SCHISTOPROJECT(3)
advertisement
")
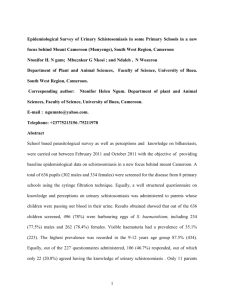
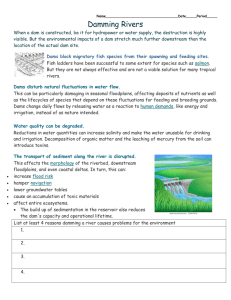
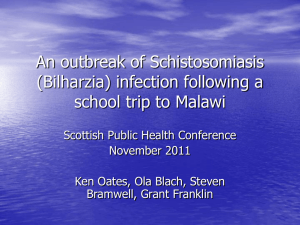
Leah Machen Kirsten Rogers Parasites and Pestilence Proposal Mapping the Key to Prevention Spotlighting the link between Dam Construction and Schistosomiasis Outbreak Introduction: Since 1970, there has been an upsurge in dam construction in Nigeria that has been strongly correlated to schistosomiasis outbreak in endemic states. Although there are several ways to combat the increased incidence of schistosomiasis associated with water development projects including the administration of praziquantel to residents of endemic areas, molluscides for intermediate host snail control, or the introduction of a competitor species to reduce the snail population, a preventative intervention must also be implemented to promote the awareness of the adverse health effects caused by water development projects so that appropriate action can be taken. Specific Aims: This project will investigate the correlation between dam construction and schistosomiasis prevalence in Nigeria with the goal of constructing a color-coded nation-wide map. The map consists of bulleted locations of all dams within the country along with colorcoded indicators of schistosomiasis prevalence. This map will serve as a tool designed to provide the information needed to establish a positive correlation between dam and reservoir construction and schistosomiasis outbreak. Demonstration of a significant positive correlation will promote the consideration of the potential adverse health effects caused by water development. The purpose of the map is to deter further dam and reservoir construction in areas with endemic schistosomiasis, promote pre-construction examination of schistosomiasis prevalence, promote the instillation of snail (schistosoma reservoirs) abundance monitoring systems in areas with dams, and to make schistosomiasis control a key factor in the planning and building of dams. Background: Schistosomiasis, also known as Bilharzia or Snail fever, is a parasitic disease caused by trematode flatworms of the genus Schistosoma. It is a major source of morbidity affecting over 200 million people worldwide and it is endemic to 76 developing countries throughout the tropics. The prevalence of schistosomiasis demonstrated in Figure 1 is changing dramatically due to control programs in Asia and the Americas that have eliminated or drastically reduced transmission however; similar success has yet to be achieved in sub-Saharan Africa as its prevalence of schistosomiasis is increasing. i Three species of schistosomiasis, S. haematobium (Africa), S. japonicum (Japan, Southeast Asia, Western Pacific) and S. mansoni (Africa, Southwest Asia, Brazil, Caribbean) are responsible for the majority of schistosomiasis infection while the other two species, S. intercalatum and S. mekongi parasitize humans to a much lesser extent. Humans are the most important reservoir for S. haematobium and S. mansoni and are infected when exposed to contaminated freshwater (e.g., when wading, swimming, or bathing). ii The life cycles of the human schistosomes, as seen in Figure 2, are generally similar. Eggs are released into the environment from the urine or stool of infected individuals. Once the eggs reach water, they hatch to release free-swimming miracidium. The miracidium then infect the intermediate host, a freshwater snail, by penetrating its foot. The host snails of the important human schistosomes are those of the genera Biomphalaria (S. mansoni), Bulinus (S. haematobium) and Onchomelania (S. japonicum) as seen in Figure 3. After infection, asexual proliferation occurs in the snail and thousands of new larval parasites known as cercariae emerge. When humans are in contaminated freshwater, cercariae attach to, explore, and ultimately penetrate the skin. The cercariae morphs into a migrating schistosomulum and travels to the lungs. In the lungs, the schistosomlum undergoes developmental changes, which allow it to migrate to the liver where it feeds on redblood cells, grows into an adult worm and finds a partner. After finding its mate, the pair unites and copulation begins. Pairs of male and female worms relocate to the rectal veins, in the case of S. mansoni and S. japonicum, and in the case of S. haematobium, the worms migrate to the perivesical venous plexus of the bladder, kidneys and ureters. S. mansoni and S. japonicum eggs pass through blood vessel and intestinal wall to be passed out the body’s feces. S. haematobium eggs pass through the ureteral or bladder wall and exit the body in the urine. Worm pairs can dwell in the body for an average of four and a half years, but may persist up to 20 years. The pathology associated with schistosomiasis is caused by the cellular infiltration resulting from antigens secreted by trapped eggs. These antigens elicit a vigorous bodily immune response creating illness, rather than the worms themselves. Acute clinical manifestations of schistosomiasis include abdominal pain, fever, cough, diarrhea and hepatosplenomegaly (FIGURE 4) while individuals with persistent infections may suffer from severe symptoms such as cystitis and ureteritis, pulmonary and portal hypertension and bladder