10-11 - UAB School of Optometry
advertisement

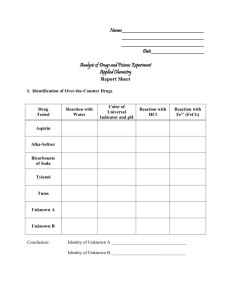
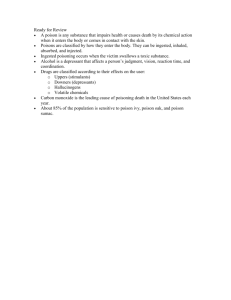
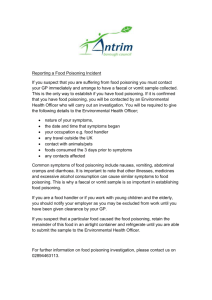
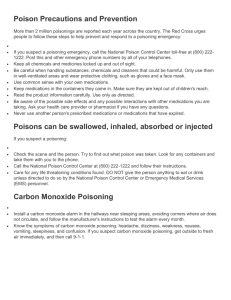
FUN2: 10:00-11:00 Scribe: Ashley Holladay Thursday, December 11, 2008 Proof: Teresa Kilborn Dr. Smith Toxicology Page 1 of 5 Toxicology Abbreviation MOA- mechanism of action, CO- carbon monoxide, OTC- over the counter I. [S1]Introduction to the principles of toxicology:- emphasis on understanding the mechanism of action of toxic agents- by understanding the MOA of a drug or environmental metal or poison have a much greater possibility of accurately assessing the risk of exposure and developing antidotes to toxic damage to the tissues that are affected by the poison. We use information of the MOA in diagnosing (Ex- CO kills nearly 1000 people per year- but is easily diagnosed.) II. [S2] a. He won’t spend much time on cyanide or arsenic- covered in the powerpoint. Arsenic is a relevant poisonfound in herbicide and pesticides b. People that work with these things are exposed to these things c. Arsenic- carcinogenic metal- pretty high risk in the US- found in well waters in the US d. Spend most of time on methanol poisoning (we understand this MOA), lead and mercury poisoning. III. [S3] a. Basic principle same for poison as for drugs. b. The dose distinguishes a poison from a drug. c. All substances are potential poisons. The chief goal of toxicology is to assess risk. Associated with the use of a drug or exposure to a chemical. d. Most poisonings are dose related. Dose is proportional to the concentration you might breathe in over time. e. Exposure = Concentration X Time IV. Dose Effect [S4] a. LD50- Dose of a poison that causes 50% lethality. b. This is done mostly in experimental animals. You determine the LD50 from a graph c. [S5] The range of LD50s for toxic agents is enormous. d. Some toxic agents that are most potent (botulinum toxin) produce relatively few deaths because we know how to avoid exposure. e. Ethanol, which has a relatively low potency, is responsible for many deaths. (automobile accidents) f. [S6] Toxicity test done in animals because they cannot be done in humans, but there are some limitations. g. Have to assume that it has the same affects in animals as it does in humans. It may or may not have the same MOA on the experimental animal as it does on humans. h. Difficulty in assessing risks is extrapolating risks from exposures of high doses of poison to low doses in carcinogenic agents. It is a necessity to do this because the incidence of cancer is usually 1/ 10000 or less. i. This would require large numbers of animals which is not feasible. V. Dose-related toxicity [S7] a. Most toxicity is dose related. An exception to this is an allergic reaction to a chemical. b. Usually one or a few organs are affected and it is usually not where the concentration is the highest. c. Most exposures produce dose related toxicity. d. Not necessarily where the concentration is the highest in the animal. e. Many affect the CNS. It is the most frequently affected organ in systemic toxicity. f. Many agents are highly specific in their MOA. VI. Acute poisoning [S8] a. In regards to acute poisoning, we want to terminate exposure and provide supportive care. We are dealing with emergency situations. We want to make sure the airway is open and the heart is beating and get the individual out of the environment with the poison (CO for example) b. Once the individual is stabilized we want to minimize the amount of the poison in the critical tissues. c. Lastly, we want to combat the toxic effects of the toxin by administering an antidote or some agent that is able to decrease the toxic effect of the particular poisoning. d. (also be talking about acetaminophen poisoning in the liver) VII. Decrease Absorption of the poison [S9] a. Different ways to decrease absorption if it has been ingested. b. Older way would be to induce vomiting but this has now been contraindicated. c. Preferred in hospital setting- stomach tube and gastric lavage to remove the poison from the stomach. This can be enhanced by activated charcoal. Carbon charcoal- ground to very fine powder w/ a very large surface area that binds a variety of organic molecules administered by oral suspension and removing it from the stomach it can further enhance the removal of organic compounds. d. Hemodialysis- efficient and rapid method of removing poisons from the blood VIII. Carbon Monoxide Poisoning [S10] a. Responsible for almost 500 deaths/ year, 