personal genetics education project Social, Legal and Ethical Issues
advertisement

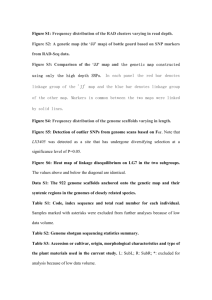
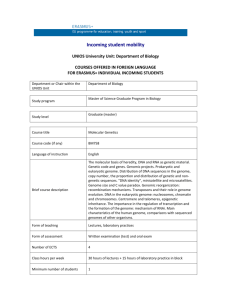
personal genetics education project Social, Legal and Ethical Issues in Personal Genetics Title: What is Personal Genetics? Aim: How might new advances in personal genetics impact our lives and medical decisions? Time: 1-2 days Guiding Questions: ● How would you decide whether or not to get your genome sequenced? ● How might genome sequencing change health care? ● What are the benefits and risks to you and other stakeholders? Learning objectives: After completing this lesson, students will be able to: ● Grasp the rapid rate at which technology is developing ● Define what a personal genome sequence is and how it differs from typical genetic testing ● Analyze why people would or would not want to know more about their genome Materials: Projector or Smartboard, laptop, paper, tape, handouts (at the end of lesson plan) Common Core Standards: RH.11-12.1. Cite specific textual evidence to support analysis of primary and secondary sources, connecting insights gained from specific details to an understanding of the text as a whole. RST.11-12.2. Determine the central ideas or conclusions of a text; summarize complex concepts, processes, or information presented in a text by paraphrasing them in simpler but still accurate terms. RST.11-12.7. Integrate and evaluate multiple sources of information presented in diverse formats and media (e.g., quantitative data, video, multimedia) in order to address a question or solve a problem. www.pgEd.org 1 Before the lesson: If you have not done a full unit on genetics (particularly if this lesson is used in a health, ethics, or non-science class), explain to students that many diseases are passed down from parent to child through their genes. On their own, students can learn more about heredity, genes and traits at University of Utah’s award-winning site: http://learn.genetics.utah.edu/. Click on the “Heredity and Traits” link in the box on the left under Basics. High school and college age students are likely to become independent health care consumers at about the time that personal genome sequencing becomes an affordable and accessible option for many people. This lesson introduces them to the recent advances in genetics, genetic testing, and personal genome sequencing, and presents some of the decisions and ethical challenges an individual may face regarding the use of this technology. It also highlights some of the likely benefits of personal genomes, such as gaining the ability to act on one’s genetic risks, tailoring medicines and interventions, and becoming more active and engaged healthcare consumers. Via class discussion and the readings, students will be able to generate ideas about the possible risks and benefits. There are many reasons people want to get their genome sequenced. Genome sequencing analyzes all of your genes, as opposed to a traditional genetic test that targets a single gene or small cluster of genes. Some people decide to get their genome sequenced so they can take steps to try to prevent a disease for which they are at risk (heart disease, diabetes), or to find out if certain drugs are likely to be effective based on genetic factors. People who learn that they will likely develop a disease with no cure might opt to buy long-term disability insurance, write a will, name a healthcare proxy, or take other steps to plan for the future. Some may decide to become activists, educators and start or participate in research studies. Others might decide to not have biological children to avoid passing on a genetic disorder, or use advanced reproductive technology to screen IVFcreated embryos in an effort to choose an embryo free of the genetic disease they are seeking to avoid. To give students a sense of the “big picture” in genetics, we recommend Mary Carmichael’s excellent series she wrote for Newsweek in 2010. If you are going to read only once piece from the six- part series, read the first one! “DNA Dilemma: Should I take a genetic test?” Mary Carmichael, Newsweek. Do now: (7 min) Students should answer questions individually or discuss with a partner. www.pgEd.org 2 1.What are the potential benefits to knowing more about you genetic predisposition (chance of developing) to disease? 2.What are the possible negatives to knowing? Discuss student answers after they have finished. Activity: 1. Interactive Slideshow (15 - 20 min) We have created a PowerPoint slideshow (located under the lesson plan link here: http://www.pged.org/lesson-plans/) that explores what types of information people can learn from genome sequencing, the hopes and limits of sequencing, and how this information may impact us. The notes that accompany the slides are included in this lesson. One important point to make to your students is that genetics can make predictions about your health risks and other traits, but does not tell the future. The intricate relationship between genetics and environment is key to our understanding of behavior and health. You may want students to take notes to help evaluate their understanding, particularly if you will be using additional lesson plans and students will later participate in a debate and/or writing activity. One excellent method for note-taking is Two-Column Note Taking. A sample graphic organizer is at the end of the lesson plan. Notes for slideshow: Slide 3: New DNA sequencing technologies are quickly making it faster and less expensive to learn about one’s DNA. The cost of finding