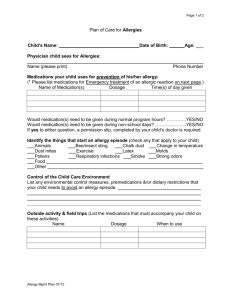
ED Outreach Services Flow Chart, and Medical Directive Form
advertisement

ED Outreach Services MEDICAL DIRECTIVES Hôpital régional de Sudbury Regional Hospital ISSUED BY: AUTHORIZED BY: ISSUE DATE: CATEGORY: ED Patient Care Team Emergency & Medical Program Council SUBJECT: Medications REVISION DATE: PAGE: 1 of 17 Medical Directives ED Outreach Services Medical Directive - Medications Directive EDOS03 Number: Title: Medications Directive Activation Date: Sponsoring/Contact Person(s) (name, position, contact particulars): Orders: Review due by: Dr. Chris Bourdon, Interim Chief of Staff Dr. Andrew Caruso, Interim Emergency Department Medical Director Dr. Andre Roch, Physician Lead, Extendicare and TCU Mary Beth Gibbons, RN, Clinical Lead – ED Outreach Appendix Attached: Yes Title: Medication Order Table Orders as identified on the appended order table: 1. Medication Order Table Acetaminophen Amoxicillin Amoxicillin/Clavulanate Azithromycin Benadryl Cefprozil Ceftriaxone Cefuroxime-AX Cephalexin Ciprofloxacin Clarithromycin Clindamycin Cloxacillin EMLA Epi 1:1000 Ipratropium Lidocaine Jelly 2% Macrobid No CATEGORY: Medical Directives SUBJECT: Medications Page 2 of 17 Moxifloxacin Pancrelipase Prednisone Ranitidine Salbutamol Sodium Bicarbonate Solu-Medrol Trimethropin/Sulfamethoxazole Recipient Patients: Appendix Attached: Yes Title: Medication Order Table No Any patient presenting to the ED Outreach Services (within the HRSRH or Long Term Care facilities with who the HRSRH has a Memorandum of Understanding) who meets the conditions identified in this directive. Authorized Implementers: Appendix Attached: Yes Title: Medication Order Table No All ED Outreach Nurses and designated staff who have successfully completed the relevant ED Outreach Services Medical Directive orientation program as described in Review & Quality Monitoring Guidelines. Medical directive certification is to be completed every 2 years. The ED Outreach Nurse - Team Lead will maintain a list of authorized implementers as part of the Medical Directive record. All physicians involved in the ED Outreach Services will review the medical directives yearly and upon any new directives added to the program. The ED Outreach Nurse - Team Lead and/or ED Medical Director will make available to all new physicians to the ED Outreach Services a medical directive package which will be signed prior to program involvement. CATEGORY: Medical Directives SUBJECT: Medications Indications: Page 3 of Appendix Attached: Yes Title: Medication Order Table 17 No Medications will be administered from the period beginning from when a patient is assessed by the ED Outreach Nurse to first contact with the attending LTC physician, unless the attending LTC physician specifically orders implementation of the directive beyond that period. Prior to implementation of any directive, a patient assessment is completed in accordance with standards of practice and any applicable HRSRH policy. Allergies and sensitivities must be documented. Specific indications are identified in the appended Order Table. Definitions for indications used in the table: 1. Acute Delirum and/or Confusion 2. Anaphylaxis 3. Cellulitis 4. Dehydration 5. Falls 6. Fever – Temperature greater than/equal to 38°C 7. Foley Catheter Difficulties 8. G-tube/Enteral Difficulties 9. Lacerations 10. Lower Respiratory Tract Infections 11. Upper Respiratory Tract Infections 12. Syncope 13. Urinary Tract Infections 14. Weakness/Dizziness Contraindications: See appended Order Table. Consent: Appendix Attached: Yes No Title: Medication Order Table Staff implementing the directive will obtain consent in accordance with the Health Care Consent Act and any relevant HRSRH policies and procedures. Guidelines for Implementing the Order / Procedure: See appended Order Table. Appendix Attached: Yes Title: Medication Order Table No CATEGORY: Medical Directives SUBJECT: Medications Documentation and Communication: Page 4 of Appendix Attached: Yes Title: Medication Order Table 17 No Implementing staff will document the: Medication order (including name of medication, dose, route, time of administration) in the order section of the patient record, noting the medical directive name and number, signing off the order as per the attending LTC physician (when attending LTC physician known) Indications, administration, and patient response in accordance with any HRSRH record-keeping policies ED Outreach Services Flow