Research Paper - Psycho Genomics Research Institute
advertisement

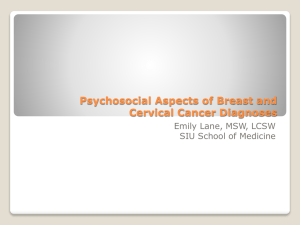
Stressors, psycho-genomic pathways and cancers Identifying psychological, psychosocial, physiological, environmental & genomic pathways to prevent and treat cancers The Power Thinking Health Council has been established to encourage and develop psycho-genomic research in order to explore these links and identify possible methods of preventing and treating cancer. Contact details: Theo Richter FPNA, President, Psycho-Genomics Research Institute research@psycho-genomics.org Stressors ____________________________________________________________ 1 Physiology and stress __________________________________________________ 2 Emotions & stress views from the Institute of HeartMath® ____________________ 3 Psychological & psychosocial interventions and cancer ______________________ 4 DNA, genes, predisposition & cancer _____________________________________ 6 Conclusion _________________________________________________________ 11 Bibliography ________________________________________________________ 12 Abstract Various experiments and clinical research have identified links between stressors and psychological, psychosocial, environmental factors and genes which may provide a basis for treatment and prevention of cancers. This paper considers existing research into cancer predisposing genes and the psychological, psychosocial, and environmental factors which may be involved. Stressors The Breast Cancer at the ABC Toowong Queensland: Third Progress Report from the Independent Review and Scientific Investigation Panel, (2006) (Third Progress Report) reported on what has been referred to as a review of a cluster of women with breast cancer in a work place in Queensland noting “Stress and an individual’s response to it are popularly believed to be important factors in causing cancer.” (p.29). The Third Progress Report cautioned, however, that a recent critical review of psychological factors and cancer development by Garrsen (2004) concluded that: “…there is not any psychological factor for which an influence on cancer development has been convincingly demonstrated in a series of studies.” (p.29). On the other hand, another review, by Butow et al (2000), also referred to in the Third Progress Report, that focused specifically on breast cancer and commissioned by Australia’s National Breast Cancer Centre, noted that while research had not indicated that psychosocial factors played a major role in the development of breast cancer, “… few studies have been of sufficient quality to state definitively that such a role does not exist.” (p.29). While Butow et al (2000) observed that the strongest psychosocial factors associated with the development of breast cancer are emotional repression (especially repression of anger) and severely threatening life events such as the death of a significant other, results from a more recent prospective cohort study with follow up over 9 years, by White et al (2007) suggested that anger control and negative affect are not connected with breast cancer, melanoma, or total cancer, although they may have a small role in the risk of prostate, colorectal and lung cancer. The conclusions by White et al (2007) noted that although more research is needed to confirm the latter associations, the results suggested that if affective states are associated with cancer development, the association may differ for different cancers and argue against the use of total cancer as an outcome measure for studies in this area. Physiology and stress Research over the years has identified the physiological effects of different levels of stress on various bodily functions. The table below (Melhuish, 1978) summarizes early research that is still useful today. Normal (relaxed) Under pressure Acute pressure Chronic pressure (stress) Brain blood supply normal blood supply up thinks more clearly headaches or migraines, tremors and nervous tics Mood happy serious increased concentration anxiety, loss of sense of humour Saliva normal reduced reduced dry mouth, lump in throat Muscles blood supply normal blood supply up improved performance muscular tension and pain Heart normal rate and increased rate and hypertension improved performance blood pressure blood pressure and chest pains Lungs normal respiration Stomach reduced blood normal blood supply and supply and acid increased acid secretion secretion Bowels normal blood supply and bowel activity increased respiration rate improved performance coughs and asthma ulcers due to reduced blood supply heartburn and reduces digestion indigestion. reduced blood supply and increased bowel activity reduced blood supply abdominal pain reduces digestion and diarrhoea frequent urination frequent frequent urination due