Supplemental Digital Content 1. Reactogenicity and Safety Assessment
Methods
Reactogenicity and safety were evaluated using diary cards that were completed by the
children’s parents/guardians. Specific symptoms commonly associated with injectable
childhood vaccines were actively solicited for 4 days (day 0–3) after vaccination, including
local (pain, redness, swelling at the injection sites) and general (fever, drowsiness,
irritability/fussiness, loss of appetite) symptoms. Temperatures recorded on a daily basis by
parents/guardians with a digital thermometer provided at the time of enrolment were taken by
the axillary route and, for analysis, adjusted to the equivalent rectal temperature by
increasing temperatures by 0.5°C, to be consistent with previous Hib-MenC-TT studies.
Unsolicited adverse events (AEs) and serious adverse events (SAEs), defined as any
medical event resulting in death, any life-threatening event, any event causing disability, or
requiring hospitalization or prolongation of hospitalization, were recorded within a 31-day
(days 0–30) follow-up period after vaccination. SAEs considered by the investigator to be at
least possibly related to vaccination were also recorded up to 12 months after vaccination.
The intensity of each symptom was graded on a scale from 0 (absent) to 3 (severe) by the
children’s parents/guardians. Grading was reviewed by study staff when diary cards were
returned. Pain at the injection site was considered to have a grade 3 intensity if the child cried
when the limb was moved or was spontaneously painful; redness and swelling at the injection
site if the diameter was >30 mm (parents/guardians were issued a measuring ruler at study
enrolment); and fever if rectal temperature was >40°C (axillary temperature >39.5°C).
Irritability/fussiness and drowsiness were considered of grade 3 intensity if the child cried and
could not be comforted or it prevented normal activity, and for loss of appetite if the child did
not eat at all. Grade 3 intensity for all unsolicited symptoms was defined as preventing normal
everyday activity, such as preventing attendance at day-care center and/or causing
parents/guardians to seek medical advice. All local symptoms were defined in the protocol as
causally related to vaccination. Investigators assessed the presence or absence of a possible
causal relationship to vaccination of systemic symptoms.
Analyses of safety were performed on the total vaccinated cohort. Incidences of solicited
symptoms and AEs were calculated with exact 95% CIs, and exploratory comparisons
between the 2 groups and the Hib priming vaccine subgroups were performed using a 2sided P-value from the Fisher’s exact test (P <0.05 indicating statistical significance).
Results
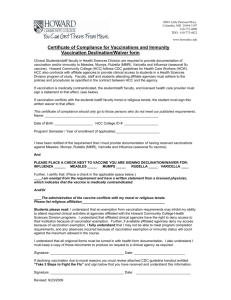
The incidence of any local symptom during the 4-day post-vaccination period was statistically
significantly lower in the Hib-MenC group compared to the Hib+MCC group (59.3% versus
78.9%; P <0.001), but there was no significant difference in the incidence of grade 3 local
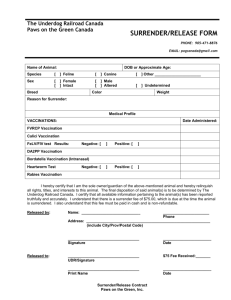
symptoms (0.9% versus 3.7%, respectively; P = 0.071) (Figure 1). Redness was the most
frequently reported solicited local symptom in both groups. A statistically significantly lower
percentage of children in the Hib-MenC group experienced redness (45.1% versus 58.7%; P
= 0.015) and swelling (24.1% versus 37.6%; P = 0.009) (Figure 2).
The incidence of any general symptom during the 4-day post-vaccination period was
statistically significantly lower in the Hib-MenC group compared to the Hib+MCC group
(73.8% versus 84.4%; P = 0.026), with similar incidences of grade 3 general symptoms in
both groups (7.4% and 7.3%) (Figure 1). Irritability/fussiness was the most frequently
reported solicited general symptom in both groups (Figure 2); this was reported in a
statistically significantly lower percentage of children in the Hib-MenC group (47.5% versus
63.3%; P = 0.005). Fever was reported in 23.5% of children in the Hib-MenC group and
27.5% in the Hib+MCC group, with grade 3 fever (>40°C) in 2 children in the Hib-MenC group
and 1 child in the Hib+MCC group (Figure 2); all 3 cases were considered related to
vaccination. There was no indication of different reactogenicity when primed with DTPa/Hib
or Hib-OMP (data not shown).
