Underlying and multiple causes of disease for 6 chronic diseases
advertisement

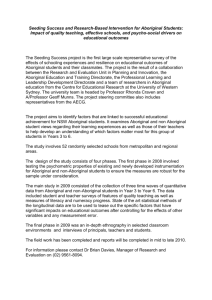
Title Page Article Title: Trends in chronic disease mortality in the Northern Territory Aboriginal population, 19972004: using underlying and multiple causes of death. WORD COUNT Abstract = 254 Main text (including references) = 2783 1 Trends in chronic disease mortality in the Northern Territory Aboriginal population, 1997-2004: using underlying and multiple causes of death Emily Fearnley, Shu Qin Li, Steven Guthridge Abstract Objective: To assess trends in chronic disease mortality in the Aboriginal population of the Northern Territory (NT), using both underlying and multiple causes of death. Method: Death registration data from 1997 to 2004, were used for the analysis of deaths from five chronic diseases; ischaemic heart disease (IHD), diabetes, chronic obstructive pulmonary disease (COPD), renal failure and stroke. Negative binomial regression models were used to estimate the average annual change in mortality rates for each of the five diseases. Chi squared tests were conducted to determine associations between the five diseases. Results: The five chronic diseases contributed to 49.3% of all Aboriginal deaths in the NT. The mortality rate ratio of NT Aboriginal to all Australian death rates from each of the diseases ranged from 4.3 to 13.0, with the lowest rate ratio for stroke and highest for diabetes. There were significant statistical associations between IHD, diabetes, renal failure and stroke. The mortality rates for diabetes, COPD and stroke declined at estimated annual rates for NT Aboriginal males of 3.6%, 1.0% and 11.7% and for Aboriginal females by 3.5%, 6.1% and 7.1% respectively. There were increases in mortality rates for Aboriginal males and females for IHD and a mixed result for renal failure. Conclusion: NT Aboriginal people experience high chronic disease mortality; however mortality rates appear to be declining for diabetes, COPD and stroke. The impact of chronic 2 disease on mortality is greater than previously reported by using a single underlying cause of death. The results highlight the importance of integrated chronic disease interventions. Introduction An epidemic of chronic disease has developed in Aboriginal Australians commencing in the early 1980s (1). The mortality rate in the Northern Territory (NT) Aboriginal population has been reported as greater than for other Australians (2-4), and although declines have been observed in the overall rate of NT Aboriginal mortality over four decades (1966 – 2001), the reduction has been less than in the total Australian population (2). A recent analysis of longterm trends in NT Aboriginal chronic disease mortality identified a significant increase in mortality rates for ischaemic heart disease (IHD) and diabetes over the 25 years, from 1977 to 2001 (5). Another study assessed the cause of the life expectancy gap between NT Aboriginal and non-Aboriginal people, and highlighted that through the 80’s and 90’s there was an increasing contribution from non-communicable and lifestyle diseases, which has offset a declining contribution from communicable diseases (4). Other authors have noted that as life expectancy increases, the major health conditions in a population shift towards chronic diseases (6). A characteristic of chronic diseases is that many have shared risk factors and frequently co-exist with other chronic diseases (6,7). Assessing the co-occurrence of chronic diseases helps to identify those diseases that are more likely to occur together, allowing the design of appropriate and targeted interventions. Historically, mortality studies have relied on the use of a single, underlying cause of death; which is the disease or condition that led directly to death (8). This provides useful, but limited information particularly for chronic diseases such as diabetes which are less likely to 3 be reported as the underlying cause of death (8). As a