urination, to increased nervous prostatic stimulation symptoms Bladder normal Sexual Organs (m) impotence (male) normal. (decreased blood decreased blood (female) normal supply) (f) irregular supply periods etc periods Skin healthy decreased blood supply - dry skin oxygen normal: oxygen consumption up, consumed, Biochemistry glucose glucose and and fats fats liberated. consumption up decreased blood supply (m) impotence. (f) menstrual disorders dryness and rashes more energy rapid tiredness immediately available Source: Melhuish, A, Executive Health, London Business Books with extracts from Andy Ellis, Ruskin College, Oxford, UK, 1978 Emotions & stress views from the Institute of HeartMath® The Institute of HeartMath is a non-profit organization based in California USA. It states on its website that it is a recognised global leader in researching the critical link between emotions, heart-brain communication and cognitive function. For our discussion purposes, it notes on its website that stress and emotions cannot be separated. Dr. Rollin McCraty, Director of Research for the Institute of HeartMath, in an article “Are we resigned to stress “ says, "On-going, low grade stress can do more harm to the body, mind and emotions than one large stressful event can.” Further in the HeartMath article, Psychologist Deborah Rozman, Ph.D., founding partner of HeartMath, says: The majority of people believe that emotions just happen to them. We haven't been taught that we can shift out of stressful emotions. But it's important to understand that stress is accumulated by carrying around unsettled or negative feelings without resolving them. The lack of understanding about how to address our emotions is one of the real causes for today's stress epidemic. Our brain's neural circuitry is designed to create habits to make it easier to perform tasks without having to think much about them. Each time you repeat a habit, whether an attitude, behaviour or a repetitive task like driving a car, it becomes more reinforced and unconscious. According to HeartMath, the same is true with stress. One way HeartMath says you can stop the negative emotional experiences from accumulating is to learn to track the more subtle emotional reactions. They suggest thinking of the emotions as sound effects. Your outer sound effects, such as sighs, swear words, negative humour and expressions whispered under your breath can give you clues to the real feelings underneath. Your "inner sonics" like ugh, silent swear words and feeling that things have "gone south" go on all the time and affect your next thoughts and choices. While many people believe that the mind rules, HeartMath says that it is our emotions that shape much of our thinking and, more often than not, determine choices and behaviours. Accumulated stress can actually prevent us from finding the creative solutions that we need to better deal with stress. Whether an irritation triggered by a relative or coworker, or low-grade anxiety triggered by current news events, HeartMath's research shows that stress compromises our cognitive abilities. That research notes that we cannot think as clearly or as creatively and we have a harder time making decisions. In the study by Maddock & Pariante (2001), when discussing the concept of stress, the authors noted that stress results when environmental demands exceed a person’s resources to meet those demands (Lazarus, & Folkman, 1984). They noted also that stress has various dimensions (Herbertt, & Cohen, 1993). It may be considered in terms of its duration (acute vs chronic; for example, laboratory stressor vs incurable disease); quantity (discrete events vs cumulative events; for example, bereavement vs daily hassles); and quality (interpersonal event vs non-interpersonal; for example, divorce vs earthquake). The individual’s perception of, and adaptation to, stressors is accompanied by physiological and behavioural changes. There is evidence to link stress with the onset of major depression and a poorer prognosis in cardiovascular disease and cancer. Chronic stress appears to result in suppression of the immune response, whereas immune activation and suppression have been associated with acute stress. Inflammatory cytokines, soluble mediators of the immune response, can result in symptoms of depression, Maddock & Pariante (2001). Psychological & psychosocial interventions and cancers While the relationship between psychosocial factors and the development of cancer has not been strongly established, research does demonstrate that addressing psychological stress as part of treatment programs for cancer patients does have benefits in facilitating adjustment and in improving survival. Recently 'Clinical practice guidelines for the psychosocial care of adults with cancer' were approved by the National