistance is measured by a Wheatstone bridge and propagated by a transmitter to an amplifier. Filters are usually found within the amplifier to minimize waveform noise. The signal is then converted at an analog-to-digital converter. It is transmitted to a processor that calculates other hemodynamic parameters, such as mean arterial pressure, based on the measured variables. Finally, the signal is displayed on a monitor in its analog form along with its digital output. To produce minimal error in the arterial pressure waveform, this catheter-transducer system needs to be accurate, sensitive, linear, and have minimal drift. This report focuses on the major contributor to inaccuracy, the hydraulic system. It does not discuss inaccuracy attributed to the electronic system (signal conditioning unit) for the reason that (i) it is not as significant a contributor and (ii) in terms of clinical use of the catheter-transducer system, it is the hydraulic system that can be most affected by user error. [1] Pressure Transducer Pressure Sensor (Fluid-filled Catheter) Transmitter Signal Conditioning Unit Amplifier Analog-toDigital Converter Processor & Monitor Figure 1: Schematic of Catheter-Transducer System Process B. The Typical Arterial Pressure Waveform The typical arterial pressure waveform for the cardiac cycle of a healthy individual is depicted in Figure 2. The following cardiac parameters are some of which can be interpreted 2 directly from the waveform: systolic pressure, diastolic pressure, pulse pressure, dicrotic notch pressure, heart rate, and ejection time. Systolic arterial pressure is that pressure exerted on the artery walls due to contraction of the left ventricle of the heart. Diastolic pressure is pressure exerted on the walls due to relaxation of the left ventricle. The normal range of systolic pressure is 110-140mmHg and that of diastolic pressure is 60-90mmHg. [2] Pulse pressure is the difference between the peak systolic and diastolic pressures. The dicrotic notch pressure is the pressure reflecting the closure of the aortic valve which leads to some backflow of blood in the artery downstream the valve. Heart rate is the frequency of contraction, measured in beats per minute. Ejection time is the time of left ventricle blood ejection. Examples of when these parameters are significant include: diagnosis of such diseases as hypertension, drug therapy for atherosclerosis patients, and monitoring success of implantable medical devices. P2 ( f ) P1 ( f ) 1 2 f f 2 j 1 2 Fn Fn (1) D. Factors Affecting Pressure Waveform Dynamic Response Components The dynamic response waveform components, natural frequency and damping coefficient, can be affected by three mechanical factors, leading to an error in pressure waveform of as much as 50 percent. [4] These factors include: compliance (C), fluid inertia (I), and fluid resistance (R). Compliance refers to the flexibility of the pressure transducer diaphragm and the system tubing. Fluid inertia refers to the coefficient related to the pressure needed to accelerate the liquid through the tubing. Fluid resistance refers to the viscosity of the fluid in the tubing and the friction at the walls of the tubing. [1],[3],[5] Given the values for C, I, and R, Equation (2) can be used to determine Fn Fn and . [1] 1 2 IC (2) R C 2 I Figure 2: Typical Arterial Pressure Waveform [2] C. Pressure Waveform Dynamic Response Components The catheter-transducer system can be modeled as a secondorder dynamic system. [1],[3] This means that the pressure waveform transmitted to the diaphragm of the transmitter via fluid-filled tubing dampens, such that with each successive pulse, its amplitude decreases. There are two dynamic response components of a waveform: natural frequency and damping coefficient. The natural frequency of a system is its number of oscillations per unit time occurring without any damping. The damping coefficient is related to the time taken to dampen the waveform. The transfer function that allows the calculation of the output transducer signal (in mV) from an input transducer signal (mmHg) is of second order. Equation (1) shows the second-order transfer function, where P1 , P2 are These values when substituted back into the transfer function, determine the arterial pressure waveform for any frequency. The resulting damping coefficient deems if the system is underdamped, overdamped, or optimally damped. In an underdamped system, the pressure waves tend to reverberate within the catheter and tubing leading to formation of wave reflections or harmonics. These harmonics are additive and lead to the overestimation of systolic pressure and underestimation of diastolic pressure. In an overdamped system, frictional forces impede the arterial waveform such that it loses energy. Figure 3 depicts a schematic of an arterial waveform in an (a) underdamped and (b) overdamped system. Notice that underdamping leads to a narrow, peaked tracing which overestimates systolic pressure and underestimates diastolic pressure while overdamping leads to a broad, flattened waveform which underestimates systolic blood pressure and overestimates diastolic blood pressure. (a) (b) output and input signals of the pressure transmitter, Fn is the natural frequency, is the damping coefficient, and j is the complex respectively, f is an arbitrary frequency, number. [1] Figure 3: Damping Affect on Arterial Pressure Waveform: (a) Underdamped Waveform and (b) Overdamped Waveform (SBP – systolic blood pressure; DBP – diastolic blood pressure) [6] 3 1.2 1.1 1.0 .8 .7 Unacceptable .6 .5 .4 Optimal . .2 .3 Damping Coefficient .9 Overdamped Adequate Underdamped .1 A catheter-transducer system