Chart, and Medical Directive Form (EDOS03) Note: Clear and timely notification, communication and documentation between the nurse and the physician are critical to safe, proper use of a medical directive. Review and Quality Monitoring Guidelines: Appendix Attached: Yes No Title: Medication Order Table Staff identifying any untoward or unintended outcomes arising from implementation of orders under this directive, or any issues identified with it will report these to LTC Physician as soon as possible for appropriate disposition. This does not include untoward or unintended outcomes or issues that are possible clinical sequelae regardless of whether a directive or direct order is used. Certification process LTC MD - yearly ED MD renewal – yearly ED Outreach Nurse recertification – every 2 years which will consist of a written test and/or successful completion of certification exam and/or maintenance of competence Administrative Approvals: ED Patient Care Team Emergency/Medical Program Council Professional Practice Council Professional Advisory Committee Medical Advisory Committee Appendix Attached: Yes Title: Medication Order Table No Appendix Attached in section under Laboratory Test and Diagnostic Procedures to cover Medical Directives: EDOS01, EDOS02, EDOS03, EDOS04 CATEGORY: Medical Directives SUBJECT: Medications Page 5 of 17 Approving Physician(s)/Authorizer(s): Appendix Attached: Yes No Title: Medication Order Table Appendix Attached in section under Laboratory Test and Diagnostic Procedures to cover Medical Directives: EDOS01, EDOS02, EDOS03, EDOS04 References Appendix Attached: Yes Title: Medication Order Table No List any references here as below and attach appendix or list references in Performance Readiness Assessment form. Public Health Agency of Canada: Canadian Immunization Guide, 6^th Ed. 2002. Talan, DA Tetanus immunity and physician compliance with tetanus prophylaxis practices among emergency department patients presenting with wounds. Ann Emerg Med. 2004 Mar;43(3):315-7. Ernst A. et al. LAT vs TAC for Topical Anasthesia in Face and Scalp Lacerations. /American Journal of Emergency Medicine. /1995;13(2):151-154. Newberry, L. (Ed.). (1998). /Sheehy’s Emergency Nursing. Principles and Practice/. 4^th Ed. .Mosby: Toronto. Guidelines 2006 for cardiopulmonary and Emergency Cardiovascular care: American Heart Association Tintinelli,j.E Kelen,GD and Stapczynski, J.S Emergency medicine: A Comprehensive Study Guide, 6th Edition 2004. Compendium of Pharmaceuticals and Specialties (CPS) 2007 Lacy,C: Armstrong,L;Lance, L Drug Information Handbook 2004 Sheehy's Emergency Nursing 5th Edition 2003 Chapter 14 Pain management Jovey, Roman Managing Pain: The Canadian Healthcare Professional Reference: The Canadian Pain Society 2002 CATEGORY: Medical Directives SUBJECT: Medications Page 6 of 17 APPENDIX: Medication Order Table Title ED Outreach Services - Medication Administration Number of Directive: EDOS03 Medication Order Table ED Outreach Services - Medication Directive (EDOS03) Orders Acetaminophen (Tylenol) Indications Fever (temperature greater than/equal to 38°C) 325-975 mg PO q 4-6 hr Mild/Moderate pain as follows: or 650mg PR (if unable to take PO) q 4 – 6 hr Maximum 3200 mg/day Headache pain Ear, nose and/or throat pain Musculoskeletal pain Skin pain Contraindications Abdominal pain Allergy or sensitivity to acetaminophen, Ingestion of therapeutic acetaminophen in last 4 hours Hepatitis, liver disease, intoxicated patients Care Map Guidelines Cellulitis Dehydration Falls Fever Lacerations Respiratory Tract Infection Syncope Urinary Tract Infections Weakness & Dizziness CATEGORY: Medical Directives SUBJECT: Medications Page 7 of 17 Medication Order Table ED Outreach Services - Medication Directive (EDOS03) Orders Salbutamol (Ventolin) 100 mcg/puff 4 to 8 puffs by MDI and aerochamber with mask q15 – 20 ; max 3 doses OR Salbutamol (Ventolin) 5 mg/mL Indications Patients presenting with SOB and a history of asthma or Chronic Obstructive Pulmonary Disease (COPD) with one or more of the following symptoms: Cough Presence of respiratory distress, wheeze, tightness or decreased breath sounds during chest auscultation Carry out febrile respiratory illness screening on all patients. If screen is 2.5 mg in 2 ml of normal saline via positive, isolate patient prior to using nebulizer mask. Repeat q15 – 20 minutes; nebulizer. max 3 doses Contraindications Care Map Guidelines Allergy or sensitivity to salbutamol or Anaphylaxis