Health and Medical Research Council and released as a National Breast Cancer and National Cancer Control Initiative 2003. It noted at page 14 that: Evidence is accumulating that psychological therapies improve emotional adjustment and social functioning, and reduce both treatment- and diseaserelated distress in patients with cancer. Meta-analyses of randomised controlled trials demonstrate the efficacy of both supportive and cognitive behavioural therapies in the treatment of depressive disorders in patients with cancer and the efficacy of both individual and group therapies. In a meta-analysis of 45 randomised controlled trials in patients with cancer, those receiving psychological therapies showed, on average, a significant improvement of 12% in measures of emotional adjustment, 10% in social functioning, 14% in treatment and disease-related symptoms, and 14% in overall improvement in their quality of life, compared with those not receiving psychological therapies. A meta-analysis of 116 intervention studies found that patients with cancer receiving psycho-educational or psychosocial interventions showed much lower rates of anxiety, depression, mood disorders, nausea, vomiting and pain, and significantly greater knowledge about disease and treatment, than the control group. Psycho-educational programs are defined as programs with both psychological (for example, supportive group therapy) and educational (for example, coping skills training, stress management, education about disease and treatment) components (italics added). Psychosocial intervention programs are defined as treatments that are intended to address psychological, social and some spiritual needs, while psychosocial support is the culturally-sensitive provision of psychological, social and spiritual care.(italics added). While a number of studies discussed below demonstrated that interventions to reduce psychological stress improve cancer survival, further research is required. Speigel, Bloom, Kraemer & Gottheil (1989) treated women with metastatic breast cancer by means of weekly group therapy. The intervention focused on encouraging a discussion of how to cope with cancer, and the expression of feelings about illness and its physical consequences. Relationships that developed amongst group members provided increased social support. A randomized study compared one year of the psychosocial treatment versus a control group. Both groups received routine oncology care. After 10 years of follow-up, the survival time of patients in the intervention group was almost double that of the controls; 36.6 months versus 18.9 months starting from the onset of the intervention. A further randomized prospective trial by Speidel et al (2007) however was unable to replicate these findings and concluded: The earlier finding that longer survival was associated with supportive-expressive group therapy was not replicated. Although it is possible that psychosocial effects on survival are relevant to a small sub sample of women who are more refractory to current hormonal treatments, further research is required to investigate subgroup differences. A group therapy intervention approach was utilised in the treatment of patients with malignant melanoma (Fawzy et al, 2003). The intervention was multifaceted, consisting of: (1) health education (eg melanoma, nutrition, exercise, sun exposure); (2) stress management (eg general stress information, personal stress awareness, relaxation techniques); (3) enhancement of coping skills (eg problem solving, general coping alternatives, theoretical and personal application of solutions); and (4) psychological support (from group members and staff). At six months follow-up the intervention group, compared to a randomly selected control group, exhibited lower levels of psychological distress (Fawzy et al, 1990a). Furthermore, after 5-6 years of follow-up the psychosocial intervention group had a lower rate of death and cancer recurrence than controls (Fawzy et al, 1993.) In a 10 year follow-up review the researchers noted that between the 5-6 year follow-up and the 10 year follow-up, the effects of the intervention had not entirely disappeared (Fawzy et al, 2003). In 2000, Stanton et al noted: Although not yet extended to cancer patients, experimental investigations provide the most convincing evidence to date that emotional processing and expression are related causally to positive outcomes. The study by Stanton et al (2000) tested the hypothesis of coping through emotional approach and its impacts on enhancing adjustment and health status for breast cancer patients. The authors noted evidence suggesting that coping through emotional approaches, i.e. coping through actively processing and expressing emotion, may enhance adjustment in cancer patients. In the Stanton