Physician Referral Form
advertisement

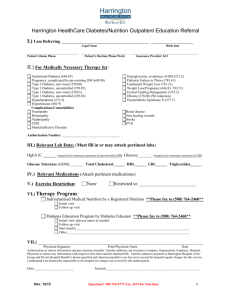
Physician Referral Form Diabetes Self-Management Education (DSME)/ MNT Medical Nutrition Therapy Fax: 216-591-0320 www.diabetespartnerhip.org/education By signing this form, I agree that the patient named below needs the following: 1. Group DSME classes offered at the Diabetes Partnership of Cleveland. 2. An individual assessment or re-education, classroom instruction and follow-up after completion of the classes, which will not exceed 10 hours. 3. Individual Medical Nutrition Therapy sessions - up to 3 hours (diabetes and other nutrition issues) Patient Name ____________________________________ DOB ________________________ Referral date _____________________ Patient Phone Number____________________ ICD - 10 Code for diabetes: diagnosis/Code __________________/E___________ ICD- 10 Code for nutrition related issue: diagnosis/code ________________/_______ (See reverse side for list) Lab tests Result Date A1C ________ ________ Fasting Glucose Result Date ________ ________ Please attached patient current electronic list of medication or their diabetes care plan. Complications for this patient: _________________________________________________________ Reason for client referral (more than 1 can apply): Recurrent elevation of blood glucose Recurrent hypoglycemia Recent hospitalization for DKA or HHNS Recurrent use of diabetes services (ER, hospital or physician/clinic visits) Other_____________________ Diabetes Education Re-education Change in mediation or treatment plan Medical Nutrition Therapy Barriers to patient’s ability to learn or perform self-management skills: Visual/hearing impairment Impaired mental status Impaired psychosocial status Eating disorder Impaired mobility Learning disability Impaired dexterity Exercise Restriction Physician signature _______________________________________ Date ______________________ Physician name (print) ______________________________ Physician NPI __________ PLEASE RETURN BY FAX TO: 216-591-0320 (fax) www.diabetespartnerhip.org/education DIABETES DIAGNOSIS AND ICD-10 CODE E08 Diabetes mellitus due to underlying condition E09 Drug or chemical induced diabetes mellitus E10 Type 1 diabetes mellitus E11 Type 2 diabetes mellitus E13 Other specified diabetes mellitus E88.81 Metabolic syndrome (cluster of metabolic risks for CVD and type 2 DM) O24.911 (Unspecified diabetes mellitus in pregnancy, 1st trimester (O24.912 2nd trimester, O24.913 3rd trimester) R73.09 Other Abnormal glucose Z86.32 Gestational Diabetes NUTRITIONAL DIAGNOSIS AND ICD-10 CODE E28.2 Polycystic Ovaries E78.2 Hyperlipidemia, mixed E73 Lactose intolerance D50 Iron deficiency anemia D51 Vitamin B12 deficiency D52 Folate deficiency D53 Other nutritional anemias F50.00 Anorexia nervosa, unspecified F50.02 Anorexia nervosa binge eating/purging type K21.9 GERD K50.10 Crohn’s Disease K51.0 Ulcerative Colitis K58.9 IBS K86.1 Chronic Pancreatitis K90.0 Celiac Disease K80 Cholelithiasis K81 Cholecystitis K82 Other diseases of gallbladder K85 Acute pancreatitis K86 Other diseases of pancreas K87 Disorders of gallbladder, biliary tract and pancreas in diseases classified elsewhere K90 Intestinal malabsorption K91 Intraoperative and postprocedural complications and disorders of digestive system, not elsewhere classified K92 Other diseases of digestive system K94 Complications of artificial openings of the digestive system K95 Complications of bariatric procedures I50 Heart failure I70 Atherosclerosis I42 Cardiomyopathy I43 Cardiomyopathy in diseases classified elsewhere I10 Essential (primary) hypertension I11 Hypertensive heart disease I12 Hypertensive chronic kidney disease I13 Hypertensive heart and chronic kidney disease I15 Secondary hypertension N18.3 CKD, stage III (moderate) N18.4 CKD, stage IV (severe) N18.5 CKD, stage V N18.9 CKD, unspecified. R63.4 Abnormal Weight Loss R63.5 Abnormal weight gain B20 Human immunodeficiency virus (HIV) disease