Internal Ventral Cavity
advertisement

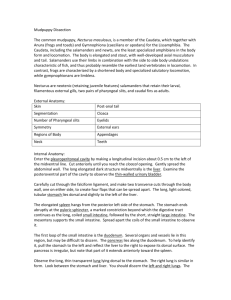
Cats Ventral Cavity Guide Cat Guts p. 1 The Ventral Cavity A. The trunk is divided into the thoracic region (anterior) and the abdominal (posterior) region. Each of these regions contains cavities, which ontologically are portions of the coelom (intramesodermal space). The thoracic region has four subdivisions: two lateral pleural cavities; the mediastinum; and within the mediatinum, the pericardial cavity. The abdominal region contains the abdominopelvic cavity: the abdominal (or peritoneal) cavity, which is enclosed laterally and ventrally by an abdomial wall of soft tissues (no bones), contains most of the digestive organs; the pelvic cavity, which which is the region within the pelvic girdle, contains the organs of urination and reproduction. These two portions of the abdominaopelvic cavity are essentially continuous with each other, and their functions overlap. Thoracic Cavities Using scissors, carefully make the shallowest possible cut along the midventral line of the chest about 0.5 cm off the center line, cutting the costal cartilages from the edge of the sternum, from end to end. Then, from the anterior end of this cut, carefully make shallow lateral cuts (chest wall only) dorsally and caudally to a point under the original location of the belly of the latissimus dorsi. From the posterior end of the sternal cut, make lateral cuts following the anterior edges of the last true ribs around to where the dorsal surface lies on the work surface. You may break the ribs near the spine in order to pin back the chest walls, to make study of the thoracic contents easier. B. After the chest is opened, the revealed cavities are the left and right pleural cavities— sometimes called the pleural sacs. The pleural cavities contain the soft, spongy lungs. Anteriorly, the pleural cavities narrow toward the junction where the trachea, major blood vessels, and esophagus pass to the throat. The lateral walls of the pleural cavities are the interior surface of the chest wall; and the posterior wall of the pleural cavities is formed by a dome-shaped partition of thin muscle, the diaphragm. Cat Guts p. 2 C. GENERAL PLAN OF THE PLEURA: Each pleural cavity is lined by a smooth, moist membrane, the pleura, which is defined in two parts: the parietal pleura lines the inside surface of the thoracic walls, covers the anterior face of the diaphragm, and forms the doublelayered mediastinal septum (ventrally) and the walls of the mediastinum (dorsally). The visceral pleura is that part of the pleura which lines the surface of the lung, to which it is indistinguishably fused. In the median region, under the original location of the sternum, lies the heart. You may notice (if it hasn’t been damaged too much by the opening of the chest) a membranous partition that reaches from the heart toward where the sternum was. This dense irregular connective tissue (D.I.C.) is called the mediastinal septum (“middle divider”). It actually consists of the medial portions of the left and right parietal pleura sacs in contact with each other. Heading dorsally, the two membranes separate and pass around the heart, which is further enclosed in its own membranous sac, the parietal pericardium. The “space” between the two membranes of the mediastinal septum is called the mediastinum. Dorsal to the heart, the mediastinum also contains the esophagus, the branchings of the trachea into the bronchii (which enter each lobe of lung), and the major ascending and descending blood vessels of the chest (the dorsal aorta and the pre- and postcaval veins). D. Examine the left lung. It is a soft, spongy organ divided into three lobes: a smaller anterior and larger middle and posterior lobes. Use a scalpel to make a ½”-deep cut into the left posterior lobe; note that macroscopically the organ appears solid, but is really composed of innumerable minute air sacs called alveoli. E. Note that the right lung is larger than the left lung. It too is divided into anterior, middle, and posterior lobes; but notice that the posterior lobe may also be divided into two lobules, a medial and a lateral. The medial lobule projects into a pocket formed by a special, dorsally directed fold of the mediastinal septum, called the caval fold. The caval fold has the function of supporting the large postcaval vein, which can be found in the fold’s dorsal margin, extending from the diaphragm to the heart. F. Examine the heart and pericardial sac. The pericardial sac, or parietal pericardium, is a sac of thin tissue (areolar/D.I.C.) enclosing the heart but not attached to it except at the anterior end, where the great vessels enter and leave the heart. The