et al (2000) study, the authors referred to previous randomized, controlled studies of psychological interventions, in which one intervention component was the facilitation of emotional expression. These studies provided evidence that in groups with cancers such as metastatic breast cancer and malignant melanoma such interventions can enhance psychological adjustment (Fawzy et al, 1990; Spiegel, Bloom, & Yalom, 1981), improve immune function (Fawzy et al, 1990), and perhaps promote longer survival (Fawzy et al, 1993; Spiegel, Bloom, Kraemer, & Gottheil, 1989). Further in the Stanton et al (2000) study, the authors referred to other studies of adjustment to cancer that indicated that coping through cognitive and behavioural avoidance is detrimental to adjustment (Carver et al, 1993; Friedman, Nelson, Baer, Lane, & Smith, 1990; Stanton, & Snider, 1993) and perhaps to health status (EppingJordan, Compas, & Howell, 1994; Jensen, 1987). DNA, genes, predisposition & cancer It is important to note that genes themselves do not cause disease – gene-based disorders are caused by mutations that make a gene function improperly. For example, when people say that someone has “the cystic fibrosis gene”, they are usually referring to a mutated version of the CFTR gene which causes the disease (Genomics Home reference – Your Guide to Understanding Genetic Conditions, US National Library of Medicine, National Institute of Health website). A mutation occurs when a DNA gene is damaged or changed in such a way as to alter the message carried by that gene. Once a gene is damaged or changed, the mRNA transcribed from that gene will now carry an altered message. Since genes are composed of DNA, nearly anything that can change the structural composition, sequence, physical integrity or length of a DNA molecule can cause mutations. Further, mutations can occur by what are described in the field as missense, nonsense, insertion, deletion, duplication, frameshift or repeated expansion. Cancers develop due to alterations (mutations) in genes that when working properly, promote normal, controlled cell growth. Only a small percentage of cancers involve inherited mutations that are passed from generation to generation (genetic). The majority of cancers can be attributed to acquired mutations. "Acquired" means that the mutations occur only in the tissue that is affected by cancer (for example, colon cancer cells), and are not passed to children. These changes occur at the cellular level after birth, as a result of environmental exposures (such as smoking, working with asbestos), lifestyle behaviours (such as eating poorly or not exercising), or chance alone. Mutations in a person's DNA accumulate over time. If mutations affect genes that control cell growth this may cause a cell to grow out of control, and to ultimately become a cancer cell (All About Cancers, description of genetics, Health Topics, University of Virginia Health System, website). How does our mind potentially modulate our genes? This question is explored in a book by E L Rossi (2003), The Psychobiology of Gene Expression: Neuroscience and Neurogenesis in Hypnosis and the Healing Art. Rossi explains that genes can be affected by thoughts and emotions. Ewin, D M, American Journal of Clinical Hypnosis, 2003 referring to an extract of the book, notes: ’Gene expression’ is the technical word for a gene that is activated into producing a particular protein. Some of these in turn, generate new neurons and connections in our brain. Since a thought or emotion can cause gene expression, there is now a true psycho-biology awaiting our understanding. We have millions of genes that can toggle ‘on’ or ‘off’ when we find the right switches in our thoughts and feelings. A Japanese study (Irie et al, 2001) using a sample of healthy adults, not only provided evidence of a stress-cancer linkage, but also suggested possible sex differences in the mechanisms of stress-related cancer initiation. This study noted that gene alterations, which are important in the pathogenesis of cancer, have scarcely been investigated in relation to psychosocial factors. It examined the relationship between psychosocial factors and cancer-predisposing gene alterations simultaneously in order to assess the stress-cancer linkage, particularly with respect to cancer initiation. Very limited issues, such as poorer repair of DNA damage, an increase of sister chromatid exchange and alterations in apoptosis, have been reported to be linked causatively with stress. Irie et al, (2001) undertook a study to investigate the relationships between the levels of 8-OH-dG in peripheral blood leukocytes and various psychosocial factors that may be associated with oxidative DNA damage. The study considered such psychosocial factors as emotions, stress-coping