Self Study Guide For Procedural Sedation Credentialing
advertisement

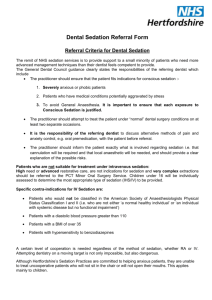
Sonoma Valley Hospital – Medical Staff Self-Study Guide for Procedural Sedation Credentialing PURPOSE AND GOALS In procedural sedation, the goals are to: 1) maintain safety throughout the intervention 2) minimize pain and/or anxiety, and 3) facilitate the procedure or the investigation. The patient must be able to respond rationally to commands and to maintain his/her own airway. The ability to maintain a patent airway is not only dependent on the amount of sedation given, but is also impacted by the patient’s underlying medical problems, debilitation, and body habitus. Every physician must thoroughly evaluate these critical factors prior to a sedation procedure. Deep sedation is not to be provided under any circumstance by a physician who is only credentialed to deliver procedural sedation. These guidelines are not intended to manage patients with other known medical conditions (such as pain management patients, patient with seizure disorders, patients in labor and/or patients being managed by an anesthesiologist. When procedural sedation is used, it is crucial to understand and appreciate the different levels of sedation and general anesthesia: DEFINITIONS Light Sedation/Anxiolytic: Route of medication can be oral, intramuscular (IM) or intravenous (IV). These patients are basically awake. There is essentially no anesthesia. Amnesia may or may not be present. All bodily functions are normal and their protective reflexes are intact. Procedural Sedation (previous terminology, Conscious Sedation): A minimal level of depressed consciousness that retains the patient’s ability to maintain a patent airway independently. The patient would be able to respond spontaneously to physical and verbal stimuli. The drug and the dosage are not intended to produce loss of consciousness. An ideal level of sedation is when one achieves the clinical presentation of the patient’s slurring of speech. Deep Sedation: A controlled state of depressed consciousness or unconsciousness from which the patient is not easily aroused and is unable to respond purposefully to physical stimuli or verbal commands. This may be accompanied by partial or complete loss of protective airway reflexes and the patient’s inability to maintain a patent airway independently. General Anesthesia: A controlled state of unconsciousness accompanied by a loss of protective reflexes, including loss of the ability to maintain a patent airway independently or to respond purposefully to physical stimulation or verbal command. Page 1 of 13 Sonoma Valley Hospital – Medical Staff Self-Study Guide for Procedural Sedation Credentialing GUIDELINES 1. Patient Education and Participation Staff will educate patients about treatment or diagnostic procedures, including moderate sedation expectations so they can participate in their care plans to determine appropriate use of sedation and analgesia and promote best patient outcomes. 2. Personnel: A. The practitioner supervising the administration of drugs for procedural sedation shall be appropriately trained in the following: 1) Airway management including: positioning of the airway, use of a oral pharyngeal airway, application of positive pressure ventilation with a bag and mask 2) Safe use of drugs with recognition of their effects with patient variability 3) Basic arrhythmia recognition course B. The practitioner (nurse) will complete competencies as defined and monitored by each department. C. The practitioner (nurse) monitoring the patient shall have no other assigned duties while the patient is under procedural sedation. 2. Quality Monitoring: A. The Department of Anesthesiology will monitor and evaluate procedural sedation practices throughout the hospital to promote uniform standard of care. The Anesthesia Department will review, on and on-going basis, cases that are identified by the Procedural Sedation Indicators. B. Procedural Sedation Indicators are defined as the following: 1) Cardiopulmonary arrest 2) Unanticipated admission to the hospital or the ICU 3) Use of Narcan or Romazicon 4) Oxygen saturation less that 90% despite supplemental oxygen 5) Respiratory rate less than 8 per minutes for duration of greater than five minutes 6) Any patient requiring any assisted ventilation. 