out your entire DNA sequence is anticipated to decrease so quickly that, within ten years, your physician might request your genome be sequenced as part of routine blood-work, possibly covered by health insurance. Genetic tests are directly available to consumers – called direct-to-consumer (DTC) testing. Companies sell kits on-line consisting of a tube for saliva, and directs customers to spit into the tube and mail the tube back to the company. The companies then analyze the DNA (which look at pieces of the genome rather than the entire genome) in the saliva and send a report of the traits that might be predicted by your DNA. Our DNA can reveal important information about our health, behavior and other traits. However, it is important to remember that we are much more than our genetic information. Learning about our DNA is highly personal, but also raises many questions about how we as a society are going to handle the accessibility of genetic information. For example, if you learn about your risk for Alzheimer‘s disease, this may raise concerns for your mother, who might not want to know anything about her Alzheimer’s status. Might easy www.pgEd.org 3 access to genetic predispositions affect dating relationships? Should insurance companies be able to know information about your DNA? These are just a few of the issues that your class will discuss. Slide 4: The generation that is now in middle and high school likely will be more directly impacted by the increase in genetic information than any previous generation. Doctors and scientists think of the “$1000 genome” as an important milestone, because at that cost (or less) it will be a similar cost to other routine medical tests like MRIs, and may become a common tool to help diagnose disease and indicate treatment options. Note: Slides 5-9 offer a very brief overview of some of the ways that genetic testing or genome sequencing are being used and impacting real people. Slide 5: Genome sequencing has already had real-world impacts on patients, including twins Alexis and Noah Beery. The twins exhibited a number of developmental delays and were diagnosed with cerebral palsy at the age of two. However, their mother, Retta, never felt that this diagnosis was correct, particularly since their symptoms worsened over the course of the day. Through her own research and advocacy, the twins were diagnosed with a genetic disorder called dopa-responsive dystonia and began taking a medication that seemed to successfully treat the condition. However, some symptoms persisted and escalated, particularly for Alexa, including serious breathing problems. The Beerys had the twins' genomes sequenced, leading to the identification of a mutation in the SPR gene which, when disrupted, causes deficiencies in two neurotransmitters, called dopamine and serotonin. Upon treatment to address both genetic disorders, the twins’ symptoms quickly improved, permitting them to resume full, active lives. Slide 6: In May 2013 actress Angelina Jolie revealed that she had undergone a double mastectomy because she carried a mutation in the BRCA1 gene that greatly increased her risk of breast and ovarian cancer. According to Jolie’s op-ed in the New York Times, her “chances of developing breast cancer have dropped from 87 percent to under 5 percent.” This example is a great way to engage students with a real-life example of a well-known person making a major medical decision based on genetic information. My Medical Choice in The New York Times Slide 7: Some people use a technique called pre-implantation genetic diagnosis in conjunction with in-vitro fertilization (IVF) to avoid deadly childhood diseases. IVF is a process used to help people with fertility issues conceive. Usually, women are given hormone injections to produce multiple eggs, which are then extracted and combined in a petri dish with sperm. One or (usually) more embryos are then implanted in the woman’s uterus. www.pgEd.org 4 Pre-implantation genetic diagnosis (PGD) is used during IVF when parents have a high likelihood of passing on a serious or deadly genetic condition to a child. A single cell is removed from an 8-cell embryo and tested for a specific condition. Embryos that are free of the condition (if any) are then considered for implantation into the woman’s uterus. This image is a cell being removed from an 8 cell, 3-day-old embryo. Studies have shown that the removal of one cell at this stage does not seem to impact the development of the embryo. This technique raises ethical issues for many people; some believe that people should not interfere with the process of conception. Others raise concerns that parents can use this technique to screen for adult-onset disease or non-medical issues (i.e. eye color, sex, having severely crossed eyes) will lead to “designer babies” and that parents and doctors should not have the ability to choose a child’s traits. Slide 8: This picture shows a child getting the inside of his cheek swabbed for DNA that will be sent to a company that will test for a specific version of the ACTN3 gene, to see if he might excel at certain sports (endurance vs. sprinting, like soccer vs. hockey). There is a lot of controversy about how useful this test is, and if it is right for parents to test small children for this rather than, for example, encourage your child to try different sports and seeing what she or he likes best. Slide 9: DNA tests can be used to help people learn about their ancestry, particularly when that history is unknown for various reasons. Because of this history of slavery, many people