adrenergic amines (salmeteral, terbutaline, albuterol, fomerterol) Shortness of Breath Mild/Moderate Reassess and document patient response and vital signs within 15 minutes following administration or as indicated as per HRSRH policies & procedure guidelines Utilize aerochamber for all MDI administrations Use droplet precautions CATEGORY: Medical Directives SUBJECT: Medications Page 8 of 17 Medication Order Table ED Outreach Services - Medication Directive (EDOS03) Orders Ipratropium (Atrovent) 20mcg/puff; 4 to 8 puffs via MDI and aerochamber with mask q15 – 20 minutes ; max 3 doses OR Ipratroprium (Atrovent) 250mcg/ml 250 ug in 3mls NS via nebulizer Repeat q15 – 20 minutes ; max 3 doses Indications Patients presenting with SOB and a history of asthma or Chronic Obstructive Pulmonary Disease (COPD) with one or more of the following symptoms: Cough Presence of respiratory distress, wheeze, tightness or decreased breath sounds during chest auscultation Carry out febrile respiratory illness screening on all patients. If screen is positive, isolate patient prior to using nebulizer. Contraindications Allergy or sensitivity to Ipratropium (Atrovent) Care Map Guidelines Anaphylaxis Shortness of Breath Mild/Moderate Reassess and document patient response and vital signs within 15 minutes following administration or as indicated as per HRSRH policies & procedure guidelines Utilize aerochamber for all MDI administrations Use droplet precautions CATEGORY: Medical Directives SUBJECT: Medications Page 9 of 17 Medication Order Table ED Outreach Services - Medication Directive (EDOS03) Orders Indications Contraindications Care Map Guidelines Prednisone 50 mg tablet po X 1 dose Mild/moderate SOB Allergy or sensitivity to Prednisone Shortness of Breath – Mild/Moderate Methylprednisolone Mild/moderate SOB Allergy or sensitivity to Solu-Medrol Shortness of Breath Mild/moderate (Solu-Medrol) 40mg to 125 mg IV X 1 dose Dilute in 50ml D5W or 0.9% normal saline and infuse over 15 to 30 minute CATEGORY: Medical Directives SUBJECT: Medications Page 10 of 17 Medication Order Table ED Outreach Services - Medication Directive (EDOS03) Orders Lidocaine Jelly 2%, 200 mg/10mls Approximately 5 minutes prior to any urinary catheter insertion. Indications Any patient requiring urinary catheterization who is not allergic to amide anaesthetics Apply to cover lacerations 30 minutes prior to suturing. Allergy to lidocaine or other aminetype topical anaesthetics (e.g. articaine, bupivacaine, prilocaine, mepivacaine, ropivacaine) Care Map Guidelines Foley Catheter Difficulties Urethral trauma or known structural abnormality May repeat x 2 to max of 400 mgs. EMLA topical anaesthetic Contraindications Lacerations above the fascia requiring suturing Laceration to ear, nose, fingers, toes, penis, no mucous membranes Known allergy or hypersensitivity to any compound components Lacerations CATEGORY: Medical Directives SUBJECT: Medications Page 11 of 17 Medication Order Table ED Outreach Services - Medication Directive (EDOS03) Orders Benadryl (Diphenhydramine) 50mg IM or IV x 1 dose Indications Allergic Reaction Contraindications Care Map Guidelines Known allergy or sensitivity to Diphenhydramine Anaphylaxis Known allergy or sensitivity to adrenalin Anaphylaxis Known allergy or sensitivity to Ranitidine Anaphylaxis Known allergy or sensitivity to Cephalexin Cellulitis Itchiness Rash Epi (Adrenalin) 1:1000 0.3ml IM x 1 dose Severe allergic reaction Difficulty Breathing Difficulty Swallowing Ranitidine (Zantac) 50mg IV x 1 dose Allergic Reaction Itchiness Rash Cephalexin (Keflex) 500 mg po qid First line treatment for mild/moderate cellulitis (S. aureus & Group A Strep) CATEGORY: Medical Directives SUBJECT: Medications Page 12 of 17 Medication Order Table ED Outreach Services - Medication Directive (EDOS03) Orders Indications Contraindications Ceftriaxone (Rocephin) 1gm - 2 gm IV q12-24 hr First line treatment for mild/moderate cellulitis in patients that are unable to take and do not respond to oral antibiotic Known allergy or sensitivity to Ceftriaxone Cloxacillin (Apo-Cloxi) 500mg po qid Second line treatment for mild/moderate cellulitis Known allergy or sensitivity to Cloxacillin Care Map Guidelines Cellulitis (S. aureus & Group A Strep) Cellulitis (S. aureus & Group A Strep) Patient unable to take first line antibiotics due to allergy and/or sensitivity Clindamycin (Cleocin) 300 – 450 mg po qid Second line treatment for mild/moderate cellulitis Patient unable to take