3. Comprehensive Patient Assessment: Each patient should be assessed prior to a procedure. Assessment should include: 1) History and a physical 2) Medications 3) Allergies 4) Adverse reaction with prior anesthesia 5) Vital signs 6) NPO status 7) Proper consent signed 8) ASA classification (See ASA Classification Table.) Page 2 of 13 Sonoma Valley Hospital – Medical Staff Self-Study Guide for Procedural Sedation Credentialing American Society of Anesthesiology Patient Classification Table Class Description ASA I Healthy patient without problems ASA II Mild systemic disease or conditions that need to be treated Examples: Diabetes Mellitus, smoking, asthma, thyroid disease. ASA III Severe systemic diseases that limit activity but are not incapacitating Examples: Complicated or uncontrolled Diabetes Mellitus, uncontrolled hypertension, coronary artery disease (CAD), chronic obstructive pulmonary disease (COPD), cardiovascular vascular accident (CVA). ASA IV Severe systemic disease that is incapacitating and is a constant threat to life Examples: Severe CAD, congestive heart failure (CHF), end stage renal disease (ESRD), and steroid-dependent COPD. ASA V A moribund patient not expected to survive 24 hours with or without intervention. “E” Added category if any of the above categories are an emergency 4. Airway assessment A. Each patient must be assessed for potential airway complications prior to any procedural sedation. B. A Mallampati airway classification assessment must be documented. The Mallampati classification relates tongue size to pharyngeal size. The test is performed with the patient in the sitting position, the head held in a neutral position, the mouth wide open, and the tongue protruding to the maximum. The subsequent classification is assigned based upon the pharyngeal structures that are visible. 1) Look at the size of the tongue relative to the size of the oral cavity. If the tongue obscures much of the pharynx, the patient is more likely to obstruct under sedation. 2) Sit the patient upright and ask him or her to open their mouth as widely as possible and protrude their tongue. A good Mallampati airway assessment can be obtained without patients saying, AAAAAHH! A difficult airway may be recognized on a very gross and obvious level. However the potential difficult airway may be very subtle and requires careful examination. The basis of a difficult airway are numerous and are only briefly discussed here. Extreme caution (especially in selection of sedation level) is Page 3 of 13 Sonoma Valley Hospital – Medical Staff Self-Study Guide for Procedural Sedation Credentialing required for the patient that presents with any of these conditions, especially if the patient is in the lateral or prone position. Mallampati Classification Class I Class II Class III Class IV Visualization of the soft palate, fauces, uvula, anterior and posterior pillars Visualization of the soft palate, fauces, and uvula Visualization of the soft palate, and the base of the uvula Soft palate is not visible at all. The classification assigned by the clinician may vary if the patient is in the supine (instead of sitting) position. If the patients phonates, this will falsely improve the view. If the patient arches his or her tongue, the uvula will be falsely obscured. A Class I view suggests ease of intubation (correlates laryngoscopic view, grade I) with a 99-100% occurrence rate. Class IV view (correlates a poor laryngoscopic view, grade III or IV) with a 100% occurrence rate. Beware of the intermediate Classes which may result in all degrees of difficulty in laryngoscopic visualization. 5. Clinical Considerations and Interventions If a patient has a small mouth, receding chin, and a short or immobile neck, management of the airway could be difficult. These patients should be kept extremely light. It is essential to constantly monitor these patients who have been given sedation. Be alert for problems with ventilation and be cognizant of the fact that restlessness can be sign of excessive sedation, as well as inadequate sedation. If the patient is breathing but the oxygen saturation falls, it may only be necessary to stimulate the patient and instruct him/her to take a deep breath. Hold sedation until saturation rises. Varying degrees of stimulation during the procedure will result in comparable patient response. During the periods of relative low level of stimulation, the patient can become more somnolent. If the patient has some discomfort, it will be important to distinguish between pain and Page 4 of 13 Sonoma Valley Hospital – Medical Staff Self-Study Guide for Procedural Sedation Credentialing pressure. The administered intravenous anesthetic provides some pain relief, but it cannot be totally relied upon for complete