TRANSFUSION REACTION CASES
advertisement

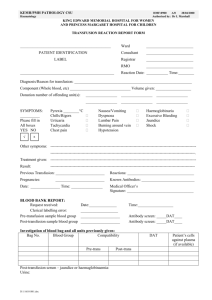
TRANSFUSION REACTION CASES Case Study #2 Three young men were simultaneously transported by ambulance to a trauma center emergency department. All had sustained injuries in gang-related violence. One was awake and alert; the other two were unconscious and were given “John Doe” designations. The conscious patient, Trey B. Jones, was a rival gang member who denied knowing the other two victims. Patient Jones had a stab wound to the right leg that was bleeding minimally. John Doe 1 had sustained a gunshot wound to the abdomen, was unconscious and hypotensive, with fractures of the leg and pelvis. According to witnesses at the scene, he was shot while running into the street and was then struck by a hit-and-run driver. John Doe 2 was unconscious and bleeding profusely from multiple head and facial lacerations sustained from blunt trauma. He was extremely hypotensive, but there was no evidence of gunshot wounds to the face or head. The Blood Bank received three separate specimens labeled “John Doe 1”, “John Doe 2” and “Trey B. Jones”, with appropriately completed requisitions. Two units of packed red blood cells were ordered for John Doe 1 and also for John Doe 2. A type and antibody screen was ordered for Trey B. Jones. The technologists began compatibility testing and the following results were obtained on the submitted specimens: John Doe 1 John Doe 2 Trey B. Jones Anti-A 4+ 0 0 Anti-B 0 0 0 Anti-D 0 3+ 3+ Rh Con 0 0 0 A1 cells 0 4+ 4+ B cells 4+ 4+ 4+ The results of the antibody screen tests were negative on all three patients. The Blood Bank issued two units of group A, Rh-negative RBCs for John Doe 1 and two units of group O, Rh-positive RBCs for John Doe 2. John Doe 1, the most severely injured patient was to be taken to surgery, but the transfusion was begun in the emergency department. During the transfusion, a nurse noticed red urine draining into the patient’s Foley catheter bag. The Emergency Room physician speculated that the red urine might be due to the renal or lower genitourinary trauma. CLS 412 Clinical Laboratory Science Theory, Application and Correlation Transfusion Reaction Case #2 Page 1 1. Discuss three substances and their sources that would cause John Doe 1's red urine. What abnormalities would you expect to see macroscopically and microscopically in his routine urinalysis? 1. RBCs, from trauma, micro-intact RBCs 2. Free hemoglobin from intravascular lysis, micro- nothing 3. Myoglobin from tissue damage, micro - nothing *All will show red hazy urine macroscopically, positive blood dipstick and protein Pre-operative specimens on John Doe 1 were collected in the emergency department. The following laboratory results were obtained: Hematology WBC: 10.4 x 103/uL RBC: 2.96 x 106/uL Hgb: 8.0 g/dL Hct: 24.0 % MCV: 81.1 fL MCH: 27.0 pg MCHC: 33.3 g/dL Platelets: 80 x 103/uL Coagulation PT: PTT: Fibrinogen: D-dimer: 17.0 sec 52.3 sec 48 mg/dL Increased 2. What does this data indicate about John Doe 1's coagulation status? RBC, HGB, HCT Dec PLT Dec PT/PTT prolonged Fibrinogen Dec Pos D-Dimer Active bleeding, clotting, and lysing occurring = patient in DIC (confirm with dec. antithrombin and schistocytes on blood smear) John Doe 1's blood pressure and hemoglobin continued to drop during surgery, despite fluids, blood pressure agents and cardiac massage. Post-operatively he continued to bleed at the site. A transfusion reaction workup was ordered on John Doe 1. A new specimen was collected on John Doe 1 and delivered to the lab. The results were as follows: Recheck of patient identification: Confirmed correct Pre-sera inspection: Non-hemolyzed Post-sera inspection: Hemolyzed Patient type and direct Coombs, post-transfusion: Anti-A 0 Anti-B 0 Anti-D 3+ Rh Con 0 A1 cells 3+ CLS 412 Clinical Laboratory Science Theory, Application and Correlation Transfusion Reaction Case #2 B cells 3+ DAT w+ Page 2 3. What information about John Doe 1 justified the physician ordering a transfusion reaction workup after surgery? Patient was not responding to treatment, cannot clot, still bleeding from site, Low BP, decreased hemoglobin. Suspect HTR. 4. Are there any discrepancies in John Doe 1's transfusion workup? Explain your answer. ABO discrepancy, Pre-Sample A -, Post O+, has positive DAT 5. Based on your explanation to question #4, explain the correct confirmation of John Doe’s identification. John Doe 1 and John Doe 2 samples were most likely switched when drawn in the ER; the original sample labeled John Doe 1 is really from John Doe 2. John Doe 1 is really O+. Confirmation must be made by redrawing both patients and properly identifying both patients before drawing. 6. Specifically, what caused the serum drawn post-operatively to be hemolyzed? ABO incompatibility, the patient’s anti-A is attacking donor A antigen + cells and destroying them. 7. Can you make a valid comparison of the pre- and post-sera? Explain. No, the specimens are from different patients. 8. What are the AABB requirements for labeling compatibility testing specimens? Specimen labeled at bedside with 2 unique patient identifiers, date of collection, phlebotomist ID. 9. What type of transfusion reaction is John Doe 1 experiencing? Explain. Acute hemolytic transfusion reaction due to ABO incompatibility. Positive DAT, actively bleeding, hypotension, hemolyzed post transfusion sample (technically) 10. Indicate the expected results if these additional tests were performed on John Doe 1's posttransfusion specimen: a. Differential DAT (IgG DAT and C3 DAT): complement positive, and IgG positive b. Elution: anti-A present in eluate c. Plasma hemoglobin: increased (second lab value to change in an acute HTR) d. Haptoglobin: decreased (drops first) CLS 412 Clinical Laboratory Science Theory, Application and Correlation Transfusion Reaction Case #2 Page 3 11. At what point during the transfusion reaction would you expect to see the following? a. Hemoglobinuria: Immediately (seen once plasma hemoglobin level reaches 25mg/dl) Usually peaks at 3hrs b. Elevated bilirubin (indirect/unconjugated) Starts 3-6hrs, peaks at 6-7hours post transfusion c. Urine hemosiderin 12-18 hours and up to a month later (more useful in diagnosing delayed transfusion reaction) The next morning, John Doe 2 (now officially identified) required further transfusion. His emergency arm band had been removed so a new specimen had to be collected. It tested as follows: Anti-A 3+ Anti-B 0 Screen cell I Screen cell II Screen cell III Auto Anti-D mixed field Rh Con 0 37o/LISS 0 0 0 0 AHG 0 0 0 0 A1 cells 0 B cells 3+ CC 2+ 2+ 2+ 2+ 12. Are there any discrepancies in John Doe 2's new specimen? Explain your answer. Yes. Originally he was typed as O pos now showing A with a mixed field with anti-D reagent (which is usually strongly positive.) 13. What could be causing his mixed field reaction with Anti-D? Due to dual population. Patient is truly A neg but received O pos cells, so both Rh positive and negative cells present. 14. Explain why John Doe #2 is not apparently experiencing a transfusion reaction. Likely his first exposure to D antigen because he has not yet made anti-D antibodies. Treat with RhIG within 72 hours to neutralize D pos RBCs, and prevent anti-D formation. CLS 412 Clinical Laboratory Science Theory, Application and Correlation Transfusion Reaction Case #2 Page 4