-----------------------------------------------------------------------------------------------------------------REPORT OF THE MONTH, Volume III, Number 6 – November - December 1999
- - - - from the North Carolina Statewide Program for Infection Control and Epidemiology
-----------------------------------------------------------------------------------------------------------------CONTENTS:
NEWS FEATURES
JCAHO and FDA Comment on Reuse of Single Use Items
Infection Control Measures That Reduce Transmission of VRE
REGULATORY/LEGISLATIVE
Tuberculosis in North Carolina: Epidemiology and New Therapy Guidelines
QUESTION OF THE MONTH
Blood-Contaminated Medical Records
NEWS AND ANNOUNCEMENTS
COURSES FOR THE INFECTION CONTROL PROFESSIONAL
News Features
JCAHO and FDA Comment on Reuse of Single Use Items
Reprocessing of medical devices listed by the manufacturer as for “single use” has
been identified as a hot spot for the year 2,000 JCAHO surveys (Inside the Joint
Commission, November 15, 1999). JCAHO recommends the following three steps on
the reuse of single use medical devices: 1) don’t do it unless you can support your
hospital’s decision; 2) decide if you will charge less for a reused item compared to a
new item; 3) provide patients with a choice to use a single use or reused device.
Additionally, the Food and Drug Administration has announced the availability of a
document that describes the agency's proposed strategy on the reuse of single use
devices. This document can be obtained via the web (www.fda.gov/cdrh). The FDA is
requesting comments on their proposed approach to regulation of single use devices
Infection Control Measures That Reduce Transmission of VRE
The use of enhanced infection control measures (15 specific interventions) to reduce
the incidence of VRE colonization and infection was assessed in a 22-bed adult
oncology unit. Historic controls were used and the interventions were implemented
simultaneously. Interventions included the following: gown and glove use on room
entry for all patients colonized/infected with VRE, gown and glove use on room entry for
all patients whose VRE status was unknown, infectious disease consultation for
patients with persistent fevers, surveillance cultures of all new admissions, and weekly,
spatial separation of patients into three cohorts (VRE positive, VRE negative, VRE
unknown), VRE-unknown patients housed on a separate unit until status clarified, and
environmental cultures in VRE-positive patient rooms before and after patient discharge
and room disinfection. Enhanced infection control measures were associated with a
decrease in VRE-associated bloodstream infections from 2.1 patients per 1,000
patients-days to 0.45 patients per 1,000 patient-days (relative rate ratio 0.22, p=0.04)
and a decrease in VRE colonization from 20.7 patients per 1,000 patient-days to 10.3
patients per 1,000 patient-days (relative rate ratio 0.5, p<0.001). In conclusion,
enhanced infection control measures were associated with a decreased incidence of
VRE colonization and bloodstream infections, and use of all antibiotics with the
exception of clindamycin and amikacin. The relative importance of each of the 15
interventions was not assessed.
Regulatory/Legislative
Tuberculosis in North Carolina: Epidemiology and New Therapy Guidelines
In 1997, 19,855 cases of tuberculosis (TB) were reported in the United States, for a rate
of 7.4 per 100,000 persons. For the same time period, 462 cases were reported in
North Carolina, for a rate of 6.2. Reported TB cases by race included: Black 61.9%,
White 32.5%, Asian 5.2%, and Native American 0.4%.
New evaluation and treatment guidelines are available from the NC TB Control Branch
(919-733-7286). The need and frequency of tuberculin skin testing required depends
on an assessment of transmission risks within the healthcare facility (see below). In
addition, indications for the therapy of latent lower respiratory tuberculous infection
(LRTI) in healthcare workers depend on this risk assessment. Candidates for therapy
for latent tuberculous infection include in addition to standard CDC recommendations
for healthcare workers under 35 years of age with >10mm PPD in occupational settings
classified as low, intermediate or high risk and with >15 mm PPD in occupational
settings classified as minimal or very low.