analgesia. Pain should be controlled by local anesthetic administered by the surgeon. Narcotic analgesics can cause some degree of respiratory depression and must be given judiciously. If the patient's airway becomes obstructed during sedation, the chin should be lifted until the tongue is lifts up from the pharynx allowing air to pass at the base of the tongue. If the patient does not breathe with the now open airway, an Ambu bag must be used to provide positive pressure ventilation until spontaneous ventilation returns. It is very important to maintain an open airway with chin lift/jaw thrust and maintaining a tight fit with the mask for ventilation. Complications of procedural sedation can occur as with general anesthesia (including cardiac arrest, pulmonary arrest, drop in blood pressure, aspiration, arrhythmia, allergic reaction or shock). In the event, that the patient stops breathing and does not respond to stimulus (such as: turning the patient supine, surgical stimuli, jaw thrust or chin lift), a Code Blue must be called. PROCEDURAL REQUIREMENTS 1. Practitioner/Nurse (with no other assigned duties) will continuously monitor and assess the patient under procedural sedations and will record (every 15 minutes or more frequently if needed) the following and communicate any abnormal conditions immediately: A. Blood pressure B. Heart rate C. Pulse oximetry D. Respiratory rate E. EKG F. Level of consciousness (Note: A patient starting to slur speech is an indication of ideal level of procedural sedation.) G. Temperature (for procedures lasting more than one hour). 2. Physician must be present or “immediately” available for any procedural sedation that involves the administration of a controlled substance. 3. All medication being used must be properly labeled, handled, stored, and documented when administered. 4. In accordance with the hospital policy, all patients having procedural sedation must have intravenous access. (The only exception would be in the pediatric or ER population.) 5. Medication must be administered according to State statutes (given by a physician or a registered nurse). 6. Supplemental oxygen is required for patients with saturation levels less than 90% on room air. Supplemental oxygen prior to sedation will provide extra time for the health care provider to respond in the event that a patient experience apnea or signs of impending respiratory arrest. Page 5 of 13 Sonoma Valley Hospital – Medical Staff Self-Study Guide for Procedural Sedation Credentialing 7. The practitioner (nurse) will provide and document a post procedural clinical assessment based on the Aldrette Scoring System. ASSESSED FUNCTION Activity Respiration Circulation Consciousness Color ALDRETTE SCORING SYSTEM DESCRIPTION Voluntary movements of all limbs to command Voluntary movements of 2 extremities to command Unable to move Breathe deeply and cough Dyspnea, hypoventilation Apneic BP 20% of preanesthesia level BP 20-50% of preanesthesia level BP 50% of preanesthesia level Fully awake or pre-procedure level Arousable Unresponsive Pink Pale, blotch, jaundice Cyanotic SCORE 2 1 0 2 1 0 2 1 0 2 1 0 2 1 0 ROOM SET-UP, EQUIPMENT, AND SUPPLIES REQUIREMENTS The following is the required list of equipment and supplies that should be immediately available in the procedural sedation room: 1. 2. 3. 4. 5. 6. 7. 8. 9. Ambu bags and airway supplies Oxygen Suction equipment with Yankauer tip Monitoring equipment Pulse oximetry EKG Blood pressure monitor Crash cart unit Reversal agents POST ANESTHESIA CARE UNIT (RECOVERY) REQUIREMENTS: 1. Monitor, assess, and document the following: A. Level of consciousness (including response to verbal interaction, commands) B. Level of comfort C. Level of knowledge, understanding D. Nature of a procedure and any complications Page 6 of 13 Sonoma Valley Hospital – Medical Staff Self-Study Guide for Procedural Sedation Credentialing 2. Intervene appropriately based on results of continuous monitoring and assessment (i.e. repositioning, administering of meds, education, comfort, physician communication, etc.) 3. Explain procedure and educate patient as to expectations in the recovery and post recovery phase. 4. Be vigilant to the signs, symptoms of complications of procedural sedation (that are the same as general sedation)—including cardiac arrest, pulmonary arrest, hypotension, aspiration, arrhythmia, allergic reaction, and shock. 