result, the contribution of chronic diseases to total mortality has been under-estimated. In 1997, the Australian Bureau of Statistics (ABS) introduced coding for multiple or associated causes of death in death registration data (8). The use of multiple causes of death coding in mortality data provides the opportunity to gain a more comprehensive view of health within a population, including information about the interaction of diseases and of the contributing causes of death (7, 9,10,11). Reports which utilise multiple causes of death are starting to appear in the literature, including a recent analysis of all-cause and cause-specific death rates for the NT Aboriginal population by varying levels of geographic remoteness (12). In recent years, concerted efforts have been made in the NT to tackle chronic diseases, with strategies including early screening and active clinical intervention (13). A systematic chronic disease strategy was established in the NT in 1999 and it is timely to assess changes that may have occurred in association with the more focused and collective efforts. This study examines the contribution of five common chronic diseases within the NT by using both underlying and multiple causes of death. The study also analyses time trends in morality rates and the associations between each of the five selected chronic diseases as causes of death. Methods Data for this study were obtained from two sources: NT and Australian death data from the ABS death registration data, and NT and Australian estimated resident population from the ABS 2001 Census of Population and Housing. The NT deaths included in this study were the deaths of all NT residents occurring in Australia, with separate analysis for the Aboriginal and non-Aboriginal population. The quality of Indigenous status in death registration and population data within the NT is high and has been previously reported as acceptable for trend 4 analysis (14). From 1997, the ABS has classified both underlying and multiple causes of death, by using the International Classification of Diseases (ICD 10) tenth revision for death registration (8). The five common, chronic diseases included in this study are ischaemic heart, disease (IHD), diabetes, stroke, chronic obstructive pulmonary disease (COPD) and renal failure. The ICD 10 codes used are listed in Table 1. Total numbers and percentages of deaths were calculated for all five chronic diseases, by underlying and multiple causes of death. NT mortality rates for each disease were calculated using direct standardisation and age-adjusted to the Australian standard population (2001). Chi squared analyses were conducted using two by two tables to determine associations between chronic diseases. The Bonferroni method was used to adjust the cut off for statistical significance testing for multiple hypothesis tests. Age-adjusted mortality rate ratios (MRR) were used to determine differences in rates in the NT Aboriginal population compared to the Australian population. A negative binomial regression model was used to estimate the average annual change in mortality rate for each of the five chronic diseases for the NT Aboriginal population compared with NT non-Aboriginal population and the Australian population. Various interaction terms were added to the negative binomial regression model to test differences in annual changes between the NT Aboriginal population and all Australians . All statistical analysis was conducted using Stata software (version 9.0; StataCorp, College Station, Texas, USA). The project was approved by the Human Research Ethics Committee of the Department of Health and Community Services and Menzies School of Health Research (Project number 07/69), and the Australian National University Human Research Ethics Committee (Protocol number 2007/2265). 