1000s of hospitalizations, often goes undiagnosed in ERs b. Why is it so dangerous? FUN2: 10:00-11:00 Scribe: Ashley Holladay Thursday, December 11, 2008 Proof: Teresa Kilborn Dr. Smith Toxicology Page 2 of 5 c. Comes from incomplete combustion (leaky hot water heaters, not burning gas completely) Incomplete combustion, such as when there is a limiting amount of oxygen, produces CO. d. [S11] If you are exposed to it and you are not active, it just creeps up on you and you pass out. If you are exercising, you notice. If just resting, you go to sleep without any indication that something is wrong. e. Its target is hemoglobin. Hemoglobin has a very high affinity for CO- much higher than its affinity for oxygen. f. Carboxy- hemoglobin has a characteristic cherry-red color even in the venous blood. g. Goal- rapidly terminate exposure. If a person is still conscious this is adequate. IX. CO [S12,S13] a. Breathing 20% oxygen air is sufficient to displace the CO and no other further treatment is needed if a person is still conscious. b. If the person is unconscious, time is of the essence. To replace the CO bound to hemoglobin it is more rapid and efficient if you put the person in a hypobaric chamber where they can breathe 100% oxygen to displace the CO. Without a supply of oxygen to the tissues- death will come quickly. X. Cyanide [S14,S15] a. He skips cyanide in the lecture- we can read this from the powerpoint. XI. Methanol [S16] a. Same thing occurs with the agent ethylene glycol (coolant/antifreeze in cars) b. It is a metabolite that causes the toxicity in methanol and ethylene glycol poisoning. c. The goal is to inhibit the metabolism of the methanol or ethylene glycol and to eliminate them from the body which can be done by normal kidney elimination as long as there is administration of an antidote that prevents metabolism of these compounds to the toxic agents. XII. Methanol Poisoning [S17] a. Pathway for methanol by metabolism by alcohol dehydrogenase (same enzyme for ethanol) b. Converts methanol to formaldehyde. c. Formaldehyde further reduced by the enzyme aldehyde dehydrogenase to toxic metabolite- formic acid. d. Formic acid is the culprit that causes blindness by damaging the ganglion cells of the retina of the eye. A small amount of accidental methanol ingestion will cause blindness unless metabolism is inhibited and the methanol is eliminated in urine. If exposure was excessive, it would be important to use hemodialysis to remove from the blood. The antidote must be administered to prevent metabolism of the methanol to the formic acid. e. The antidote for methanol poisoning is 4-Methylpyrazole. (In the old days, you would simply administer an excess of ethanol so that those enzymes would be saturated with ethanol and the enzymes would metabolize the nontoxic ethanol and the blindness would be avoided.) XIII. Ethylene Glycol [S18] a. Ethylene glycol is similarly metabolized by alcohol and aldehyde dehydrogenases and the product is oxylate- a dicarboxylic acid, which is a 2 Carbon compound with 2 carboxyl groups. b. The problem with the metabolite is that it binds very tenaciously with calcium. It produces an insoluble calcium oxylate precipitate that damages the kidney. c. There are many cases of pets ingesting this. d. Diagnose by looking at urine under the microscope and see the crystals of calcium oxylate. It also contains a fluorescent compound that can easily be detected by a UV light in urine sample. XIV. Acetaminophen Poisoning [S19] a. Responsible for liver failure in almost 1000 people in the US per year (almost a third of those die) b. Toxic at only 2-3 times the daily recommended dose- individuals often exceed the daily recommended dose because it is in many OTC drugs besides just Tylenol and pain relievers. c. The liver failure can caused by this can only be treated by liver transplant. d. SQ: How long would it take to cause this effect of toxicity- 1 dose or chronic? e. A: It will depend on the individual. But generally it will have to have some chronic use over a period of days or weeks or longer. Heavy alcohol use or other factors can increase the risk. XV. What is the basis for the poisoning of acetaminophen? [S20] a. It is the metabolism, or in a sense, an incomplete metabolism to a reactive nucleophile that causes the liver damage. b. The poisoning and toxicity of acetaminophen depends on exceeding the body’s capacity to detoxify the agent. c. If you are exposed to minimal levels of acetaminophen that do not exceed the toxic dose, you will metabolize it, and you may produce a very