Bronchopulmonary dysplasia (BPD) is the chronic respiratory
advertisement
 is the chronic respiratory")
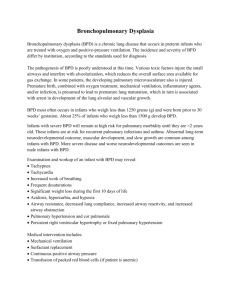
CHRONIC LUNG DISEASE OF PREMATURITY: LONG-TERM RESPIRATORY OUTCOME Eugenio Baraldi, MD Department of Pediatrics, University of Padova, Italy Bronchopulmonary dysplasia (BPD) is a chronic respiratory disease that develops as a consequence of perinatal/neonatal lung injury, and it is one of the most important sequelae of premature birth. The diagnosis of BPD is currently based on the need for supplemental oxygen for at least 28 days after birth, and its severity is graded according to the respiratory support required at 36 postmenstrual weeks. BPD almost always occurs in neonates who are delivered at a gestational age of less than 30 weeks and who have a birth weight of less than 1500 g. These are about 1.5% of all newborns and BPD develops in about 20% of them. Today BPD is mainly a developmental disorder in which the immature lung fails to reach its full structural complexity. Longitudinal studies on children with BPD identified, at all ages, increased rates of chronic coughing and wheezing, a greater need to use inhaled asthma medications and a significant airflow obstruction. Children who have survived BPD and children with asthma share some clinical and functional characteristics, but available evidence suggests that the two obstructive lung diseases do not have the same underlying airway inflammation. Spirometric values reflecting airflow, such as FEV1, are consistently lower in survivors of BPD into adolescence and young adulthood than in controls born at term rising the concern that the chronic lung disease after premature birth may predispose to the development of a chronic obstructive pulmonary disease (COPD)-like phenotype with aging. This is an open question that only follow-up and lung function studies extended to middle-age and beyond will answer. Unfortunately, no pathologic data are available elucidating which structural and pathophysiological alterations underlie the clinical and functional pulmonary abnormalities seen at long-term in some subjects delivered prematurely. A relevant question is whether the long-term pulmonary consequences of prematurity and BPD essentially depend on a non-progressive reduction of the airway caliber, due to a stabilized, non-progressive structural damage of the airways, or instead also reflect an active airway disease. Chronic lung disease of prematurity can no longer be considered only a pediatric disease and also family doctors and chest physicians should be aware of this “new” Chronic Obstructive Pulmonary Disease. References Jobe AH, Bancalari E. Bronchopulmonary dysplasia. Am J Respir Crit Care Med 2001;163:1723-9. Baraldi E, Filippone M. Chronic lung disease after premature birth. New Eng J Med 2007;357:1946–1955. Kinsella JP, Greenough A, Abman SH. Bronchopulmonary dysplasia. Lancet 2006;367:1421-31. Filippone M, Bonetto G, Cherubin E, Carraro S, Baraldi E. Childhood course of lung function in survivors of bronchopulmonary dysplasia. JAMA 2009, 302:1418-20.