During the 31-day post-vaccination period, the most common unsolicited AEs related to
vaccination were pyrexia, reported in 4.6% of the Hib-MenC group and 7.3% of the Hib+MCC
group, and rash (4.6% and 11.9%, respectively). Most cases of pyrexia and rash related to
vaccination occurred 6 to 14 days after immunization, within the incubation period for the
measles component of the MMR vaccine. Grade 3 pyrexia considered related to vaccination
was reported in 2 children (0.6%) in the Hib-MenC group and 4 children (3.7%) in the
Hib+MCC group. Grade 3 rash was reported in 3 children (2.8%) in the Hib+MCC group; all
were considered related to vaccination. SAEs were reported in 6 children during the 31-day
post-vaccination period. One child in the Hib+MCC group developed fever, rash, and
irritability with onset 9 days after vaccination and was hospitalized for viral upper respiratory
tract infection with viral exanthema. Rash and fever were considered as possibly related to
MMR vaccination. The child recovered without sequelae after 5 days. No SAEs considered
related to vaccination were reported between the end of the vaccination phase and the year 1
follow-up visit.
SDC1/FIGURE 1. Percentage (95% CI) of children reporting any symptoms, general
symptoms, and local symptoms, of any and grade 3 intensity (solicited and unsolicited),
during the 4-day post vaccination period (total vaccinated cohort). The difference between the
Hib-MenC and Hib+MCC groups was significant for any general symptom (*P = 0.026) and
any local symptom (**P <0.001) of any intensity.
*
100
* *
% children
80
Hib-MenC
Hib+MCC
60
40
20
0
Any
General
Local
Hatched area indicates symptoms of grade 3 intensity
Local symptom of grade 3 intensity: pain, crying when limb was moved/spontaneously painful;
redness/swelling, diameter >30 mm. General symptom of grade 3 intensity: fever, rectal temperature
>40°C (axillary temperature 39.5°C); irritability, crying that could not be comforted/prevented normal
activity; drowsiness, prevented normal activity; loss of appetite, child did not eat at all.
SDC 1/FIGURE 2. Percentage (95% CI) of children reporting specific solicited local and
general symptoms, of any and grade 3 intensity, during the 4-day post vaccination period
(total vaccinated cohort). The difference between the Hib-MenC and Hib+MCC groups was
significant for redness (*P = 0.015), swelling (**P = 0.009), and irritability/fussiness (***P =
0.005) of any intensity, and redness of grade 3 intensity (#P = 0.037).
***
80
*
60
% children
**
Hib-MenC
Hib+MCC
40
20
#
0
n
Pai
s
nes
Red
s
ines
ling
l
s
e
w
Sw
Dro
ess
tite
er
ssin f appe
u
F
Fev
/
ity
so
abil
Los
Irrit
Hatched area indicates symptoms of grade 3 intensity
Local symptom of grade 3 intensity: pain, crying when limb was moved/spontaneously painful;
redness/swelling, diameter >30 mm. General symptom of grade 3 intensity: fever, rectal temperature
>40°C (axillary temperature 39.5°C); irritability, crying that could not be comforted/prevented normal
activity; drowsiness, prevented normal activity; loss of appetite, child did not eat at all.
Discussion
Reactogenicity in the Hib-MenC group was generally in line with previous studies with the HibMenC-TT vaccine when given as a 3-dose primary vaccination course in infancy.1,2 The
significantly lower incidence of solicited local symptoms, redness and swelling, in the Hib-MenC
group was consistent with the lower number of injections given in this group in comparison to
the Hib+MCC group (2 versus 3 injections). The incidence of irritability was also significantly
lower for children in the Hib-MenC group compared to the Hib+MCC group. The observed
pattern in incidences of rash and pyrexia, which peaked around 6 to 14 days after vaccination,
was consistent with previous reports of these AEs associated with the measles component of
MMR vaccination.3 Incidences of symptoms and AEs by type of primary Hib vaccine were in the
same range as the overall reactogenicity and safety results, indicating that the 2 different Hib
priming vaccines did not alter vaccine safety.
References
1. Schmitt HJ, Maechler G, Habermehl P, et al. Immunogenicity, reactogenicity, and immune
memory after primary vaccination with a novel Haemophilus influenzae-Neisseria meningitidis
serogroup C conjugate vaccine. Clin Vaccine Immunol. 2007;14:426-434.
2. Tejedor JC, Moro M, Ruiz-Contreras J, et al. Immunogenicity and reactogenicity of primary
immunization with a novel combined Haemophilus influenzae type b and Neisseria
meningitidis serogroup C-tetanus toxoid conjugate vaccine coadministered with a diphtheriatetanus-acellular pertussis-hepatitis B-inactivated poliovirus vaccine at 2, 4 and 6 months.
Pediatr Infect Dis J. 2007;26:1-7.
3. Virtanen M, Peltola H, Paunio M, Heinonen OP. Day-to-day reactogenicity and the healthy
vaccinee effect of measles-mumps-rubella vaccination. Pediatrics. 2000;106:E62.
 0
0