heart is freely movable within the pericardial sac. The narrow “space” between the heart and its pericardial sac is called the pericardial cavity, and is another portion of the coelom. Cut and fold back the pericardial sac to expose the heart. The surface of the heart is invested by a thin membrane, the visceral pericardium, indistinguishably fused to the heart wall. The visceral pericardium is continuous with the parietal pericardium at the anterior end, where the great vessels enter and leave the heart. G. Look carefully in the mediastinum, in the median line, ventral and anterior to the heart, and extending forward. There will be found a mass of glandular tissue, the thymus, which is larger in younger specimens, but may be almost absent in some older specimens. As you probe for the thymus, be sure not to injure the large blood vessels occurring in this region. Cat Guts p. 3 H. Now lift the left lung and heart and gently but firmly press them over to the right, looking into the anterio-dorsal region of the left pleural cavity. You should be able to see that each lobe of the lung is anchored to the mediastinal wall by a narrow radix, or root, consisting of a 3-tube package of artery, vein, and bronchus enclosed in a thickened bit of pleura called the pulmonary ligament. Carefully cut through the root of the left posterior lobe and remove the lobe. Now you can see the radix in cross-section. I. Note that the lungs are attached along most of their length to the dorsal thoracic wall by the pulmonary ligament (D.R.C.), a thickened fold of the pleura. Note that dorsal to the root of the lung, the pleura continues onto the dorsal and lateral surfaces of the pleural cavity; that is, the visceral pleura is continuous with the parietal pleura. Further, observe that certain other structures can be seen lying against the median dorsal wall of the chest, at the back of the mediastinum. The most conspicuous of these structures is the dorsal aorta, a very large vessel that arches away from the top of the heart to the left, then turns and descends toward the diaphragm. Ventral and adjacent to the dorsal aorta is the esophagus, which should be carefully traced to where it penetrates the diaphragm. J. The diaphragm is a curved sheet forming the posterior wall of the thoracic cavity and completely separating it from the abdominal cavity. The center of the anterior face of the diaphragm is seen to consist of connective tissue forming a circular tendon, the central tendon. The rest of the diaphragm is muscular, taking its origin from the ribs, sternum, and vertebrae, and inserting on the central tendon. Sketch a ventral view of the thoracic cavity. Be sure to include the following: Lungs Thymus Common carotid Diaphragm Submaxillary gland Left subclavian artery Heart External jugular vein Great saphenous vein Trachea Pulmonary trunk Esophagus Aorta Peritoneal and Pelvic Cavities As you work your way through the abdominal (or peritoneal) cavity, keep in mind that these are inexpensive specimens. The timing of the arterial/venous/anesthetic injections was bound to be inexact among specimens of varying ages, body masses, and metabolic rates. As a result, in tripleinjected specimens, capillary color may be all yellow or all blue or blended green. [—in doubleinjected specimens: all red or all blue or blended pink.] Just realize that if a particular tissue is dense with color, but you can’t discern individual vessels with the naked eye, this indicates a capillary bed. Of course, the abdominal digestive tract is richly vascularized in all species..... K. GENERAL PLAN OF THE PERITONEUM: The peritoneal cavity is lined by a membrane, the peritoneum. As in all coelomate animals, that portion of the membrane on the inside of the body wall is called the parietal peritoneum. In both dorsal and ventral regions, the peritoneum is deflected from the body wall and passes over the surfaces of the visceral organs, forming a covering layer for them. This layer is called the visceral peritoneum (a.k.a., serosa). In passing to and from the body wall and the viscera, the peritoneum forms doublelayered membranes, generally called the mesenteries. The mesenteries act as “tethers” which help stabilize the convoluted digestive organs by interconnecting them with each other and with the abdominal walls. The ancient ventral mesentery persists in modern Cats Guts p. 4 mammals only in the regions of the liver and urinary bladder. The dorsal mesentery, however, is still very extensive; most of its various portions have their own names, which are identified in the following sections. L. GENERAL PLAN OF THE PERITONEAL CAVITY: The anterior wall of the peritoneal cavity is formed by the concavely arched