cancer.iii Currently, there is neither a vaccine nor is there chemoprohylaxis for schistosomiasis available. The most effective treatment for schistosomiasis is prescription Praziquantel, which treats all three forms of the disease. Drug treatment is effective at killing parasites already in the body, however it does not prevent new infections. For this reason, repeated treatments are often necessary and prevention of transmission is of the utmost importance. The most significant part of the schistosomiasis lifecycle for this project is the availability of suitable snail hosts in bodies of freshwater that are accessible to humans. Dams themselves do not cause schistosomiasis, but rather promote schistosomiasis transmission by dramatically altering the surrounding snail ecology and environment. The resulting ecological changes significantly extend the range of the snail habitats thereby promoting the proliferation of both snail reservoirs and cercariae parasites.iv Conditions supporting snail development are beaches located in the areas higher than 175 m but lower than the flooded water level, which are created upon dam construction. Predictive studies have demonstrated that beaches that form after the dam construction caused by the decrease in velocity of water flow and the sedimentation of silts make suitable habitats for snail reservoirs of schistosomiasis. Experimentation has shown that the vegetation, soil and physical and chemical characteristics of beaches in areas where reservoirs have been constructed are like those that are currently endemic to schistosomiasis.v Furthermore, ditches that surround migratory settlements created after damn construction are ideal breeding grounds for snails. vi Dam construction in Nigeria raises particular concern, as it is a country endemic to schistosomiasis. In response to the Sahelian drought in the 1970s, there was an increase in dam construction in Nigeria. Of 325 formal dams now registered in Nigeria, over 226 were constructed since 1970. More than 200 of these dams were built in the 10 most endemic schistosomiasis states and the rest in the other 26 less endemic states.vii Due to this upsurge of dam construction in Nigeria since 1970, schistosomiasis outbreak has been recorded in many areas. There have been multiple studies on the increase in schistosomiasis prevalence near water development projects in Nigeria. A study done by the University of Ilorin, Nigeria verified that intestinal helminthes infections among school-aged children were recovered at an overall prevalence of 78.3% of 309 children examined in the Eko-ende and Ore areas near the Erinle Dam Reservoir in Osun State, Nigeria and Schistosoma mansoni was one of the three most prevalent infections. viii A subsequent study by Oladejo et al. conveyed that the mean Schistosoma haematobium infection rate in school children in the rural areas of Oba-ile and Ilie was 46%. This study also showed that, Bulinus globosus, the snail reservoir, was present in abundance and continually throughout the year.ix These studies indicate the prevalence of more than one type of schistosoma infection within Nigeria, as well as the abundance of the snail reservoir species within close proximity to dam sites. A study conducted among school children living near the Bakalori Dam in Nigeria found that 52.1% of the subjects were positive for the test of urinary schistosomiasis (S. haematobium), and concluded that the prevalence of schistosomiasis was high and demanded intervention.x Not only has the burden of schistosomiasis in Nigeria been verified by numerous studies, but it has been confirmed that viable snail species are in highest concentrations in areas surrounding dams. A study done by the department of zoology at the University of Ibadan found that the Owena river damn in Idanre was the richest (of all surrounding areas) in molluscan fauna, including the intermediate species B. globosus and Biomphalaria Pfeiffer, which were continuously shedding cercariae.xi The impact of schistosomiasis outbreak due to dam construction is undeniable. Many of these studies call for an intervention of some kind within the study region, but due to the number of dams and corresponding the schistosomiasis prevalence within the country of Nigeria, a national campaign cannot be effectively designed without a tool that effectively compiles and organizes the data. Methodology Since this project attempts to create a map of schistosomiasis prevalence in relation to dam locations of the entire country of Nigeria, the most efficient way for this to be accomplished is by a state-by-state breakdown, starting with the most endemic states. The project will be designed as a two-part study where first, Global Information Systems (GIS) and Global Positioning Systems (GPS) will be used to identify the exact location of the dams within the state and study villages within close proximity to the dam, and second data will be collected to determine schistosomiasis prevalence in the study villages. Global Information Systems and Global Positioning Systems have become increasingly affordable and used to improve epidemiological research to better understand how ecological variation affects the distribution of intermediate hosts of schistosomiasis. A study was done in China regarding