of African ancestry do not know what area of Africa their ancestors were from. Other people may not know any ancestry information (or medical family history) if they are adopted. DNA testing can fill in these gaps and allow some people to feel more connected to a past they were previously unaware of. Slides 10 and 11: Technological advances can fuel societal change, whether it be in computers or DNA sequencers. In 1945, the US military completed the ENIAC, the first electronic general-purpose computer. The decimal-based machine used 18,000 vacuum tubes, weighed 30 tons and took up 1,800 square feet. Today, all 1,800 square feet of that machinery fits on the head of a pin. (http://www.pcmag.com/encyclopedia/term/42630/eniac) An iPad is clearly smaller, lighter and faster than the ENIAC, with countless more features. The Oxford Nanopore MinIon is a DNA sequencer that fits in one’s hand, and is a USB drive that can be plugged into a computer and read the DNA sample that has been previously loaded into it. According to its makers, it will be able to sequence up to 150 million base pairs in six hours and will cost under $1000. www.pgEd.org 5 Slide 12: Because of major technological advances, the cost of sequencing a human genome has fallen rapidly. Within the next 3-5 years, the cost of sequencing a human genome is estimated to be under $1,000 and will take only hours or days to complete. Perhaps reading human genomes will be as routine as blood tests and easy enough to be carried out in your doctor’s office. Graph is available at http://www.genome.gov/sequencingcosts/. Slide 13: An example of a director-to-consumer genetic testing kit available on the Internet. 23andMe sells kits that consumers can order online, spit into a tube (a large enough amount that a person wouldn’t be able to obtain someone else’s saliva without their knowledge), and then send back for analysis. Customers can obtain results about their risk for serious diseases such as type-2 diabetes, Parkinson’s Disease or age-related eye disease; whether they may pass on genetic variants to a child; and interesting but not particularly consequential information, such as whether or not they have a genetic predisposition to think that cilantro tastes like soap. Debate continues about whether tests such as these should be available to people without having to talk to a doctor or genetic counselor to ensure that people understand their risks and the results of the test. Others argue these are paternalistic concerns that consumers can assess for themselves. Slide 14: 23andMe tests for a very broad array of genetic variants, which assess a person’s risk for serious diseases or conditions, including macular degeneration (which can lead to blindness), Parkinson’s Disease, diabetes, and many types of cancer. This may cause some people to opt for earlier or more frequent medical screenings or adopt lifestyle changes to avoid a specific disease. Slide 15: The potential benefit of genetics in medicine is enormous. Nevertheless, there are challenges as well. Here we explore some of the challenges (this is for teacher information, which can be condensed for students): 1. Clinical utility: First, scientists are still learning how to interpret genomes – research is progressing quickly, but much remains to be learned. This is evident from the differences in the predictions that different DTC companies make with respect to disease risk. It is also evident in the predictions that change and evolve over time as research furthers our understanding. Individuals should therefore take care when they consider disease risk predictions and, furthermore, have the interpretation of their genome reassessed periodically. Second, often there is no clear medical action that can be taken based on genomic information. Already, there are a few remarkable stories, such as that of the Beery twins, where genome sequencing has brought both a diagnosis and an effective treatment. In other cases, genome sequencing may bring a diagnosis without a cure or no www.pgEd.org 6 diagnosis at all. The hope is that advancements in science and medicine will continue to improve the clinical utility of personal genomes. 2. Familial impact: Do you want to know if you have increased risk for a disease such as Alzheimer’s, which has no effective treatment or cure? For some individuals, the answer is “yes,” as they feel that knowledge is power and knowing whether they are predisposed to a disease will affect how they choose to live and plan for their future. Others would prefer not to know because, once you learn about your genetic risk, it is impossible to go back and “unknow” this information. Therefore, it is important to consider this issue before learning about your genome, to decide if there are limits to what you want to learn. It is also important to consider how our genetic information might affect our family members. For example, imagine a woman whose mother’s family has a history of breast cancer. If she learns that she carries a BRCA1 variant that puts her at increased risk, there is a good chance that her mother is at increased risk as well. Should she ask her mother’s permission before getting tested? Should she ask her husband’s opinion, because knowing whether she carries the BRCA1 variant has implications for their long-term planning and for their children? 3. The influence of factors outside of our genome: Personal experiences and environmental factors also affect our health and behavior. For example, it is known that there is a significant genetic component to addiction. We should not assume that these individuals are all addicts, nor should these individuals feel trapped by their genetics. Education and discussion are important to avoid this over-simplified thinking. 