5. Provide a comprehensive, meaningful report (SBAR—situation, background, assessment, and recommendation—communication ) to the caregiver assigned to follow the patient’s care. Page 7 of 13 Sonoma Valley Hospital – Medical Staff Self-Study Guide for Procedural Sedation Credentialing DRUGS USAGE GUIDELINES: Sedation Drugs and Reversal Agents Romazicon Narcan Diluadid Drugs Morphine Versed Fentanyl Ketamine Etomidate 0 50 100 150 200 250 300 350 Minutes Duration of Clinical Effect Page 8 of 13 Sonoma Valley Hospital – Medical Staff Self-Study Guide for Procedural Sedation Credentialing 1 **These guidelines are derived from published resources. Doses in excess of these guidelines are at the discretion of the physician.** ADULT SEDATION DRUG DOSAGE GUIDELINES Approved Medications Fentanyl (Sublimaze) Hydromorphone (Dilaudid) Midazolam (Versed) Morphine Sulfate Etomidate (Amidate) **ANESTHESIA AND ED ONLY** Ketamine (Ketalar) **ANESTHESIA AND ED ONLY** Naloxone HCL (Narcan) Flumazenil (Romazicon) 2 A. Drug Administration Guidelines Fentanyl (Sublimaze) Route: IV, IM Initial Dose: Administer 0.5 – 1.0 micrograms/kilogram (Give slow IV over 3-5 minutes; inject into infusing line.) Recommended Total Dose: 50-250 micrograms Onset: 1-1.5 minutes Peak: 5-15 minutes Duration: 30-60 minutes Half-life: 2-4 hours Potential Adverse Reactions: Respiratory depression, apnea, rigidity, bradycardia, hypotension, hypertension, dizziness, blurred vision, nausea, emesis, laryngospasm, diaphoresis, hypersensitivity, sedation, drowsiness, convulsions, respiratory depression, peripheral circulatory collapse, cardiac arrest, allergic reactions, suppression of cough reflex. B. Hydromorphone (Dilaudid) Route: IV Initial Dose: 1-2 mg slow IV push Recommended Total Dose: 4 mg (DO NOT EXCEED 0.1 mg/kg) Onset: 15-30 minutes Peak: 0.5–1 hour Duration: 4-5 hours Half-life: 2-3 hours Potential Adverse Reactions: Drowsiness, thrombosis, and phlebitis at the site of injections, slurred speech, nausea, bradycardia, hypotension, respiratory depression, skin rash, blurred vision, nystagmus, fluctuations in vital signs, apnea, hiccoughs, vomiting, coughing, over sedation, and headache, increased CSF pressure. Page 9 of 13 Sonoma Valley Hospital – Medical Staff Self-Study Guide for Procedural Sedation Credentialing C. **These guidelines are derived from published resources. Doses in excess of these guidelines are at the discretion of the physician.** ADULT SEDATION DRUG DOSAGE GUIDELINES Midazolam (Versed) Route: Initial Dose: IV 0.5 mg – 2 mg slow IV over at least 2 min.; slowly titrate every 2-3 minutes; Recommended Total Dose: 2.5-5 mg (decrease dose in elderly) IV: Onset: 1 minute-5 minutes (IV) Peak: 2-4 minutes (IV) Duration: 1-4 hours; increased in cirrhosis, CHF, obesity, elderly and acute renal failure) IM: Onset: Within 15 minutes Peak: 0.5-1 hour Duration: 2 hours mean, up to 6 hours Potential Adverse Reactions: Drowsiness, thrombosis, and phlebitis at the site of injection, slurred speech, nausea, bradycardia, hypotension, respiratory depression, skin rash, blurred vision, nystagmus, fluctuations in vital signs, apnea, hiccough, nausea, vomiting, coughing, over sedation and headache. May potentiate the action of other CNS depressants including opiate agonists or other analgesics, barbiturates, other sedatives or anesthetics. D. Morphine Sulfate Route: Initial IV Dose: IV Administer 2-5 mg over at least 5 minutes into an infusing IV line. Recommended Total Dose: 15 mg (Do not exceed .15 mg/kg) Onset: 1-7 minutes Peak: 20 minutes Duration: 4-5 hours Half-life: 2-4 hours Potential Adverse Reactions: Respiratory depression, hypotension, bradycardia, CNS depression, nausea and vomiting, urinary retention. E. Etomidate (Amidate) – General Anesthetic (**NOT RECOMMENDED FOR CHILDREN UNDER 10 YEARS**) Route: IV Initial Dose: 0.2 – 0.6 mg/kg over 30-60 seconds Recommended Total Dose: Onset : 1 minute Peak: 2-3 minutes Duration: 3-5 minutes Half-life: 75 minutes Potential Adverse Reactions: nausea, vomiting, respiratory depression (15% of patients), muscle twitching, adrenal suppression, hypotension Page 10 of 13 Sonoma Valley Hospital – Medical Staff Self-Study Guide for Procedural Sedation Credentialing F. **These guidelines are derived from published resources. Doses in excess of these guidelines are at the discretion of the physician.