Clinical Relevance of Straylight Assessment - Nin
advertisement

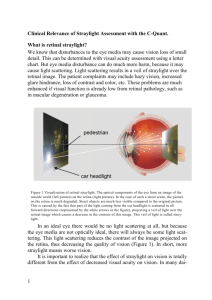
Clinical Relevance of Straylight Assessment It has long been realized that “20/20 is not enough”. Contrast sensitivity was added to better assess full quality of vision. But also contrast sensitivity is not enough. Severe complaints exist that are missed with visual acuity and contrast sensitivity. How can this be understood? The answer lies in the large “dynamics” of the human eye, as illustrated in figure 1. Figure 1 shows the point-spreadfunction of the normal human eye. It gives the light distribution that follows from a point source of light. It shows that a point source does not project on the retina as a point, but strongly spread-out. The spreading of light is caused by several essentially different optical errors of the eye. The point-spread-function dictates the effects of imperfect eye optics on vision. This has been studied over the years in many publications. Different domains can be identified in the point-spread-function. Ideally, the light distribution should only be the central peak up to 1 minute of arc, shown in red. This area dominates visual acuity. The next area goes on to 10 minutes of arc (the blue area), which dominates contrast sensitivity (6cpd corresponds to 5 minutes of arc band width). However, the light spreading continues over the full retina. The light spreading over 60 minutes of arc (1 degree) and more is called straylight. Every area of this point-spread-function is equally important for quality of vision. Visual acuity 1 min of arc => 0.02º Contrast sensitivity 18..3 cycl/degree => 0.06..0.33º Straylight => 1..30º Figure 1 The point-spread-function of the human eye. When the eye looks at a point source, the actual light distribution spreads out over the full retina. Different domains of this distribution are indicated, dominating different aspects of visual function. Small angle disturbances to the eye media may cause vision loss of small detail, determined with visual acuity assessment using a letter chart or contrast sensitivity. But how does the light scattered over larger distances affect vision? The light scattered results in a veil of straylight over the retinal image, see figure 2. The patient complaints may include hazy vision, increased glare hindrance, loss of contrast and color, etc. If concomitant retinal pathology exists, as macular de1 generation, retinal dystrophy or glaucoma, the problems experienced from straylight are much enhanced, calling for extra attention on straylight in such patients. Figure 2 Visualization of retinal straylight. The optical components of the eye form an image of the outside world (left pi cture) on the retina (right picture). In the case of such a street scene, the picture on the retina is much degraded because part of the light coming from the car headlight is scattered in all forward directions (white arrows in the figure), projecting a veil of light over the retinal image. This veil of light is called straylight. A new instrument. Recently a new instrument was introduced to assess straylight in clinical settings (C-Quant instrument from Oculus, figure 3). The measurement is easy. It takes about 1.5 minutes per eye. There are 25 short presentations the patient must respond to by pressing a button. Population norms are developed based on 5,000 normal eyes. The norms show straylight to increase with aging, doubling at 65, and tripling at 77 years of age. To date experience has been built up for large numbers of patients, comprising cataracts, PCO, refractive surgery, contact lenses, etc. Media disturbances were found to give increase in straylight by a factor of ten and more. 2 Figure 3. The C-Quant instrument from Oculus for measuring the amount of straylight in patient eyes. Straylight and visual function. Straylight gives a direct functional aspect of the eye, as opposed to optical measures. This is done with one simple figure, the “straylight parameter”. The corresponding complaints may be expressed, as hazy vision, increased glare hindrance, loss of contrast and color, halos around bright lights, and difficulties with against-the-light face recognition. It varies with individual which complaints are most important. Glare sensitivity. The primary effect of straylight is reduction of retinal contrast in areas of relatively low brightness. Best known example is blinding by head lamps at night. This has been called “disability glare”. The international standards committee CIE, has defined disability glare to be synonymous with straylight, because studies showed straylight to be a precise predictor of these phenomena. Visual acuity. Visual acuity and straylight are very different aspects of visual quality. This can be understood because straylight concerns light scattering over larger angles (1 to 90 degrees), whereas visual acuity is determined by light deflections over small angles (<0.1 degree, more commonly called aberrations). Moreover straylight is determined by very different anatomical/morphological aspects of the optical media. So, changes in the one domain do not necessarily mean changes in the other domain. This can be illustrated with simple experiments. Putting a +2 dpt trial lens in front of a subject’s eye will definitely change the subject’s visual acuity, whereas his straylight value will stay precisely the same. As opposite example, a fog filter in front of the subject’s eye will give a dramatic increase in straylight, whereas visual acuity may hardly change. Contrast sensitivity. The relation between straylight and contrast sensitivity is a matter of much confusion. A contrast sensitivity test does not reliably show straylight effects much for the same reasons as mentioned for visual acuity. Figure 1 illustrates why contrast sensitivity is closer to visual acuity than to straylight. Large population studies showed the same. Clinical use of straylight assessment 3 Cataract extraction or straylight lens exchange. When cataracts starts to develop, often the first complaints are from increased straylight, as listed above, with visual acuity still good. Visual acuity is however somewhat of the Holy Grail of ophthalmology. But if straylight is high, you can also offer surgery to relieve the patient. An asset of straylight is that you know for sure it is caused by the optical media, and that your patient will benefit from surgery. With visual acuity loss, such is not always the case. We studied the relative benefits of cataract surgery for visual acuity and straylight, and found for the present practice already that straylight improves more than visual acuity: Visual acuity by a factor 1.7, but straylight by a factor 3. Cornea. Studies are showing this difference to be even greater in major corneal conditions (dystrophies, contact lens related problems). Refractive lens exchange and refractive surgery. In case of refractive procedures a risk exists of increasing straylight by surgery or IOL related factors. So it would be wise to assess straylight before deciding for surgery. If straylight is nicely low, the postoperative outcome may be disappointing for your patient in case straylight increases as side effect of the surgery. If preop straylight is high, you are quite safe. TJTP van den Berg, PhD Netherlands Inst. Neuroscience, Royal Academy www.nin.nl t.j.vandenberg@nin.knaw.nl Disclosure statement: The Royal Academy owns a patent, licensed to Oculus GmbH for marketing the C-Quant straylight meter. -----------------------------------------------------------------------------------------------Optional. Not necessary to include. Reference van den Berg TJTP, van Rijn LJ, Michael R, et al.: Straylight Effects with Aging and Lens Extraction. Am J Ophthalmol, 2007 Cervino A, Montes-Mico R, Hosking SL: Performance of the compensation comparison method for retinal straylight measurement: effect of patient's age on repeatability. Br J Ophthalmol 92:788-791, 2008 4