4. Discrimination: Some people believe that genetic information, if made public, could be used to harm them in some way. The U.S. Congress passed the Genetic Information Non-Discrimination Act (GINA) in 2008, which states that people cannot be discriminated against with regard to employment or health insurance based on genetic information. However, this law does not protect individuals against discrimination with respect to other insurance coverage, including disability, long-term care and life insurance, which use family history to evaluate applicants. 5. Equality of accessibility: Finally, how can we ensure that everyone who wants it can access his or her genetic information? There is general agreement that everyone, regardless of socioeconomic status, should know about the possible benefits and risks of genome sequencing, but it will take time to implement a comprehensive educational program. Can we ensure equal access? Will insurance companies pay for genome sequencing? Will people enroll in research studies? Will prices continue to fall? Ensuring the accessibility of genome sequencing to all who are interested is a growing issue as personal genetics plays an increasingly important role in healthcare. 2. Four Corners Activity (15 - 25 min, depending on depth of discussion) www.pgEd.org 7 Students will hear several statements, and move to labeled corners of the room based on whether they agree or disagree with each statement, and then discuss their opinions. Step one: Preparation Label the four corners of the room before students enter with signs reading: strongly agree, agree, disagree, and strongly disagree. You could also do a straight line across the room with students placing themselves on the continuum between strongly agree and strongly disagree; the best set up likely depends on your classroom. Tell students: The new advances in genetics and genome sequencing offer great hope for medicine and health; at the same time, there are risks and questions for consumers. The statements below offer students a chance to express their opinion and discuss some of the issues with their classmates. Step two: Introduce Statements: Read each statement and have students move to the corner of the room depending on whether they strongly agree, agree, disagree, or strongly disagree (statements are in the slideshow). After they move to the corner, have them discuss in their groups why they agree/disagree. Once students are in their places, ask for volunteers to explain their position; they should cite information from the article that supports their position. Encourage students to switch corners if someone presents an idea that causes them to change their opinion. After a representative from each corner has defended his or her position, you can allow students to question each other’s evidence and ideas. Before beginning the discussion, remind students about norms for having a respectful, open discussion of ideas. Note: If you have longer class periods and/or will use this as a pre-writing activity for either an essay or debate, you can distribute statements and give students the opportunity to respond to them in writing before discussing. Statements: ● People should get counseling from a doctor or genetic counselor when they get genetic testing because they won’t be able to handle the information otherwise. ● People should have the right to learn whatever they want to about their DNA because it is their own body. www.pgEd.org 8 Note for teacher: The first two statements show conflicting viewpoints about genetic testing, particularly in regard to direct-to-consumer (DTC) testing. New York State banned the sale of DTC tests, and the American Medical Association recommended that the Food and Drug Administration ban the tests, because they think people need the results interpreted by a qualified doctor. The other side typically finds this argument paternalistic and believes that individuals absolutely have the right to learn about their DNA. You can read more at http://www.ama-assn.org/ama1/pub/upload/mm/399/consumergenetic-testing-letter.pdf and http://www.wired.com/wiredscience/2011/02/american-medicalassociation-you-cant-look-at-your-genome-without-our-supervision/. ● I would only want to find out my likelihood of developing a disease if there are ways to prevent or treat it. Note for teacher: Even in the absence of medical interventions, some people want this information to guide lifestyle changes, financial planning, or may be spurred into advocacy or research studies. Other people feel that concerns about discrimination and emotional impact override the benefits of having this information. However, research has shown that learning about heightened genetic risk to disease does not do long-term harm: Learning of Risk of Alzheimer’s Seems to Do No Harm ● Parents undergoing in-vitro fertilization should have the option to screen embryos for serious disease. Note: Some parents who know they carry a genetic variant that would likely cause serious disease or death in a child opt to get special testing, called pre-implantation genetic diagnosis (PGD), to test embryos for that disease. They then would choose to implant only embryos that are free from the disease. Some people see this as a great advance that can eliminate serious and deadly diseases, while others believe that any testing of embryos is unethical because conception should not be