the distribution of Oncomelania hupensis (the intermediate host snail of Schistosoma japonicum) using GPS coordinates to map the 11 villages in which the researchers performed cross sectional surveys.xii Studies have shown that the use of GPS and GIS technologies for mapping epidemiological data promotes intersectoral collaboration for disease control, allows better analysis of spatial distribution of parasite infection in relation to environmental factors, and aids in the design of optimal drug or health measure delivery systems. Studies have also supported the use of GIS technology to serve as tools for spatial distribution data collection and potential use as tools for parasite control.xiii, xiv GIS and GPS imaging allow epidemiological data to be mapped with great accuracy, providing better data to make a strong case for the positive correlation between dams in Nigeria and increased schistsomiasis prevalence in local areas. In this study, the GIS and GPS will be used to ensure the accuracy of the map produced, by using satellite data to confirm exact coordinates of dam locations and the proximity of villages with schistosomiasis. By solidifying the accuracy of the map and the exact locations with endemic schistosomiasis in relation to the location of the dam, not only can the most effective intervention strategy be developed, but also a more accurate picture of the exact effect of the dam on the prevalence of schistosomiasis including a precise measure of at risk proximity can be constructed. For the data collection aspect of the study, data will be obtained in the form of previously conducted post-dam construction studies measuring schistosomiasis prevalence in specific locations. If no data exists for the identified site then urine filtration tests and Kato-Katz smears to identify schistosome eggs will be performed in primary school-aged children (5-14 years) to determine prevalence. This method of determining prevalence will be used in order to assess the actual prevalence of schistosoma infection in the populations as opposed to using a predictive model of infection based on environmental and climate indicators. Researchers have used primary school age children participants to determine the prevalence of schistosomiasis in communities since children ages 5-14 years have the highest prevalence of any age group of infection in Nigeria. xv,xvi Although the dams specifically effect the population of infectious snails in the water, and measuring the density of infectious snails in the water would give a more precise view of the impact of the dam (and would control for human water contact habits), this study aims to specifically show the effect of the increased infectious snail population (caused by the dam) on the surrounding human population. This method also controls for the fact that there is not a significant amount of data measuring the density of infectious snails in the water pre-dam construction, which would weaken the positive correlation that this study aims to establish. Once all previous data is collected and necessary additional studies are conducted, all of the data can be compiled into a map with all dam locations flagged with corresponding color-coded schistosomiasis prevalence. Significance A map of all of the dam locations in Nigeria with color coded indicators of schistosomiasis prevalence corresponding to dam location would be an invaluable tool for developing a nation-wide intervention program to reduce the prevalence of schistosomiasis. In areas that may have low prevalence and incidence of schistosomiasis, a drug treatment intervention could be planned, as opposed to areas that have high endemicity and are in close proximity to dams, where molluscides or elimination of host species may be a more appropriate intervention. More importantly, academic literature on schistosomiasis in Nigeria is lacking comprehensive data showing the effect of dams/reservoirs on schistosomiasis prevalence in local communities. The map will be used as a way to indicate the cumulative effect of dam construction on schistosomiasis prevalence. Since many sites lack pre-dam construction data of schistosomiasis prevalence, the color-coded map will provide evidence of the high correlation between the presence of dams and schistosomiasis endemicity. The map will be used as a tool to aid the national government (and private sectors) to consider the adverse health effects of water development projects before undertaking dam construction and will eventually lead to a shift toward improved dam engineering strategies and alternative energy and water sources. With a tool that can effectively show the direct correlation between dam development and schistosomiasis outbreak, not only can undertaking water development projects be reconsidered, but also locations for dam projects can be more strategically placed to reduce the prevalence of schistosomiasis and its associated morbidity. Fewer dams constructed in endemic states of Nigeria will directly prevent the over-abundance of intermediate host snail species that release cercariae into water used for recreation, bathing, washing, and drinking by local residents, thus there will be a decrease in schistosomiasis incidence. Furthermore, even if the Nigerian government (or dam