5 Results Between 1997 and 2004, there were a total of 3438 deaths among NT Aboriginal residents. Of this total, 1115 (32.4%) deaths listed one of the five selected chronic diseases assessed in this paper as the underlying cause of death. A further 579 (16.8%) deaths listed at least one of the five chronic diseases as a multiple cause of death, without another of the five diseases listed as the underlying cause of death. A total of 1694 (49.3%) NT Aboriginal deaths had at lest one of the five chronic diseases listed as either the underlying or multiple cause of death. Using both underlying and multiple causes, IHD was identified as the leading chronic disease that contributed to deaths, with 711 (20.7%) deaths followed by diabetes (524, 15.2%), renal failure (518, 15.1%), COPD (396, 11.5%), and stroke (299, 8.7%). Among Aboriginal people who died of IHD, 474 (66.7%) had IHD recorded as the underlying cause of death and for another 237 (33.3%), IHD was recorded as one of the multiple causes of death. In contrast, diabetes, renal failure, COPD and stroke were more likely to be recorded as a multiple cause than underlying cause of death. The ratio of multiple to underlying cause of death for diabetes, renal failure, COPD and stroke were 1.3, 4.6, 1.2 and 1.1 respectively (Table 2). Deaths due to renal disease were the least common of the five chronic diseases to be reported as the underlying cause of death, with only 93 deaths listing renal disease as the underlying cause, but an additional 425 deaths listed renal disease as a multiple cause of death. Figures 1 and 2 outline the age-adjusted mortality rates for five chronic diseases by all contributing causes of death, for NT Aboriginal population compared with NT nonAboriginal population and all Australian. The age-adjusted mortality rates for all five chronic 6 diseases were much higher in the NT Aboriginal than both NT non-Aboriginal and all Australian populations, especially for diabetes and renal disease in Aboriginal females. The co-occurrence of the five chronic diseases by Indigenous status is presented in Table 3. A significantly high level (P<0.0127) of association was observed between a number of diseases, including IHD and diabetes, IHD and renal failure, IHD and stroke, diabetes and stroke, diabetes and renal failure. The age adjusted mortality rate ratio (MRR) of NT Aboriginal deaths to all Australian deaths was statistically significant for all five chronic diseases, using all contributing causes of death and ranged from the lowest 4.3(3.5, 5.1) for stroke to the highest 13.0, (11.3, 14.9) for diabetes (Table 4). Similarly, the mortality rate ratios of NT Aboriginal deaths to NT nonAboriginal deaths were also significantly higher for all five chronic diseases, and ranged from 4.1 (3.3, 5.0) for stroke to 10.3 (8.3, 12.8) for renal failure The negative binomial regression model estimated average annual changes in all contributing causes of death rate for each of the five chronic diseases are presented in Table 5. While most changes are not statistically significant they indicate important and sometimes substantial changes. The mortality rate for IHD increased in the NT Aboriginal population, with an annual increase of 1.3% (-5.0, 8.1) in Aboriginal males and 2.9 %(-5.2, 11.7) for Aboriginal females compared to reductions of 3.5%,(-7.2, 0.2) in Australian males and 3.2% (-7.6, 1.4) in females. There was a greater reduction in the annual mortality rate for diabetes in the NT Aboriginal males (-3.6%, (-8.8, 1.9)) and NT Aboriginal females (-3.5%,(-9.4, 2.9)) compared with the smaller declines for Australian males (-0.6%, (-1.6,0.3)) and Australian females (1.3%, (-4.2, 1.7) .The mortality rate from COPD declined for both the NT Aboriginal 7 population and all Australians, with average annual declines of 1.0% (-9.6, 8.4) in NT Aboriginal males and 6.1 (-12.3, 0.6) compared with a decline of 5.0% (-10.2, 0.5) for Australian males and 2.8% (-4.5, 1.0) for Australian females. The mortality rate from stroke declined in both the NT Aboriginal population and all Australians population, with a greater reduction in average annual mortality rate 