diaphragm which, when intact, completely separates the peritoneal and pleural cavities. Just posterior to the diaphragm, and shaped to fit its concave surface, is the large, lobed liver, generally grayish brown in preserved specimens. Posterior to the liver, the peritoneal cavity appears filled by the coils of the intestine. The intestine will be at least partially covered ventrally by a thin double membrane impregnated with streaks of fat, called the greater omentum. Forming part of the complicated stomachrelated peritoneum called the mesogaster, the greater omentum helps anchor the small intestine and the transverse colon to the visceral peritoneum of the stomach, and to the parietal peritoneum of the dorsal wall of the abdominal cavity. (The organization of the mesogaster and of the greater and lesser omenta are described more thoroughly below, in sections P and Q.) M. By raising the liver and looking dorsally, find the stomach, with the spleen attached to its left border by a mesentery called the gastrosplenic ligament. The spleen is the largest lymphoid organ of the mammalian body. LIVER N. The liver presents a convex anterior surface, fitting against the posterior surface of the diaphragm; and a concave posterior surface, fitting over the stomach and the most anteriorventral part of the intestine. The liver is divided into right and left lobes, each of which is further divided into median and lateral lobes. The left lateral and right median are usually distinctly larger than the other two lobes; and the left lateral is further cleft into two lobules. To understand these divisions, lift portions of the liver and study the roots of attachment. When you do, you should note there is one further, small lobe, called the caudate lobe, Cat Guts p. 6 situated inside a mesentery called the lesser omentum between the median lobes and the stomach. Nestled between the two right lobes, find the yellowish green gall bladder. STOMACH O. To examine the stomach, raise the liver and press it craniad. (The exposure of the stomach may be facilitated by slitting the diaphragm on its left side.) The stomach is an elongated, irregularly shaped, fairly muscular organ. Find where the esophagus emerges from the diaphragm and enters the anterior surface of the stomach. This junction is called the cardia, and the region of the stomach adjacent to it is called the cardiac region of the stomach; the sac-like bulge of the stomach to the left of the cardia is called the fundus; and the muscular, transverse section of the stomach is called the body. At its right end, the pylorus of the stomach narrows conically to a constriction called the pyloric sphincter, which regulates the passage of food from the stomach into the intestine. [Just beyond the pylorus, you’ll see that the intestine makes an abrupt caudal-and-leftward U-turn.] The shorter, laterally concave anterior surface of the stomach is called the lesser curvature; the larger convex posterior surface is called the greater curvature. P. RELATIONS OF THE STOMACH TO THE PERITONEUM. Raise the fundus and note the mesogaster (peritoneum related to the stomach) extending from the dorsal cavity wall to the stomach. Only a small portion of the mesogaster actually passes directly to the stomach; the greater part “descends” posteriorly to form the greater omentum, which envelopes and supports the intestine [as discussed above in section L]. Then it returns anteriorly, passing onto and around the pancreas and duodenum and finally onto the stomach wall along the greater curvature. To the left of the stomach, the spleen is enclosed in the ventral wall of this sheet; the portion of the omentum directly between spleen and stomach is called the gastrosplenic ligament. From the greater curvature, it passes over the stomach surfaces, forming the visceral peritoneum (or serosa) of the stomach. Q. At the lesser curvature of the stomach, the peritoneum becomes mesentery again, passing to the middle of the posterior face of the liver as a strong ligament called the lesser omentum (a.k.a., gastrohepatic ligament). A portion of it, called the hepatoduodenal ligament, then continues rightward from there to the first section of intestine. R. IN THE HEPATODUODENAL LIGAMENT.....run the bile ducts. To see them distinctly, carefully dissect away the ventral face of the ligament. The cystic duct can be traced from the gall bladder; and the hepatic ducts can be traced from the lobes of the liver— especially large ones from the right lateral lobe. The cystic duct and the hepatic ducts unite to form the common bile duct, which should be traced to the duodenum. Also in this ligament, to the right and dorsal to the cystic and common bile ducts, lies the