behaviours, social support, working conditions, and lifestyle factors in workers during usual stressful conditions. The relationships were examined adjusting for age, body mass index (BMI), cigarette smoking and alcohol drinking habits, because these factors have been reported to have associations with carcinogenicity and the formation of 8-OH-dG. In an article on current directions in cancer research, Antoni and Lutgendorf (2007) state that psychosocial factors such as stress, personality, and social support relate to differences in disease progression in cancer patients. Neuroendocrine substances associated with psychosocial factors may regulate immune responses to cancer as well as regulate the activity of oncogenic (cancer-causing) viruses, DNA-repair processes, and the expression in tumor cells of genes that may affect the tumor's growth and metastasis. Biobehavioral oncology research seeks to understand how these psychosocial factors, and interventions designed to modify them, become neurohormonal changes that alter cell signaling and tumor growth, viral oncogenesis, and immune responses. Antoni and Lutgendorf (2007) reviewed the empirical basis for psychosocial factors and biobehavioral processes in cancer progression and suggest future research. Lutgendorf et al, (2005) examined the relationships between distress, social support and natural killer (NK) cell activity in ovarian cancer patients in peripheral-blood mononuclear cells (PBMC), ascetic fluid and tumor-infiltrating lymphocytes (TIL). The researchers found that psychosocial stress was related to impaired immunity in cancer patients. However, the extent to which these relationships exist in immune cells in the tumor microenvironment in humans was not explored. In Lutgendorf et al (2005) research, patients awaiting surgery for a pelvic mass suspected of being ovarian cancer completed psychological questionnaires and gave a pre-surgical sample of peripheral blood. Samples of tumor and ascites were taken during surgery, lymphocytes were then isolated, and NK cytotoxicity and percentage were determined. The final sample, which was confirmed by surgical diagnosis, included 42 patients with epithelial ovarian cancer and 23 patients with benign masses. The results of the research by Lutgendorf et al (2005) noted that peripheral NK cell activity was significantly lower among ovarian cancer patients than in patients with benign masses. It noted, among ovarian cancer patients, NK cytotoxicity in TIL was significantly lower than in PBMC or ascitic fluid. Social support was related to higher NK cytotoxicity in PBMC and TIL, adjusting for stage. Distress was related to lower NK cytotoxicity in TIL. A multivariate model indicated independent associations of both distress and social support with NK cell activity in TIL. In other words, the research by Lutgendorf et al (2005) concluded that psychosocial factors, such as social support and distress, are associated with changes in the cellular immune response, not only in peripheral blood, but also at the tumor level. These relationships were more robust in TIL. These findings supported the presence of stress influences in the tumor microenvironment. An earlier study on vascular endothelial growth factor (VEGF) by Lutgendorf et al (2002) also contributes to our understanding of the biological basis for the link between social support and cancer prognosis. Pre-surgical levels of VEGF, a cytokine that stimulates tumor angiogenesis, were lower in patients with ovarian cancer who had higher levels of social well-being. Barclay (2002) observed that research is providing evidence that psychosocial factors can affect immunological responses of cancer patients. He discussed particularly one study conducted in Iowa, and noted from that research: Growing evidence has indicated that psychological factors, such as stress, depression, and social support, are able to modulate many of the immunologic activities relevant to patients with malignant disease. Of 24 women with ovarian carcinoma who were recruited at the pre-surgical clinic visit, those who reported higher levels of social well-being on the Functional Assessment of Cancer Therapy Quality of Life survey and the Profile of Mood States had lower levels of VEGF (P=.005). Specific perceptions linked to lower VEGF levels were greater support from friends and neighbours (P=.005) and less distance from friends (P=.04). Although depression as a whole was not related to VEGF levels, feelings of helplessness (P=.03) or worthlessness (P=.08) predicted higher VEGF levels. In light of study limitations including the cross-sectional nature of the data and use of a quality-of-life instrument measuring only limited aspects of social support, they recommend further research before drawing any causal inferences. They (sic