11.7%, (-19.5, -3.1) for NT Aboriginal males and 7.1% (-15.8, 2.4) for NT Aboriginal females. There was a mixed pattern observed for death from renal failure in the NT Aboriginal population. The estimated annual reduction rate in NT Aboriginal males was 1.3% (-9.4, 7.6) whereas there was an annual average increase of 4.4% (-3.7, 13.2) in NT Aboriginal females. These rates compare with the annual reductions of 4.5% (-9.4, 7.6) in Australian males and 2.0% (-7.2, 3.5) in Australian females. Discussion The combination of underlying and multiple causes of death provides a more comprehensive overview of mortality, including a more complete assessment of the burden of chronic diseases within a population, than available from the sole use of underlying cause of death data (7,8,9,10,11). The previous underestimation of the impact of a specific disease is especially evident within this study for renal disease, for which the burden of the disease was more than four times greater if multiple causes of death were considered compared to limiting analysis to the underlying cause of death. Previous studies have highlighted that certain chronic diseases; particularly diabetes, COPD, stroke, and renal disease are frequently overlooked as the underlying cause of death, a shortcoming that is addressed by use of multiple cause of death data (7, 9). This study highlights the substantial contribution these chronic diseases made to the overall mortality in the NT Aboriginal population, and the associated need for appropriate health policy and action to target the prevention and reduction of chronic diseases. 8 The poor health status and higher mortality rate of the NT Aboriginal population has been well documented (2-4). There are many factors that contribute to the higher chronic disease mortality rates including social disadvantage, poor access to primary health care and high prevalence of smoking (6, 15). This study emphasises the association between chronic diseases, with people who had one of the selected chronic diseases as a cause of death more likely to have had other chronic diseases. This is partially explained by the shared risk factors of chronic diseases including poor nutrition, lack of exercise, smoking and high alcohol intake (6). Most of the selected chronic diseases were significantly associated with one another. The co-occurrence of chronic diseases reinforces the importance of an integrated approach to tackle common chronic diseases. The Northern Territory Department of Health and Families developed the first integrated non-communicable diseases strategy in Australia (13) and collective efforts have been made for more than a decade to reduce the morbidity and mortality of chronic diseases in the Northern Territory through screening, prevention and clinical management. A recent study shows improvements in life expectancy in the NT Aboriginal population in the recent decades (16). Another NT study reports that between 1990 and 2001, the death rate from some chronic diseases such as COPD and stroke declined in the NT Aboriginal population, but increased for IHD and diabetes (5). Using both underlying and multiple cause of death, and more recent data, the current study provides a more comprehensive picture of mortality ascribed to chronic disease in the NT Aboriginal population. This study found that the death rate from diabetes, COPD and stroke have all declined between 1997 and 2004 in the NT Aboriginal population and a decline in mortality rate was also observed in renal failure death in NT Aboriginal males. Although not statistically significant, the reduction in 9 annual mortality rate in diabetes and stroke were much higher in the NT Aboriginal population and this may indicate early signs of improvement in chronic disease mortality. The results support an argument that collective efforts in early screening and treatment of chronic diseases are resulting in improved health outcomes in the NT. There remain areas of continuing concern, particularly