first line antibiotics due to allergy or sensitivity Known allergy or sensitivity to Clindamycin Cellulitis (S. aureus & Group A Strep) CATEGORY: Medical Directives SUBJECT: Medications Page 13 of 17 Medication Order Table ED Outreach Services - Medication Directive (EDOS03) Orders Azithromycin (Zithromax) 500mg po on Day 1, then 250 mg po x 4 days Indications Contraindications Third line treatment for mild/moderate Known allergy or sensitivity to cellulitis Azithromycin Care Map Guidelines Cellulitis (S. aureus & Group A Strep) Respiratory Tract Infection (S.pneumoniae, H.influenzae, Gram –ve bacilli, S.aureus, Legionella sp., C.pneumoniae) Patient unable to take first or second line antibiotic due to allergy or sensitivity First line treatment for suspected respiratory tract infection Pancrelipase (Cotazyme) 1 capsule Blocked G-tube or feeding tube Known allergy or sensitivity to Pancrelipase G-tube / Enteral Difficulties Sodium Bicarbonate 325mg tablet Blocked G-tube or feeding tube Known allergy or sensitivity to Sodium Bicarbonate G-tube / Enteral Difficulties Trimethropin/Sulfamethoxazole (Septra) First line treatment for suspected urinary tract infection Known allergy or sensitivity to Trimethropin/Sulfamethoxazole Urinary Tract Infection (E.coli, S.saprophyticus, Gram –ve bacilli) CATEGORY: Medical Directives SUBJECT: Medications Page 14 of 17 Medication Order Table ED Outreach Services - Medication Directive (EDOS03) Orders Indications Contraindications Care Map Guidelines 2 tablets bid or 1 double strength tablet bid Note If CrCl 30-50 ml/min, reduce dose by 25% (i.e. 1.5 tabs bid) If CrCl 15-30 ml/min, reduce dose by 50% If CrCl is < 15 ml/min, do not administer Macrobid 100 mg po bid Note: If CrCl is < 60 ml/min, avoid use. Discuss with pharmacist First line treatment for suspected urinary tract infection Known allergy or sensitivity to Nitrofurantoin or Macrobid Urinary Tract Infection (E.coli, S.saprophyticus, Gram –ve bacilli) Amoxicillin (Amoxil) Second line treatment for suspected Known allergy or sensitivity to Urinary Tract Infection (E.coli, S.saprophyticus, CATEGORY: Medical Directives SUBJECT: Medications Page 15 of 17 Medication Order Table ED Outreach Services - Medication Directive (EDOS03) Orders 500 mg po q8h Indications urinary tract infection Contraindications Amoxicillin Care Map Guidelines Gram –ve bacilli) Patient unable to take first line antibiotic due to allergy or sensitivity Ciprofloxacin (Cipro) 250 – 500 mg po bid Note: If CrCl is 5-29 ml/min, administer 250 – 500 mg q 24 hrs. Amoxicillin/Clavulanate (Augmentin) 500 mg po tid OR 875 mg bid Note If CrCl 10-30ml/min, administer 250 – Second line treatment for suspected urinary tract infection Known allergy or sensitivity to Ciprofloxacin Patient unable to take first line antibiotic due to allergy or sensitivity First line treatment for suspected respiratory tract infection Known allergy or sensitivity to Amoxicillin/Clavulanate Urinary Tract Infection (E.coli, S.saprophyticus, Gram –ve bacilli) Respiratory Tract Infection (S.pneumoniae, H.influenzae, Gram –ve bacilli, S.aureus, Legionella sp., C.pneumoniae) CATEGORY: Medical Directives SUBJECT: Medications Page 16 of 17 Medication Order Table ED Outreach Services - Medication Directive (EDOS03) Orders Indications Contraindications Care Map Guidelines 500 mg q12h. If CrCl is < 10 ml/min, administer 250 – 500 mg q24 hours. The 875 mg BID dose should not be used if CrCl is less than 30 ml/min Cefuroxime-AX (Ceftin) 500 mg po bid First line treatment for suspected respiratory tract infection Known allergy or sensitivity to Cefuroxime-AX Respiratory Tract Infection (S.pneumoniae, H.influenzae, Gram –ve bacilli, S.aureus, Legionella sp., C.pneumoniae) Cefprozil (Cefzil) 500 mg po bid First line treatment for suspected respiratory tract infection Known allergy or sensitivity to Cefprozil Respiratory Tract Infection (S.pneumoniae, H.influenzae, Gram –ve bacilli, S.aureus, Legionella sp., C.pneumoniae) Note: CATEGORY: Medical Directives SUBJECT: Medications Page 17 of 17 Medication Order Table ED Outreach Services - Medication Directive (EDOS03) Orders Indications Contraindications Care Map Guidelines if CrCl is < 30ml/min, decrease dose by 50% Moxifloxacin (Avelox) 400 mg po/IV od First line treatment for suspected respiratory tract infection Known allergy or sensitivity to Moxifloxacin Respiratory Tract Infection (S.pneumoniae, H.influenzae, Gram –ve bacilli, S.aureus, Legionella sp., C.pneumoniae)