the researchers) suggested that these findings suggest a novel mechanism by which bio-behavioural factors may be associated with the progression of ovarian carcinoma. They concluded that understanding the mechanisms of such interactions and the type and magnitude of their potential effects is an important goal of future research. In a more recent study by Sharma, Sharp, Greenman, Monson, & Walker (2007), the authors questioned if VEGF was related to psychosocial factors in patients with colorectal cancer. They reported that: Various psychosocial factors, particularly cancer-related concerns and depression, appear to be related to pre-operative and post-operative VEGF level in patients with colorectal cancer. Future prognostic studies involving VEGF should assess psychosocial variables and include these in a multivariate analysis of outcomes. In another link to the capacity of our immune system to have a positive effect on cancer outcomes Koebel et al (2007) presented their research findings that suggested “when cancer cannot be killed, it may be possible to find ways to use the immune system to contain it”. Co–author Prof Mark Smyth, Head of the Peter MacCallum Cancer Immunology Program in Melbourne, suggested that the next step would be to mobilise the immune system to suppress cancer and prevent it from spreading (Kelly, 2007). In research of another possible predisposition gene marker, Wu et al (2003) provided support to their hypothesis that telomere dysfunction impairs chromosomal stability and is associated with an increased risk of various cancers. These results (using two different methods to measure telomere length) demonstrated that telomere length was statistically significantly shorter in lymphocytes from case patients with head and neck cancer, bladder, lung, or renal cell carcinoma than in control subjects. It also provided evidence of an increasing risk for head and neck, lung, and renal cancer associated with progressively shorter telomeres, indicating that telomere dysfunction may be a risk factor for cancer at these sites and possibly for cancer in general. A stress hypothesis, including the epigenetic alterations, was investigated in a study that reported sustained stress environment (SSE) investigations, noted in the table below, by different natures of stress impacts (Karpinets, & Foy, 2005). The table below summarizes the links between epigenetic alterations, the relationships with the nature of stress (environmental) and the tissues and organisms reviewed. Epigenetic alterations induced by SSE in mammalian cells Epigenetic alterations Nature of stress Tissue/organisms Ref. Hypermethylation of tumor suppressor genes (p16, APC) and decrease in the mean methylation index Tobacco smoke exposure Lung tissue of long-time smokers 59 Hypermethylation of tumor suppressor gene p16 Exposure with cadmium (potent carcinogen) Cell culture (BALB/c-3T3 cells) 60 Hypermethylation and transcriptional silencing of p16 and p53 Exposure with dioxin (an Primary human ubiquitous environmental keratinocytes contaminant and a highly potent carcinogen) 61 Hypomethylation including rafgene Phenobarbital's exposure Rodent liver tissue 62 Upregulation and hypomethylation of c-myc and c-jun Exposure with carcinogens (arsenite, dichloroacetic acid and trichloroacetic acid) Variety of tissues, including 63, 64 the liver Hypomethylation of the genome Exposure with cadmium Rat liver cells (TRL1215) 65 Decondensation of the heterochromatin Exposure with nickel Chinese hamster embryo cells 66, 67 Dose-dependent hypomethylation Gamma radiation Four non-malignant cultured cell lines 68 Dose-dependent hypomethylation Ultraviolet radiation (UVB 280–340 nm) Rat liver 69 Induction of Alu elements (short interspersed elements) Genotoxic stress induced by a variety of DNA damaging agents Mouse cells 70 Induction of long interspersed nuclear element-1 (LINE-1) Endogenous oxidative stress Glucose 6-phosphate dehydrogenase deficient mice 71 Induction of VL30 elements (a Anoxia (may accompany multigene family within the class of wound healing) retroviruses and retrotransposons) Rat fibroblasts 72 Hypermethylation of mismatch repair genes and microsatellite instability Chronic inflammation (chronic ulcerative colitis) Non-neoplastic mucosa 73 Epigenetic silencing of imprinted genes that are usually induced by Proliferation under stress (cell culturing) Primary mouse embryonic fibroblasts 74 tumorigenesis Progressive aberrant methylation of SV40 virus infection protooncogenes (RASSF1A, HPP1, DcR1, TMS1, CRBP1, HIC-1 and RRAD) methylated in malignant mesothelioma Human mesothelial cells Hypermethylation of p16 promoter Hepatitis B virus and hepatitis C virus infection in liver with chronic inflammation Liver tissue specimens of human hepatocellular carcinoma with or without