accurately measures arterial pressure waveform if its dynamic waveform components (natural frequency and damping coefficient) are accurate. In other words, if the system is accurate, a pressure waveform can return to its baseline waveform after being perturbed. Studies by Gardner and Van Genderingen determined the effect of dynamic waveform components on system accuracy. [1],[7] Van Genderingen investigated these effects for systems requiring a quick response, such as systems for measuring neonatal arterial pressure. These systems are required to detect waveforms resulting from high resting heart rates (150230 beats per minute). [5] Gardner investigated the effects of dynamic waveform components on accuracy for systems requiring a response to normal resting heart rates (50-100 beats per minute). Both studies used pressure simulators to generate waveforms of different natural frequency and damping coefficients and recorded the extent to which the perturbed waveform differed from the original one. The method of perturbation used is known at the square wave test or the fast-flush test. In this test, a square pulse in pressure waveform is generated by opening and closing the flush valve. Subsequently, the flow through the catheter-transducer system is acutely increased and generates an acute rise in pressure within the system in the form of a square wave. A system with appropriate dynamic response components will return to the baseline waveform within one to two oscillations. Figure 4 shows the relationship between natural frequency and damping coefficient for a system requiring normal dynamic response. It describes a range of natural frequency and damping coefficient combinations that are required for an optimally damped system. An optimally damped system has a high natural frequency to allow for the largest possible range in damping coefficients. Commonly, for systems not requiring a fast response, natural frequencies greater than 30Hz are accurate, meaning that they yield an arterial pressure that is within 1mmHg of the true pressure. [1] Further, the absolute minimum natural frequency that can lead to an adequate pressure waveform is 7Hz. A damping coefficient of 0.5 is an adequate level of damping for the widest range of natural frequencies. [1] Figure 4 shows the relationship between natural frequency and damping coefficient for systems requiring a fast or high dynamic response. Error of 2 percent in arterial pressure waveform is considered to be small and as such, acceptable, whereas error greater than 10 percent is excessively large and is unacceptable. [7] Note that a 2 percent error translates to an error in arterial pressure of 3-4.6mmHg, which is greater than the error permitted for lower dynamic response systems (1mmHg). This is the case since fluid-filled cathetertransducer systems that require a fast response are affected more heavily by compliance, fluid inertia, and fluid resistance than solid probe systems. Consequently, the aim of recently developed solid probes is to combat error in arterial pressure measurement for high dynamic response systems. Figure 5 shows that an absolute minimum natural frequency that can lead to an accurate pressure waveform is 4Hz. In general, for systems requiring a fast response, natural frequencies greater than 60Hz are accurate. A damping coefficient of 0.5, as in Gardner’s study, is also an adequate level of damping for the widest range of natural frequencies. [7] In general, for both systems, as the natural frequency decreases, the requirement for damping coefficient is less than 1. This indicates that the second-order dynamic system is a damped one. 0 III. ACHIEVING AN ACCURATE PRESSURE WAVEFORM 0 5 10 15 20 25 30 35 40 45 Natural Frequency (Hz) Figure 4: Degree of Pressure Waveform Damping as a Function of Natural Frequency and Damping Coefficient for Patients with a Normal Heart Rate [1] Figure 5: Percentage Error in Pressure Waveform as a Function of Natural Frequency and Damping Coefficient for Patients with a High Heart Rate [7] IV. DISCUSSION - QUALITY ASSURANCE TO ACHIEVE ACCURATE DYNAMIC RESPONSE COMPONENTS The catheter-transducer system obtained from the manufacturer has a set natural frequency value. Yet, the compliance, fluid inertia, and fluid resistance factors that affect natural frequency and damping coefficient vary with 4 system setup and use. This variation needs to be controlled by the user to assure high quality arterial pressure waveform measurement. The following procedural steps should therefore be followed with every patient being measured: (1) priming and monitoring of system components, (2) zeroing and (3) leveling or referencing the transducer, and (4) dynamic response testing. [5],[6],[8] 1) Priming and Monitoring System Components The presence of air bubbles in the system as well as any blood clotting at the tip of the catheter both contribute to overdamping of the pressure waveform. An overdamped waveform leads to an underestimation of systolic blood pressure and an overestimation of diastolic blood pressure. Air, an incompressible fluid, acts as a shock absorber that dampens the waveform, subsequently producing erroneous pressure values. It affects the resistance of the fluid by altering its viscosity. Air bubble entrapment is a high-risk source of error as (i) even air bubbles measuring 1 mm in diameter can cause substantial waveform distortion and (ii) they can occur at many locations throughout the system.