constructing entity) decides to proceed with dam construction despite evidence of the potential for a schistosomiasis outbreak, they can still test the prevalence of schistosomiasis infection before the project is underway, providing more opportunities for researchers to indicate causation instead of simply correlation. Furthermore, if the government is aware of the associated health risk of dam construction, the post-dam snail abundance can be continuously monitored, which would better assist an intervention using molluscides to control snail population before it reached a point of abundance that would be too difficult to control. Most importantly, schistosomiasis prevalence is second only to malaria and is endemic to Nigeriaxvii, and due to the recent (since 1970) upsurge of dam construction, Nigeria is the optimal place for this mapping project to occur. Because droughts are common in Nigeria, dam construction will not be coming to an end anytime soon, which is why this map is essential for future control and prevention of schistosomiasis. Conclusion: The burden of schistosomiasis weighs heavily on the citizens of Nigeria, which is why it is imperative that not only intervention, but also prevention becomes an integral role of a national campaign to reduce the morbidity caused by schistosomiasis. Using GPS/GIS technology and data on schistosomiasis prevalence from previous and newly conducted studies, this project will produce an accurate and specific mapping of schistosomiasis prevalence of communities in close proximity to dam locations. The proposed color-coded map of dams and schistosomiasis prevalence will undoubtedly serve as a key tool in the prevention of schistosomiasis outbreak nationwide. APPENDIX FIGURE 1 Geographic distribution of schistosomiasis. Source: Center for Disease Control. Prevention of Specific Infectious Disease: Schistosomiasis. http://wwwn.cdc.gov/travel/yellowBookCh4-Schistosomiasis.aspx Date Accessed: May 15, 2008. FIGURE 2 Schistosomiasis Life Cycle Source: Ross G, Bartley PB and Sleigh AC, Olds GR, Li Y, Willliams GM,McCanus DP. Schistosomiasis, N Engl J Med 2002;346:1212–1220. FIGURE 3 Source: Masden et al. “Bilharzia in Lake Malawi, What are the facts?” NSF/NIH joint project in Ecology of Infectious Disease (DEB-0224958). FIGURE 4 source: Oneil. “An individual in chronic stages of Schistosomiasis” .University science. Irish Universities Promoting Science. <<http://www.universityscience.ie/pages/scientists/sci_sandraoneill.php> i Chitsulo L, Engels D, Montresor A, Savioli L. The global status of schistosomiasis and its control. Acta Trop 2000;77:41-51. ii WHO Expert Committee. Prevention and control of schistosomiasis and soil-transmitted helminthiasis. World Health Organ Tech Rep Ser. 2002;912:1-57. iii Ross G, Bartley PB and Sleigh AC, Olds GR, Li Y, Willliams GM,McCanus DP. Schistosomiasis, N Engl J Med 2002;346:1212–1220. iv Li, Y, Raso G, Zhao Y, He HK, Ellis M, and McManus DP. Predicted impact of large water management projects on schistosomiasis transmission and control in the Dongting Lake Region, China. Emerg. Infect. Dis. 2007;13:973-979. v Scientific leading Team of Chinese Academy of Science. Studying on environment of Three Gorge Project. Proceedings of Ecological and Environmental Impact of Three Gorge Project and Strategies. Science Press, 1987. pp. 277–923. vi Zheng J, Gu XG, Xu YL, et al. Relationship between the transmission of schistosomiasis japonica and the construction of the Three Gorge Reservoir. Acta Trop 2002; 82:147–56. vii Oladejo SO, Ofoezie IE. “Unabated Schistosomiasis Transmission in Erinle River dam, Osun Sate, Nigeria: evidence of environmental effects of development projects.” Trop Med Int Health. June;11 2006;6:843-50. viii Ugbomoiko US, Ofoezie IE. “Multiple infection diagnosis of intestinal helminthiasis in the assessment of health and effect of development projects in Nigeria.” J.Helminthol. 2007 Sep; 227-31. Epub 2007 June 21. ix Ibid., at 7 x Umar AS, Parakoyi DB. “The prevalence and Intensity of Urinary Schistosomiasis Among School Children Living in Bakalori Dam, Nigeria.” Niger Postgrad Med J. 2005 Sep; 12(3):16872 xi Odaibo AB, Adewunmi CO, Olorunmola FO, Adewoyin FB, Olofintoye LK, Adetula Mo, Awe CO, Akinyemi F.”Afr. J Med Med Sci. 2004 Sep; 33(3): 219-24. xii Yang K. Wang Xh, Yan GJ, Wu XH, Qi YL, Li HJ, Zhou Xn. “An integrated approach to identify distribution of Concomelania hupensis, the intermediate host of schistosoma japonicum, in a mountainous region in china.” Int J Parasitol. 2008 Jan 24. Brooker, S., Michael E. “The potential of geographical information systems and remote sensing in the epidemiology and control of human helminth infections” Adv. Parasitol. 2000;47:245-88 xiv N.R. Bergquist. “Vector-borne parasitic diseases: new trends in data collection and risk assessment” Elsevier Science B.V. 2001. xv Olaseha IO, Sridhar MK. “Participatory action research: community diagnosis and intervention in controlling urinary schistosomiasis in an urban community in Ibadan, Nigera.” Int Q Community Health Educ. 2005-2006; 24(2): 153-160. xvi Umar AS, Parakoyi DB. “The prevalence and Intensity of Urinary Schistosomiasis Among xiii School Children Living in Bakalori Dam, Nigeria.” Niger Postgrad Med J. 2005 sep; 12(3):16872 xvii Ibid., at 13