hepatitis virus infection Epstein–Barr virusassociated gastric carcinoma Epstein–Barr virusassociated and negative gastric carcinoma Specific high-density methylation of cyclin-dependent kinase inhibitors p14 and p16 75 76 77 NB: the references are to those in the original article Source: Karpinets, & Foy (2005) Part of the commentary to this table noted that tumorigenesis is considered a process of the adaptation of mammalian cells to SSE (sustained stress environment) by means of EA (epigenetic alterations) of the genome, subsequent mutations matched to EA and natural selection of originated mutant cells via apoptosis (Figure 1, replicated schematic below in this article). The process of adaptation to SSE involves the emergence of senescent epigenetically reprogrammed (ER) cells with specific tumor related EA in the genome. The EA prime the cells for error prone replications and provide epigenetic tags in the genome for beneficial mutations to arise. The authors (Karpinets, & Foy, 2005) further hypothesized that tumor related EA occur before mutations and reprogram the genome for their origin. The initiation event for these EA is long-term exposure of cell tissue to SSE that induces continuing replication of some cells in the tissue. Persistent proliferative and stressrelated survival signals in the environment induce in these proliferating cells a stable activation of biological processes related to promotion of replication and stress response. On the other hand, processes related to inhibition of proliferation, activation of cell-cycle arrest and apoptosis, and DNA repair pathways will be constantly suppressed in these cells. Source: Karpinets, & Foy (2005) Conclusion The evidence presented demonstrates some relationships across psychological, psychosocial, environmental and gene pathways and cancer. While not determinative, the evidence provides opportunities for further high quality research in what is a psychogenomic structure. Research streams that form part of psycho-genomics include cancer, psychology, emotional expression & processing, psychosocial, environmental, physiology, DNA genes and genomics. Power Thinking Health Council aims to undertake that research and will: identify gene expression and gene mutation marker differentials between cancer and non-cancer population; undertake a study over several years looking for blood markers of cellular dysfunctions which predispose to cancer, i.e. a step before the current screening phase, and identify psychological/psychosocial intervention affects on those blood markers over time in order to treat cancers to increase survivorship and prevent initiation of cancers. Bibliography Antoni, M., & Lutgendorf, S. (2007). Psychosocial Factors and Disease Progression in Cancer Current Directions. Psychological Science, 16(1),42-46. doi:10.1111/j.1467-8721.2007.00472. http://www.blackwell-synergy.com/doi/abs/10.1111/j.1467-8721.2007.00472.x?journalCode=cdir Barclay, L. (2002). VEGF May Explain Link Between Social Support, Cancer Prognosis. Cancer, 95, 808-815. http://www.medscape.com/viewarticle/440058_print [Also see 2005 report National Cancer Institute, Nations investment in Cancer Research, Scientists Explore Effects of Biobehavioral Factors on Ovarian Cancer. http://plan2005.cancer.gov/highlights.html#5. Also Naushen, B.; Gidron, Y.; Peveler, R.; Bruce L., & Verrill, C. (2006). The relationship between social support and disease markers in colorectal cancer. Poster session presented at the 8th World Congress of Psycho-Oncology, Venice, Italy.]. Breast Cancer at the ABC Toowong Queensland: Third Progress Report from the Independent Review and Scientific Investigation Panel, 21 December 2006. http://mp3.news.com.au/bcm/1221ABC/ABC.pdf Butow, P.; Hiller, J.; Price, M.; Thackway, S.; Kricker, A., & Tennant, C. (2000). Epidemiological evidence for a relationship between life events, coping style, and personality factors in the development of breast cancer. Journal of Psychosomatic Research, 49, 169181. Fawzy, I.; Canada, A., & Fawzy, N. (2003). Malignant melanoma: effects of a brief, structured psychiatric intervention on survival and recurrence at 10-year follow-up. Arch Gen Psychiatry, 60, 100-103. http://archpsyc.ama-assn.org/cgi/content/full/60/1/100 Garssen, B. (2004). Psychological factors and cancer development: evidence after 30 years of research. Clinical Psychology Review, 24(3), 315-338. See also HeartMath, Institute of, website: Are we resigned to stress – HeartMath stress experts say we can significantly reduce our stress by understanding how our emotions work. http://www.heartmath.com.au/company/proom/pr/resigned_to_stress.html Irie, M.; Asami, S.; Nagata, S.; Ikeda, M.; Miyata, M., & Kasai, H. (2001). Psychosocial Factors as a Potential Trigger of Oxidative DNA Damage in Human