large hepatic portal vein. Try not to injure this vessel, but trace it to its branch into the right lateral lobe of the liver. S. HEPATIC LIGAMENTS. As we have seen, the lesser omentum extends to the middle of the posterior face of the liver, where it becomes the serosa of the liver. Here its two walls part and follow the surface of the liver, fused with it as visceral peritoneum, around to the anterior face, where they again unite to form ligaments. The falciform ligament (now torn by opening of the ventral abdominal wall, and so probably not easily recognizable) normally extends from between the two median lobes of the liver to the median ventral line of the abdominal wall (where it becomes parietal peritoneum again); in vivo, it is a thin sheet with a Cat Guts p. 7 concave posterior border; anteriorly and dorsally, it is continuous with the coronary ligament, a stout ligament which attaches the liver to the central tendon of the diaphragm. The coronary ligament is circular in form, and its ring of attachment to the liver bounds a small area of the liver’s anterior face that is actually free of serosa. INTESTINE (formerly called the “small intestine”) T. Now trace the intestine, starting from the pylorus. As you proceed through sections U, V, W, carefully but thoroughly detach such mesentery as necessary to unravel the intestine and spread it out in the work surface. BUT! leave the colon (“large intestine”) in its original position until later. U. The first portion of the intestine, the duodenum, begins by abruptly curving caudad, and then turning left. Its caudad curve is bound to the liver by the hepatoduodenal ligament, and the transverse portion is supported by a dorsal portion of the greater omentum, the mesoduodenum, and is also attached to the right kidney by the duodenorenal ligament. V. Located in the mesoduodenum is the pancreas,which is more easily seen by gently spreading the mesentery. The pancreas is a loosely organized, usually tan or pinkish gland which extends leftward into the dorsal wall of the greater omentum posterior to the greater curvature of the stomach. There are two pancreatic ducts. The principle one joins the common bile duct at the point where the latter enters the duodenum (you may need to pick away the substance of the pancreas to see this duct); the slightly swollen common chamber where bile and pancreatic ducts unite is called the ampulla of Vater. The secondary, or accessory pancreatic duct, enters the duodenum slightly posteriorly to the ampulla, but is usually hard to isolate. W. From the duodenum trace the coils of the remainder of the intestine. These are supported by the major portions of the greater omentum (in this region, usually called simply the dorsal mesentery, or sometimes the mesentery proper). The second, longest Cat Guts p. 8 portion of the intestine, called the jejunum, begins where the duodenum turns posterior and begins markedly coiling; and the last portion, where the coils begin to relax, is called the ileum; but there is no definite boundary between the two portions. Note the coils of the mesentery that accompany the intestine, and the frequent fusions that occur between these coils. Follow the ileum to where it enlarges into the colon. (This usually occurs in the right posterior region of the abdomen—but the location can vary in individual specimens, especially in pregnant females.) The junction of the intestine with the colon (see below) is marked by a baggy projection called the caecum. [By the time evolution reached the primates, the caecum became reduced to a vermiform appendix, such as you were born with.] Again, it may be necessary to partially tear the mesenteric fusions, but keep the organ structures as intact as possible. COLON (formerly called the “large intestine”) X. The colon passes anteriorly as the ascending colon; then turns left and extends across the abdominal cavity as the transverse colon; then turns abruptly and proceeds straight posteriorly as the descending colon. The portion of dorsal mesentery supporting the colon is called the mesocolon (no surprise). At the left corner, where the transverse turns to descending, the mesocolon is secondarily fused to the mesogaster (see sections L and P above). Y. The terminal portion of the descending colon is the rectum. Both the rectum and the urinary duct (urethra) pass to the exterior through the ring formed by the pelvic girdle and the spinal column. (We will follow these to the anus and to the penis or vagina when we dissect the urogenital system of the cat.) Now cut through the exact junction of the small and large intestine and note an elevation, the ileocolic valve, projecting into the ileum. Also make short incisions at