[6] Consequently, airfree priming of the entire system is one of the most important steps in avoiding technical error. It includes the following checks: tightening of all connections, closing stopcocks to air, avoiding multiple stopcocks and injection ports, and periodically flicking and flushing all tubing and stopcocks to eliminate tiny air bubbles escaping the flushing solution. In particular, special monitoring of tubing, stopcocks, interconnectors, and the transducer needs to be conducted as these locations are prone to air entrapment. Also, the use of tubing that is as short as practically possible is advised, as this decreases the number of possible locations of air bubble occurrence. If a patient is having their arterial pressure monitored for an extended period of time, the likelihood that blood clotting at the tip of the catheter will occur is increased.[6] As such, the catheter should be visually inspected and flushed regularly. The physical properties of the tubing also affect the transmission of the pressure waveform. If the tubing is overly compliant, the pressure waveform will be overdamped. If the diameter of the tubing is too large (greater than 1x10 -3), optimal damping cannot be achieved. [8] Thus, as a general rule, stiffer, shorter, and narrower tubing produces improved accuracy of the pressure waveform. 2) Leveling For each arterial pressure monitoring session, the equipment must be setup such that an accurate reference point from which all subsequent measurements is established. This reference point refers to the position of the air-fluid interface of the catheter-transducer system (the stopcock attached to the top of the transducer) that is to read atmospheric pressure. For arterial pressure monitoring, this height corresponds to the patient’s right atrium of the heart. Clinical personnel approximate it externally by an anatomical landmark called the phlebostatic axis. In the event that the transducer is placed below the phlebostatic axis, the resulting arterial pressure waveform will be inaccurately high. Conversely, the arterial pressure waveform is erroneously low if the transducer is higher than the phlebostatic axis. [5] 3) Zeroing Zeroing ensures that the catheter-transducer system assigns the air-fluid interface as the reference point measuring atmospheric pressure. This is done by opening a stopcock to atmospheric pressure, and, as with most instrumentation, selecting ‘zero’ from the console. Zeroing eliminates zerodrift, which is the potential, usually minimal, transducer offset or distortion occurring over time. A pressure monitoring system should be zeroed regularly. [5] 4) Dynamic Response Testing To determine if dynamic response components have been altered throughout the course of system setup and use, a square wave test like that used by Gardner and Van Genderingen should be performed. If dynamic response components are inadequate, that is if after perturbation the waveform does not return to its original waveform within one or two oscillations, the above procedural steps should be readdressed. [6] In general, in order to achieve accurate arterial pressure measurements, it is essential that the catheter-transducer system have a high natural frequency, be suitably damped, properly zeroed, appropriately referenced, and regularly tested for dynamic response. V. CONCLUSIONS Direct pressure monitoring is essential for determining immediate changes in a patient’s blood pressure values. The waveform offers valuable diagnostic, treatment, and surgical monitoring information. Yet, if not accurate, erroneous data in the arterial pressure waveform can potentially lead to detrimental treatment. For systems required to respond to normal heart rates, the minimum natural frequency ensuring accuracy is 7Hz. For high dynamic response systems, this frequency is 4Hz. In both systems, the damping coefficient that permits the widest range of natural frequencies is 0.5. Clinical personnel need to be aware of these dynamic response components leading to optimal damping and consequently accurate waveforms. Their involvement in system setup (priming, leveling, zeroing) as well as regular dynamic response testing is critical to quality assurance of the measured arterial pressure waveform. These findings are a significant benchmark in physiological measurement and pave the way for direct blood pressure measurements of the ventricles and atria, as well as pressure measurement of other fluids such as the craniocerebral fluid. 5 REFERENCES [1] [2] [3] [4] [5] [6] [7] [8] Gardner, RM. “Direct blood pressure measurement: dynamic response requirements”. Anesthesiology. Volume 54, No. 3, pp. 227-236. March 1981. Hebert, JL., et al. “The Relation between Aortic Dicrotic Notch Pressure and Mean Aortic Pressure in Adults”. American Journal of Cardiology. Volume 76. No. 4, pp. 301-306. August 1995. Taylor, BC. “Frequency Response Testing in Catheter-Transducer Systems”. Journal of Clinical Engineering. Volume 15, No. 5, pp. 395407. September 1990. Taylor, BC., Donavan, F. “Hydraulic Resistance and Damping in Catheter-Transducer Systems”. IEEE Engineering in Medicine and Biology. pp. 72-78. December 1992. Promonet, C. et al. “Time-dependent Pressure Distortion in a Catheter– Transducer System: Correction by Fast Flush”. Anesthesiology. Volume 92, No. 1, pp. 208-218 January 2000. Cheatham, M. “Hemodynamic Monitoring: Dynamic Response Artifacts”. Surgical Intensive Care Units Orlando Regional Medical Center. Online: 5 July 2002. http://www.surgicalcriticalcare.net/Lectures/dynamic_response.pdf Van Genderingen, HR. “Intra-arterial Pressure Measurement in Neonates: Dynamic Response Requirements”. Physiology Measurement. Volume 16, pp. 55-61. 1995. McGhee, BH., Bridges, MEH. “Monitoring Arterial Blood Pressure: What You May Not Know”. Critical Care Nurse. Volume 22, No. 2, pp. 60-78 April 2002.