the increasing death rates from IHD in NT Aboriginal males and females and from renal failure in NT Aboriginal females. A recent paper demonstrated the complexity of the challenge to reduce mortality rates, when reporting that improved survival after Acute Myocardial Infarction (AMI) for the NT Aboriginal population was counterbalanced by the increasing AMI incidence (17). It is likely that parallel increases in other chronic diseases are placing a similar brake on improved outcomes. The limitations of this study include the reliance on data collection from death certificates, which have a number of imperfections, including that coding practices are known to change over time (9, 18). Another limitation of this study is the relatively short time period that data on multiple cause of death has been available. This period was constrained on one hand by the introduction of multiple causes of death coding in 1997, and on the other by the availability of data up until 2004, at the time of the study. The death registration and coding process is often lengthy and incomplete until a number of years after deaths have occurred. References 1. Australian Bureau of Statistics and Australian Institute of Health and Welfare. The Health and welfare of Australia’s Aboriginal and Torres Strait Islander peoples 2005. Canberra (ACT): ABS; 2005. Catalogue. No.: 4704.0. 2. Condon JR, Barnes T, Cunningham J, Smith L. Improvements in Indigenous mortality in the Northern Territory over four decades. Aust N Z J Public Health 2004;28:445-51. 10 3. Cunningham J, Paradies Y. Mortality of Aboriginal and Torres Strait Islander Australians 1997. Canberra (ACT): Australian Bureau of Statistics; 2000. Occasional Paper No.: 3315.0. 4. Zhao Y, Dempsey K. Causes of inequality in life expectancy between Indigenous and non-Indigenous people in the Northern Territory, 1981-2000: a decomposition analysis. Med J Aust 2006;184:490-4. 5. Thomas DP, Condon JR, Anderson IP, Li SQ, Halpin S, Cunningham J, et al. Longterm trends in Indigenous deaths from chronic diseases in the Northern Territory: a foot on the brake, a foot on the accelerator. Med J Aust 2006;185:145-9. 6. Condon JR, Warman G, Arnold L. The health and welfare of Territorians. Darwin (NT): Territory Health Services; 2001. p. 97-104. 7. Tardon AG, Zaplana J, Hernandez R, Cueto A. Usefulness of the codification of multiple causes of death in mortality statistics. Int J Epidemiol 1995;24:1132-7. 8. Australian Bureau of Statistics. Multiple cause of death analysis, 1997-2001. Canberra (ACT): ABS; 2003. Catalogue. No.: 3319.0.55.001. 9. Li SQ, Cunningham J, Cass A. Renal-related deaths in Australia 1997-1999. Intern Med J 2004;34:259-65. 10. Redelings MD, Sorvillo F, Simon P. A comparison of underlying cause and multiple causes of death. Epidemiology 2006;17:100-3. 11. Mackenbach JP, Kunst AE, Lautenbach H, Bijlsma F, Oei YB. Competing causes of death: An analysis using multiple cause of death data from The Netherlands. Am J Epidemiol 1995;141:466-75. 12. Andreasyan K, Hoy WE. Patterns of mortality in Indigenous adults in the Northern Territory, 1998-2003: are people living in more remote areas worse off? Med J Aust 2009;190:307-11. 11 13. Weeramanthri T, Morton S, Hendy S, Connors C, Rae C, Ashbridge D. Northern Territory preventable chronic disease strategy – Overview and framework. Darwin (NT): Territory Health Services; 1999. 14. Condon JR, Barnes T, Cunningham J, Smith L. Demographic characteristics and trends of Northern Territory Indigenous population, 1966 to 2001. Darwin (NT): Cooperative Research Centre for Aboriginal Health. Occasional Paper. 2004. 15. Cunningham J. Cigarette smoking among Indigenous Australians, 1994. Canberra (ACT): Australian Bureau of Statistics; 1997. Occasional Paper Catalogue No.: 4701.0. 16. Wilson T, Condon JR, Barnes T. Northern Territory Indigenous life expectancy improvements, 1967-2004. Aust N Z J Public Health 2007;31:184-8. 