various points along the small and large intestines to see how the lining of the intestine varies from one region to another. KIDNEYS Z. On the dorsal wall of the peritoneal cavity, at about the level of the posterior ends of the liver lobes, and outside [behind] the parietal peritoneum, are the kidneys, which can be seen by gently lifting the coils of the intestine. BLADDER AA. The urinary bladder is a sac occupying the posterior end of the peritoneal cavity, immediately internal to the ventral body wall, and ventral to the colon. When intact, a mesentery called the median ligament of the bladder (median umbilical fold in human anatomy) extends from the ventral surface of the bladder to the median ventral line, and extends forward for some distance. Near the exit of the bladder from the peritoneal cavity, each side has a small ligament called the lateral ligament of the bladder. LYMPHATICS BB. The small round bodies that you may notice in the mesenteries, often buried in fat, are lymph glands, parts of the lymphatic system. Small portions of lymphatic tissue, called lymph nodules, are also abundant in the walls of the intestine. Aggregations of the Cat Guts p. 9 nodules are called Peyer’s patches. They appear as thickened oval spots on the surface of the intestine, of a slightly different color than the surrounding intestinal wall. REPRODUCTIVE STRUCTURES CC. In female specimens: The cat’s uterus is quite different from a human. The uterus in a cat is Y-shaped and is called a bipartite uterus. The base od the Y is the body of the uterus and the upper two branches are the uterine horns (where multiple fetuses may be located if your cat is pregnant). In the pelvic cavity, locate the small, oval ovaries posterior and lateral to the kidneys and the small uterine tubes that have tiny fimbriae curved over the ovaries. Note the thin mesentery that attaches these structures to the body wall. DD. In male specimens: Because a male cat has a retractable penis, you may need to check for the external urethral orifice first to find the penis and the sheath-like prepuce covering it. To observe the glans penis, make an incision in the prepuce. Identify the scrotum or scrotal sac covering the paired testes, which may not be very obvious if you have a young male. Carefully, make a lateral incision in one side of the scrotum and remove the loose fascia and inner fibrous connective tissue to expose one testis. Note the Epididymis on the medial and posterior surfaces of the testis, and inspect its tiny, coiled tubules (you may want to use a hand lends for this). Identify the ductus (vas) deferens that begins at the tail of the epididymis and travels toward the body in the spermatic cord. Observe the spermatic cord and cut away the connective tissue to identify the ductus (vas) deferens, testicular artery, testicular vein, and autonomic nerves within it. Follow the ductus (vas) deferens through the inguinal canal into the pelvic cavity. Trace the path of the ductus (vas) deferens in the abdominopelvic cavity as it arches around the ureter, and continues posterior to the bladder to join the small prostate gland at the urethra. Inside the pelvic cavity, the testicular blood vessels and autonomic nerves travel near the ureters, taking a different route from the ductus (vas) deferens. Cat Guts p. 10 Make sure to observe the dissection of a cat belonging to the opposite gender at some point during the class period. Sketch a ventral view of the abdominal cavity. Be sure to include the following: Liver Mesentery Esophagus Intestine Kidney Ureter the appropriate reproductive structures Stomach Ascending colon Urinary Bladder Spleen Transverse colon Gall Bladder Descending colon ************************************************************************ ************************************************************************ BLOOD VESSELS Double injected cats are usually used to identify blood vessels. Arteries are injected with red latex, and veins are injected with blue latex. Blood vessels differ slightly in location from cat to cat. It is important to understand that these slight differences in location are normal and also occur in humans. Observe the fascia that protects and secures blood vessels. Carefully remove the fascia with blunt instruments to separate blood vessels from other structures. ARTERIES A. If you have not done so already, cut open the pericardial sac surrounding the heart with scissors. Expose the heart and identify the pulmonary trunk exiting from the right ventricle. Locate its branches, the right pulmonary artery and the left pulmonary artery, and follow them to the lungs. Cat Guts p. 11 B. Identify the ascending aorta as it exits the left ventricle. Identify