small amount of toxic metabolite. But a small amount of toxic metabolite isn’t sufficient to cause liver failure. It may cause damage to some liver cells. d. Reason for that is in part that we don’t exceed the liver’s capacity to metabolize the acetaminophen to a non toxic glutathione conjugate. FUN2: 10:00-11:00 Scribe: Ashley Holladay Thursday, December 11, 2008 Proof: Teresa Kilborn Dr. Smith Toxicology Page 3 of 5 e. At the toxic level, the glutathione level in the liver becomes depleted, and then the acetaminophen is incompletely metabolized and it doesn’t become modified by glutathione and instead remains this toxic intermediate that damages the liver. f. The liver failure and the excessive production of the toxic metabolite of acetaminophen does not become sufficient until the level of glutathione in the liver falls below the level needed to maintain metabolism of acetaminophen to the non-toxic form. XVI. Acetaminophen [S21] a. In this slide, examples of damage to liver cells, these holes in the liver are characteristic of acetaminophen poisoning. b. There is to some degree genetic influence on the poisoning. i. There is a gene called the CAR gene. ii. If it is inactivated then there is a decrease in susceptibility to acetaminophen poisoning. iii. We don’t fully understand the susceptibility to acetaminophen poisoning although we do know a lot about the metabolism to the toxic intermediate. iv. There is a genetic component. c. The maintenance of glutathione levels is essential for avoiding liver damage by acetaminophen. XVII. Antidote for acetaminophen [S22] a. The antidote for acetaminophen poisoning is to administer a precursor to glutathione. b. It contains an amino acid of glutathione. c. Glutathione is composed of three amino acids: glutamate, cystine, and glycine. It is a modified tripeptide. It is not the usual glutamate, it is called gamma glutamate. d. The limiting amino acid for synthesis is cystine. By administering the N-acetyl-cystine which is a form of cystine that has a higher bioavailability than cystine. It is a more effective form. e. If someone is exposed to excessive amounts of acetaminophen, then N acetyl- cystine is administered in order to maintain levels of glutathione in the liver that are normal. As long as that is done, then the acetaminophen will be completely metabolized and eliminated and the toxic intermediate will not be produced in sufficient levels to cause liver damage. XVIII. Organic Solvents [S23] a. Responsible for some toxic exposures and they generally depress the CNS b. One of them is widely used in gasoline- benzene. c. It is an additive to premium gasoline. d. Benzene is a toxic agent that causes leukemia and aplastic anemia. e. He’s unclear on how much the street exposure increases our risk for leukemia or a plastic anemia (complete wipe out of all blood cells- irreversible). More research is needed here. XIX. Metals [S24] a. Very significant risk for exposure in the US. b. If you are interested in Arsenic, look at it in the handout. i. It affects energy metabolism, the production of ATP. ii. It is a carcinogenic metal. iii. It is a public health concern because of its presence in well water particularly the Western US and other parts of the world. c. Metals are among the oldest drugs and toxins known to man. The problem is the more we use them, we increase our exposure to them. We have to take action to reduce the exposure to metals such as lead and mercury. XX. Lead (Pb) Poisoning [S34] a. Lead poisoning is occurring in epidemic proportions in the US now and in the past couple decades. b. We know that so many children have suffered irreversible damage to the CNS and become impaired in the ability to learn and perform in school because of lead poisoning. c. Lead poisoning and other metals is readily diagnosable be simply measuring the metal content in the blooddefinitive basis for diagnosis. FUN2: 10:00-11:00 Scribe: Ashley Holladay Thursday, December 11, 2008 Proof: Teresa Kilborn Dr. Smith Toxicology Page 4 of 5 d. Mother’s are growing more concerned as children play with toys that are covered in lead containing paint. The epidemic is coming from neighborhoods where there are older homes that are painted with lead containing paints, outside paints especially. They can contain 50% or more of lead. e. Kids absorb the lead more efficiently and are more toxic to it. This leads to CNS problems in kids especially. We need ways to monitor the environment and make sure that the environment is cleaned up or marked as a high lead environment. f. [S36] Lunch boxes