Leukocytes. Japan J. Cancer Res., 92, 367-376. Cancer Science, 93(3), 367-376. http://www.blackwellsynergy.com/doi/abs/10.1111/j.1349-7006.2001.tb01104.x Karpinets, T., & Foy, B. (2005). Tumorigenesis: the adaptation of mammalian cells to sustained stress environment by epigenetic alterations and succeeding matched mutations. Carcinogenesis, 26(8), 1323-1334. Originally published online on March 31, 2005: Carcinogenesis, 26(8). doi:10.1093/carcin/bgi079. http://carcin.oxfordjournals.org/cgi/content/abstract/26/8/1323 Kelly, J., Medical research hailed in cancer fight, Herald Sun, 20 November 2007: http://www.news.com.au/heraldsun/story/0,21985,22787451-2862,00.html Koebel, C.; Vermi, W.; Swann, J.; Zerafa, N.; Rodig, S.; Old, L.; Smyth, M., & Schreiber, R. (2007). Adaptive immunity maintains occult in an equilibrium state. Nature, 450, 903-907. Lutgendorf, S.; Johnsen, E.; Cooper, B.; Anderson, B.; Sorosky, J.; Buller, R., & Sood, A. (2002). Vascular endothelial growth factor and social support in patients with ovarian carcinoma. Cancer, 95(4),808-815. http://www3.interscience.wiley.com/cgibin/abstract/97515913/ABSTRACT?CRETRY=1&SRETRY=0 Lutgendorf, S.; Sood, A.; Anderson, B.; McGinn, S.; Maiseri, H.; Dao, M.; Sorosky, J.; De Geest, K.; Ritchie, J., & Lubaroff, D. (2005). Social support, psychological distress, and natural killer cell activity in ovarian cancer. Journal of Clinical Oncology, 23(28), 7105-7113. http://jco.ascopubs.org/cgi/reprint/23/28/7105 Maddock, C., & Pariante, C. (2001). How does stress affect you? An overview of stress, immunity, depression and disease. Epidemiologia e Psichiatria Sociale, 10(3), 82-92. Melhuish, A., Executive Health, London Business Books, with extracts from Andy Ellis, Ruskin College, Oxford, UK, The Stress Management Society website. http://www.stress.org.uk/4617/9903.html?*session*id*key*=*session*id*val* National Breast Cancer Centre and National Cancer Control Initiative (2003). Clinical practice guidelines for the psychosocial care of adults with cancer. National Breast Cancer Centre, Camperdown, NSW . http://www.nhmrc.gov.au/publications/synopses/_files/cp90.pdf National Institute of Health (2008). How can gene mutations affect health and development? Genomics Home reference: your guide to understanding genetic conditions, US National Library of Medicine, published at: http://ghr.nlm.nih.gov/handbook/mutationsanddisorders/mutationscausedisease Rossi, E. (2002). The Psychobiology of Gene Expression: Neuroscience and Neurogenesis in Hypnosis and the Healing Arts. New York: W.W. Norton & Co. In D. Ewin (2003). The Psychobiology of Gene Expression: Neuroscience and Neurogenesis in Hypnosis and the Healing Arts: book review. American Journal of Clinical Hypnosis, January 2003, published at: http://findarticles.com/p/articles/mi_qa4087/is_200301/ai_n9197346 Spiegel, D.; Bloom, J.; Kraemer, H., & Gottheil, E. (1989). Effect of psychosocial treatment on survival of patients with metastatic breast cancer. Lancet. 14(2), 888-891. http://www.ncbi.nlm.nih.gov/pubmed/2571815 Spiegel, D.; Butler, L.; Giese-Davis, J.; Koopman, C.; Miller, E.; DiMiceli, S.; Classen, C.; Fobair, P.; Carlson, R., & Kraemer, H. (2007). Effects of supportive-expressive group therapy on survival of patients with metastatic breast cancer: a randomized prospective trial. Cancer. 110(5), 1130-1138. http://www.ncbi.nlm.nih.gov/pubmed/17647221?ordinalpos=1&itool=EntrezSystem2.PEntrez.Pubmed.P ubmed_ResultsPanel.Pubmed_RVAbstractPlus Sharma, A.; Greenman, J.; Sharp, D.; Monson, J., & Walker, L. (2006). Is VEGF related to psychosocial factors in patients with colorectal cancer. Journal of Surgical Research, 130, 321. See also National Cancer Research Institute Cancer Conference UK, 2006 Poster Abstract. http://www.ncri.org.uk/ncriconference/abstract/pdf/pdfs/NCRI2006_0405.pdf Stanton, A.; Danoff-Burg, S.; Cameron, C.; Bishop, M,; Collins, C.; Kirk, S., & Sworowski, L. (2000). Emotionally Expressive Coping Predicts Psychological and Physical Adjustment to Breast Cancer. Journal of Consulting and Clinical Psychology, 68(5), 875-882. http://www.apa.org/journals/features/ccp685875.pdf University of Virginia Health System website. All about Cancers: description of genetics. https://www.healthsystem.virginia.edu/UVAHealth/hub_cancer/gendesc.cfm White, V.; English, D.; Coates, H.; Lagerlund, M.; Borland, R., & Giles G. (2007). Is Cancer Risk Associated With Anger Control and Negative Affect? Findings from a Prospective Cohort Study. Psychosomatic Medicine, 69, 667-674. Wu, X.; Amos, C.; Zhu, Y.; Zhao, H.; Grossman, B.; Shay, J.; Luo, S.; Hong, W., & Spitz, M. (2003). Telomere Dysfunction: A Potential Cancer Predisposition Factor. Journal of the National Cancer Institute, 95(16), 121-1218. http://jnci.oxfordjournals.org/cgi/reprint/jnci;95/16/1211.pdf