the aortic arch. In cats, there are only two branches off the aortic arch, the brachiocephalic artery (first branch) and the left subclavian artery. Identify these branches. C. The brachiocephalic artery divides into the right subclavian artery, the common carotid, and the left common carotid. Locate the right subclavian artery as it turns laterally and travels toward the upper extremity. Locate the right and left common carotid arteries as the travel along the trachea. At the level of the larynx, the common carotid arteries divide to form the external and internal carotid arteries. D. The first major branch off each subclavian artery is the vertebral artery. Follow the right and left subclavian arteries to the first rib. As each subclavian crosses the first rib, it becomes the axillary artery. Follow the axillary artery into the arm, where it becomes the brachial artery. Distal to the elbow, the brachial artery divides to form the radial and ulnar arteries. E. Lift up the heart and follow the aortic arch as it descends and forms the thoracic aorta. Follow the thoracic aorta and observe where it passes through the diaphragm with the esophagus and inferior vena cava, and becomes the abdominal aorta. The abdominal aorta is retroperitoneal. You must move aside the visceral organs and remove the parietal peritoneum lining the dorsal body wall to observe the aorta. F. Locate the celiac trunk, the first branch off the abdominal aorta. The celiac trunk branches into the hepatic artery, the left gastric artery, and the splenic artery. Posterior to the celiac trunk is the superior mesenteric artery, whose branches can be observed traveling through the mesentery of the small intestine. Follow the abdominal aorta to the level of the kidneys and observe the paired renal arteries branching off and traveling to the kidneys. G. The gonadal arteries, testicular arteries in males and ovarian arteries in females, are the next major branches off the abdominal aorta. Follow these arteries to the gonads (testes in males and ovaries in females). H. The inferior mesenteric artery branches off the abdominal aorter posterior to the gonadal arteries. Branches of the inferior mesenteric artery travel through the mesentery of the large intestine. Iliolumbar arteries are large branches off the abdominal aorta posterior to the inferior mesenteric arteries. I. The abdominal aorta ends when it divides into right and left external iliac arteries, and the internal iliac artery. There is no common iliac artery in the cat. Follow one external iliac artery into a thigh, where it becomes, the femoral artery. The femoral artery travels down the thigh and becomes the popliteal artery in the popliteal area. VEINS Blood leaving tissues travels through veins back to the heart. Remember that some veins are superficial (close to the surface), whereas others are deep. Many of the deep veins are adjacent to arteries with the same name Cat Guts p. 12 J. Observe the large superficial vein traveling along the medial surface of the leg ascending into the thigh. This is the great saphenous vein, and it joins the femoral vein, a deep vein, traveling through the thigh adjacent to the femoral artery. The femoral vein becomes the external iliac vein in the groin region. The internal iliac vein joins the external iliac vein to form the common iliac vein. The right and left common iliac veins unite to form the inferior vena cava (postcava in cat). K. The hepatic portal vein probably does not contain blue latex and may appear brown from the presence of coagulated blood. The hepatic portal vein receives blood from the digestive organs and carries this blood to the liver. The hepatic portal vein is formed from the gastrosplenic vein and the superior mesenteric vein. Follow the inferior vena cava through the diaphragm, into the thoracic cavity, and into the right atrium. L. Locate the radial and ulnar veins in the forearm. These veins are adjacent to their corresponding arteries. The radial and ulnar veins merge to form the brachial vein. The brachial vein becomes the axillary vein that is adjacent to the axillary artery in the axillary regions. M. In the shoulder area, the axillary vein becomes the subclavian vein. Each subclavian vein unites to form either the right or left brachiocephalic vein. The brachiocephalic veins merge to form the superior vena cava (precava). Follow the superior vena cava until it enters the right atrium. N. Blood draining from the face and skull enters the external jugular vein. The internal jugular vein drains the brain. Identify the large external jugular vein traveling along the lateral surface of the neck until it joins with the subclavian vein to form the brachiocephalic vein.