17. You JQ, Condon J, Zhao Y, Guthridge S. Incidence and survival analysis for acute myocardial infarctions in the Northern Territory, 1992–2004. Med J Aust .MJA 2009; 190 (6): 298-302 18. Mckenzie K, Tong S, Walker S, Sadkowsky K. Evolution in classifying mortality statistics. Canberra. The National Centre for Classification in Health.2002. 12 Table 1 ICD 10 codes for IHD, diabetes, stroke, COPD and renal failure Conditions Ischaemic heart disease Diabetes Stroke COPD Renal failure ICD 10 Codes I20, I21, I22, I23, I24, I25 E10, E11, E13, E14 I6 J40, J41, J42, J43, J44, J47 N17, N18, N19 Table 2 Number of underlying and multiple causes of death reported for selected five chronic diseases by Indigenous status, NT population, 1997 – 2004. Underlying cause of death IHD Diabetes COPD Renal Stroke NT Aboriginal 474 226 180 93 142 NT nonAboriginal Total 525 999 86 312 173 353 25 118 175 317 Multiple cause of death NT Aboriginal 237 298 216 425 157 NT nonAboriginal Total 279 516 190 488 220 436 219 644 144 301 Ratio of Multiple to Underlying NT Aboriginal 0.5 1.3 1.2 4.6 1.1 NT nonAboriginal Total 0.5 0.51 2.2 1.56 1.3 1.23 8.8 5.5 0.8 0.9 13 Figure 1 Age-adjusted mortality rates per 100 000 population for selected chronic diseases, males, 1997-2004. NT Aboriginal males NT non-Aboriginal males COPD per 100 000 population Diabetes Age adjusted death rate Australia males 600 500 400 300 200 Stroke Renal 0 IHD 100 Figure 2 Age-adjusted mortality rates per 100 000 population for selected chronic diseases, females, 1997-2004. Age adjusted death rate, per 100 000 population NT Aboriginal females NT non-Aboriginal females Australia females 600 500 400 300 200 100 Stroke Renal COPD Diabetes IHD 0 14 Table 3 The association of five chronic diseases as reported causes of death, by Indigenous status, Northern Territory 1997– 2004 Co-conditions for IHD deaths Diabetes Renal COPD Stroke Aboriginal % (p) 27.6 (0.000)* 18.6 (0.003)* 13.7 (0.045) 5.5 (0.001)* Non-Aboriginal % (p) 17.9 (0.000)* 10.7 (0.000)* 15.6 (0.000)* 7.5 (0.042) Co-conditions for diabetes deaths IHD Renal Stroke COPD Co-conditions for COPD deaths IHD Renal Diabetes Stroke Aboriginal % (p) 24.5 (0.045) 15.2 (0.964) 12.9 (0.163) 6.8 (0.158) Non-Aboriginal % (p) 31.8 (0.000)* Diabetes 6.6 (0.688) IHD 11.2 (0.014) COPD 7.9 (0.311) Stroke Aboriginal % (P) Non-Aboriginal % (p) 37.4 (0.000)* 52.2 (0.000)* 34.5 (0.000)* 15.9 (0.014) 12.6 (0.001)* 13.8 (0.007)* 9.7 (0.163) 15.9 (0.000)* Co-conditions for renal deaths Aboriginal % (p) Non-Aboriginal % (p) 34.9 (0.000)* 23.0 (0.000)* 25.5 (0.003)* 35.3 (0.000)* 11.6 (0.964) 10.7 (0.688) 8.9 (0.872) 8.2 (0.544) Co-conditions for stroke deaths Aboriginal % (p) Non-Aboriginal % (p) Diabetes 22.1 (0.001)* 11.9 (0.007)* Renal IHD 15.4 (0.872) 13.0 (0.001)* 6.3 (0.544) 18.8 (0.042) COPD 9.0 (0.158) 9.7 (0.311) Note: * Significant at P<0.0127 as per Bonferroni method to adjust for multiple comparisons. 15 Table 4 Age-adjusted mortality rate ratios (MRR) for mortality rates by disease, in NT Aboriginal population compared with NT non-Aboriginal population and all Australia , 1997–2004. NT Aboriginal to NT non- NT non- Aboriginal to NT Aboriginal to Australia Aboriginal Australia 8.4 (7.1,10.0) 5.0 (4.1,6.0) 1.0 (1.0,1.4) 13.0 (11.3,14.9) 9.0 (7.4,11.1) 1.3 (1.1,1.5) COPD 10.3 (8.6,12.5) 5.3 (4.2,6.6) 1.7 (1.4,2.0) Renal 10.9 (9.2,12.9) 10.3 (8.3,12.8) 1.0(0.8,1.2) 4.3 (3.5,5.1) 4.1 (3.3,5.0) 1.0 (0.8,1.2) Conditions IHD Diabetes Stroke Table 5 Annual changes in NT Aboriginal and Australian mortality rates, for five chronic diseases, by gender, 1997–2004. Condition IHD NT Indigenous male NT Indigenous female Australia male Australia female 1.3 (-5.0,8.1) 2.9 (-5.2,11.7) -3.5 (-7.2,0.2) -3.2 (-7.6,1.4) -3.6 (-8.8,1.9) -3.5 (-9.4,2.9) -0.6 (-1.6,0.3) -1.3 (-4.2,1.7) -11.7 (-19.5, -3.1) -7.1 (-15.8,2.4) -2.7 (-7.7,2.6) -4.6 (-9.7,0.7) -1.0 (-9.6,8.4) -6.1 (-12.3,0.6) -5.0 (-10.2,0.5) -2.8 (-4.5,1.0) -1.3 (-9.4,7.6) 4.4 (-3.7,13.2) -4.5 (-9.4,7.6) -2.0 (-7.2,3.5) Diabetes Stroke COPD Renal failure 16 17