interfered with. ● Parents should be able to choose a child’s traits for non-medical issues such as eye color, sex, and athletic ability. Note: Many clinics that offer PGD for medical reasons also allow parents to select the sex of the child for social reasons. It is possible to test for cosmetic traits such as eye or hair color, though most clinics do not provide that. With the ability of geneticists to sequence fetal www.pgEd.org 9 genomes, however, many people think it is possible that people will be able to test for athletic ability, perfect pitch (the ability to identify or recreate a musical note without a reference pitch), height, etc. ● Some people are better suited for certain jobs based on their DNA. The Genetic Information Non-Discrimination Act (GINA) was passed by Congress in 2008 prohibits employers from basing hiring or firing decisions based on genetic information. This statement gets students thinking about the practicality of this idea and raises some interesting questions: Can everyone be a professional athlete? Truck driver? Professor? Soldier? Although most people agree people shouldn’t be discriminated against based on genetics, this question helps students think about the role genetics may play what career choices people make. ● Parents should be able to find out whatever they would like about their children’s DNA before they turn 18. Note: This statement is intentionally broad to encourage students to consider how much information could be available to parents through genome sequencing. There is a big debate about how much parents should find out about their offspring’s DNA, either prenatally or after birth. While genome sequencing can help to predict, diagnose or treat certain diseases, it may uncover genetic risks for disease later in life or other information that might affect how a child is raised. Many people are concerned about the availability of this information before the child is able to give informed consent. Should testing be done that only looks for a specific subset of genetic risks? Or, if genome sequencing is performed, should only specific types of information be provided to parents? Is it ethical for parents to test for athletic ability before the child can understand what this means, and what kind of pressures might that create on the child? The American College of Medical Genetics and Genomics released new guidelines in March 2013 regarding the reporting of incidental, or secondary, findings when performing genome sequencing: “The guidelines recommend that doctors tell patients (and the families of children or impaired adult patients) if their genome analysis reveals the presence of one of several types of genomic variants in 50 or so genes that have been strongly associated with about two dozen diseases. A key factor in selecting these genes and diseases was that the disorder is serious and that there are practical things that the patient and doctor can do to mitigate the associated risks. If genome www.pgEd.org 10 sequencing reveals any of these, the standard of care will now be for the laboratory to return the information to the doctor and for the doctor to then tell the patient, prompting appropriate follow-up care to keep the patient healthy.” (http://www.genome.gov/27553717) ● I would want to know if someone I was dating had a genetic condition that would likely cause a serious disease. Note: The goal of this statement is to encourage students to think about how the availability of genetic information will impact our social perceptions and how private or accessible they want their information to be. We’ve included the statements on the PowerPoint. This helps students understand the statement and prevents the teacher from having to read it several times. Step three: Debrief You can debrief the lesson as a whole class or individually. Discuss or have students write about how the activity changed or reinforced their original ideas. To clarify ideas shared during the discussion, chart the main arguments on the board as a whole-class activity. Homework: Have students answer questions below. 1. Explain some of the reasons people choose to get genetic analysis. What are some of the benefits of doing so? What are some of the possible disadvantages of doing so? Explain. 2. Do you think people should be able to get genetic testing directly from companies, instead of going through their doctors? Why or why not? 3. Would you consider getting genetic testing to learn more about your health? Why or why not? If yes, under what circumstances might you consider it? Teacher resources for further exploration: 1. Amy Harmon’s “DNA Age” series in the New York Times for news, analysis and video clips. While some of the science has changed, the issues Harmon examines are still timely. http://topics.nytimes.com/topics/news/national/series/dnaage/index.html www.pgEd.org 11 2. The Hastings Center is an independent, nonpartisan, and nonprofit bioethics research institute with many resources and articles about ethics and genetic and genomic testing: http://www.thehastingscenter.org/Issues/Default.aspx?v=246&gclid=CMuUl OD_orgCFcad4AoddHEA2w www.pgEd.org 12 Name__________________________________ Key Ideas: What ideas are most important to remember? What new terms or concepts have been introduced? Date__________ Response: What questions does this information raise for you? What other ideas, events or texts does this information remind you of? Why do you think this information is important? How does this information connect to your own lives? What do you think of these ideas? www.pgEd.org 13