In the next issue we will review new recommendations for the drug therapy of latent
lower respiratory tuberculous infection. Please note that this is the preferred
terminology replacing “prophylactic therapy” because it emphasizes that therapy is
being offered to persons with latent infection in order to prevent the development of
active tuberculous disease.
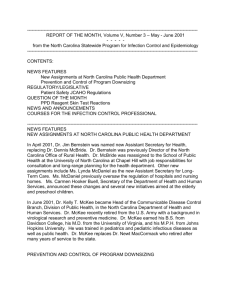
Risk Classification
Minimal
Very Low
Low
Intermediate
High
Tuberculin Skin Test (TST) Requirements
Annual TST NOT required
No infectious TB cases in county in the past year and
No infectious TB cases seen in the facility in the past year
Annual TST NOT required
TB cases in county in the past year and
No infectious TB cases seen in the facility in the past year and
No evidence of transmission among patients or workers
Annual TST required
TB cases in county in the past year and
<6 TB cases seen in the facility in the past year and
No cluster* of HCW TST conversions and
No evidence of transmission among patients or workers
Annual TST required
TB cases in county in the past year and
>6 TB cases seen in the facility in the past year and
No cluster* of HCW TST conversions and
No evidence of transmission among patients or workers
Annual TST required every 3 months
TB cases in county in the past year and
>6 TB cases seen in the facility in the past year and
Cluster* of HCW TST conversions and
Evidence of transmission among patients or workers
*Two or more TST conversions within a 3 month period among HCWs in a specific area or occupational
group
Question of the Month
Blood-Contaminated Medical Records
Q:
What should be done if medical records become blood-contaminated?
A:
The concern is to prevent the spread of bloodborne pathogens. In the literature
there is one report that blood-contaminated laboratory file cards led to the transmission
of hepatitis B among laboratory technicians. Hepatitis B can survive for up to 30 days
in dried blood. HIV has been found to die off at 1 log every 9 hours (i.e., 100 infecting
virus particles to 10). At UNC Hospitals, blood contaminated pages would first be
placed into plastic sleeves and photocopied until the original pages could be ETO
sterilized. Unfortunately, the pages would continue to look contaminated due to the
bloodstains and could alarm someone who may handle them in the future. These
pages could either be stamped "sterilized" or "decontaminated" or placed in clean,
plastic sleeves and so labeled.
ANNOUNCEMENTS
The Occupational Safety and Health Administration issued a new directive, Compliance
Directive CPL 2-2.44D on November 5, 1999. This document revises the Bloodborne
Pathogens Compliance Directive issued in 1992 and will help minimize serious health
risks faced by workers exposed to blood and other potentially infectious materials. The
document is available online at http://www.osha.gov/
The Occupational Safety and Health Administration issued a proposed new ergonomics
standard in the Federal Register, November 23, 1999. The document is available online at
http://www.osha.gov/
COURSES FOR THE INFECTION CONTROL PROFESSIONAL
"Infection Control Part I: Clinical Surveillance of Nosocomial Infections" will be held April
10-14, 2000 at the Holiday Inn in Chapel Hill.
"Infection Control in Long-Term Care Facilities" will be held April 26-27, 2000 at The
Friday Center in Chapel Hill.
-----------------------------------------------------------------------------------------------------------------Contributors to Report of the Month: Karen K. Hoffmann, RN, MS, CIC; William A.
Rutala, PhD., MPH., Eva P. Clontz, MEd.
-----------------------------------------------------------------------------------------------------------------To subscribe to the Report of the Month, send email to
spice@unc.edu
Report of the Month is also available on the home page of the Statewide Program for
Infection Control and Epidemiology at http://www.unc.edu/depts/spice/
The Statewide Program for Infection Control and Epidemiology (SPICE) is funded by
the General Assembly of North Carolina to serve the State. SPICE is not a regulatory
agency but provides education and consultation to North Carolina healthcare facilities.
Copyright 1999 Statewide Program for Infection Control and Epidemiology
 0
0