are another example of lead contaminants. g. [S36-37] Lead toxicity primarily inhibits the production of heme, the red pigment of blood. i. Lead inhibits two enzymes as seen diagrammatically. ii. Lead inhibits the last step where the iron is inserted and another step at the beginning of the pathway where aminolevulinic acid (ALA) is further metabolized to porphobilinogen. iii. In lead poisoning, there is a huge accumulation of ALA in the blood. iv. In generally, this inhibition of heme production leads to anemia, which is a key characteristic of lead poisoning, but is not responsible in any direct way for damage to the brain. What is responsible for that? We don’t know v. When heme is synthesized, normally it feedback inhibits ALA synthesis. But with the blocked formation of heme, there is no feedback inhibition of ALA synthesis. In addition, ALA utilization is blocked thus, enormous accumulation of ALA in the blood. This is another tip off for lead poisoning. h. [S38] The CDC has over the years revised their action control level for lead poisoning downward. In the 60’s and 70’s it was 60 ug/dL. That was the level at which action was required to remove the lead from the blood and now it is down to 10ug/dL. It is a problem throughout the US, including Jefferson County. Children < 6 years old were tested at 8 clinics and 117 had blood levels with 15 ug/dL. Millions of children have already been irreversible damaged by elevated blood lead levels. i. [S39] One major source of lead in the environment in the past, was gasoline. It was an additive in gasoline. Look at diagram. It shows what the industry maintains (ie. There is not increase in lead blood levels with leaded gasoline). This shows that leaded blood decreased when there was increasingly limited use of leaded gasoline. XXI. Mercury Poisoning [S42] a. [S42] Classic example of Mercury poisoning is Minamata. Minamata is a sea coast village in Japan where there was a Cheesos factory. Eugene Smith, famous photographer, photographed many pictures of the mercury poisoning. How did it happen? b. [S43] They dumped the mercury waste of their factory into the harbor and it sunk to the bottom because it is heavy. At the bottom, it doesn’t simply as the mercury metal because it is metabolized by microorganisms which add the addition of methyl groups to the mercury. It becomes methyl mercury or dimethyl mercury. The problem then is it is accumulated in the food chain. The early indications that something was wrong in Minamata was that cats were jumping into the sea and dying. This was because they were eating the fish that were eating the microorganisms contaminated with mercury. It is not a Minamata problem though, it is a global problem. c. [S44] Headline last month from The Birmingham News. One electricity power plant in Jefferson County produces more mercury into the atmosphere than any other one in the US. It produces more than 2,000 lbs. Most power plants are much cleaner and only produce about 1,000 lbs. of mercury emission into the atmosphere. Where does it go? It falls back to the earth and then it rains. When it rains, it washes it into the rivers and the lakes and into the soil. There it is metabolized into methyl mercury and it is eaten by microbes and fish. What about the risk of large mouth bass? How much mercury do they contain? There is a very big risk, he says not to eat it if you’re pregnant. Some mothers may think that they are doing their kids right by giving their kids fish sandwiches, but this may not be the case. If they get mercury poisoning and it is diagnosed early then it can be reversed, but after a point it is reversible. d. He wants us to look at the treatment of metal poisoning on our own. A chelator binds the metal and helps it to be eliminated in the urine. Succimer is an important relatively new treatment. Take a look at the properties of it. It can be administered orally. It doesn’t deplete essential metals. There is also a section on dental amalgams. They have always been known to have high levels of mercury, but it was thought to be inert. Turns out it isn’t inert. It is released when you grind on the surface of the amalgam and some is released into the body at that FUN2: 10:00-11:00 Scribe: Ashley Holladay Thursday, December 11, 2008 Proof: Teresa Kilborn Dr. Smith Toxicology Page 5 of 5 time. The ADA maintains that there is no health risk and doesn’t cause and clinical symptoms. The point is that we are being exposed increasingly, and do you want the additional exposure of dental amalgam that you don’t have to have? [End 52:55]