** ADULT SEDATION DRUG DOSAGE GUIDELINES Ketamine (Ketalar) – Anesthetic Adjunct Route: IM / IV (**ADMINISTER OVER MINIMUM OF 60 SECONDS**) Initial Dose: ADULT PEDIATRIC IV : 1 - 4.5 mg/kg 0.2 – 1 mg/kg IM: 0.5 - 4 mg/kg 2 – 10 mg/kg Onset: IV: 1 minute; IM: 5 minutes Peak: 4-5 minutes Half life: 10-15 minutes Duration: IV: 10-20 minutes IM: 15-45 minutes Potential Adverse Reactions: Contraindicated in patients with increased intracranial pressure, Coronary Artery disease, increased blood pressure, convulsion, delirium, hallucinations, amnesia, flashbacks possible for several weeks after use, agitation, transient laryngospasm, ptyalism, respiratory depression, oxygen desaturation < 85% in < 1% of patients. G. Naloxone HCL (Narcan) Route: Initial Dose: IV Administer 0.1-2 mg every 2-3 minute intervals; Inject into infusing line; may repeat every 20-60 minutes. Onset: Within 2 minutes Half-life: 1-1.5 hours Duration: 20-60 minutes Recommended Total Dose: 10 mg Potential Adverse Reactions: Excitement, hypotension, hypertension, ventricular tachycardia and fibrillation, pulmonary edema, seizures, nausea, vomiting, sweating, circulatory stress. H. Flumazenil (Romazicon) Route: Initial Dose: IV Administer 0.2 mg; administer over 15 seconds; inject into infusing line; wait additional 45 seconds before repeating, if necessary. Recommended Total Dose: 1 mg.; administer additional dosages at 0.2 mg (four additional times) at 1 minute intervals. Onset: 1-3 minutes Peak: 6-10 minutes Half-life: 41-79 minutes Potential Adverse Reactions: Nausea and vomiting, dizziness, injection site pain, agitation, headache, sweating, flushing, hot flashes paresthesia, emotional liability, inflammation at injection site, abnormal vision, fatigue, convulsions for patients on benzodiazepines for seizure control. **Duration: Resedation can occur usually within 1 hour; duration is usually related to dose given.** Page 11 of 13 Sonoma Valley Hospital – Medical Staff Self-Study Guide for Procedural Sedation Credentialing **These guidelines are derived from published resources. Doses in excess of these guidelines are at the discretion of the physician.** PEDIATRIC DRUG DOSAGE GUIDELINES Drug Administration guidelines: For pediatrics > 2 years. (Neonates and Adolescents excluded) MEDICATION Sedatives ƒ Midazolam (Versed) ROUTE DOSE mg/kg ONSET DURATION* COMMENTS 1-2 hours •IV maximum concentration— 1 mg/ml •Decrease dose by 30% if narcotics and other CNS depressants are administered concomitantly •Rapid onset; amnesic; Allow 3-5 min between doses to decrease the chance of oversedation. •Maximum IM/IV dose—10 mg 20-30 min 1-2 hrs 0.3 mg/kg 20-30 min 1-2 hrs 0.2-0.3 mg/kg 5 min 30-60 min •Concomitant use of barbiturates, alcohol or other CNS depressants may increase the risk of hypoventilation, airway obstruction, desaturation, or apnea and may contribute to profound and/or prolonged drug effect. •Contraindicated in patients with a known hypersensitivity to the drug or allergies to cherries or formulation excipients. •Rectal route: Dilute in 5 ml NS; administer rectally •Nasal route: Use a 1 ml needleless syringe into the nare over 15 sec; use 5 mg/ml concentration; ½ dose may be given into each nare Deep IM 0.08 mg/kg0.1 mg/km IM: 15 min. IV 0.08-0.15 mg/kg given over 10-20 min. IV: 1-5 min. PO (Syrup) 0.4-0.5 mg/kg with a maximum oral dose of 15 mg PR IN (Nasal Spray) Page 12 of 13 Sonoma Valley Hospital – Medical Staff Self-Study Guide for Procedural Sedation Credentialing **These guidelines are derived from published resources. Doses in excess of these guidelines are at the discretion of the physician.** PEDIATRIC DRUG DOSAGE GUIDELINES Drug Administration guidelines: For pediatrics > 2 years. (Neonates and Adolescents excluded) MEDICATION Ketamine (Ketalar) Analgesics Fentanyl (Sublimaze) Morphine Sulfate ROUTE IV DOSE mg/kg 1-2 mg/kg ONSET 1 min DURATION* 10-20 min COMMENTS Requires IV be in place before use in other then emergent situations in the Emergency Department. Must have 1:1 nurse to patient ratio. IM 2-4 mg/kg 5 min 15-45 min Requires IV be in place before use in other then emergent situations in the Emergency Department. Must have 1:1 nurse to patient ratio IV, IM 1-3 mcg/kg May repeat at 3060 minute intervals IV: immediate IV: 30-60 min IM: 7-15 min IM: 1-2 hrs. •Titrate in 1 mcg/kg doses •Inject slowly 3-5 min Rapid IV infusion may result in skeletal muscle and chest wall rigidity leading to impaired ventilation and apnea 0.05-0.2 mg/kg 5-15- min IM: 3-5 hours IV: 2-5 hours IV, IM •Administer IV for at least 5 min •Watch out for hypotension, bradycardia, peripheral vasodilation, histamine release Hypnotics No reversal agent available = IV ƒ 0 LEGEND FOR PEDIATRIC MEDICATIONS: Duration will vary according to dosages Intramuscular PR IM Intravenous Intranasal SL IN reversible with Romazicon Per mouth/orally PO Rectally Sublingual reversible with Naloxone Page 13 of 13