postpartum Obstetric Data collection
advertisement

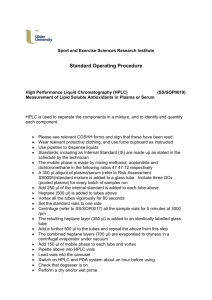
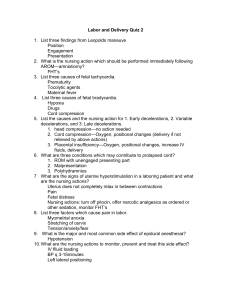
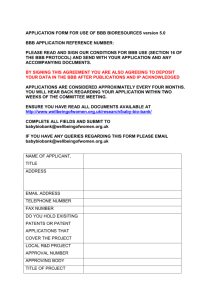
CHAPTER 8 POSTPARTUM OBSTETRIC DATA COLLECTION 8.1. Overview The main purpose of the postpartum data collection is to collect information on neonatal and labor and delivery outcomes. Postpartum OB data collection is primarily obtained through chart review and abstraction from electronic and paper charts. Specimen collection occurs before and during the delivery, and includes maternal and fetal cord blood, and placental biopsies. A postpartum participant interview administered while the participant is still in the hospital will collect additional pregnancy history. In addition to OB data, within 72 hours of delivery, and while the participant is still in the hospital an oral bedside examination with plaque specimen collection is conducted. The periodontal data collection is documented in Chapter 9. 8.2. Timing /Scheduling of the Postpartum Data Collection This data collection is very time dependent. It is critical that each center have a system in place that will identify MOTOR participants at delivery. Each center must devise a method to review the patient census in the Labor and Delivery (L&D) Units using active study participant lists. In addition, there must be a mechanism that identifies study participants to the OB staff in the L&D Unit to assure that study specimens are collected and stored for later processing by MOTOR staff. Most of the study deliveries are expected to occur at each center’s hospital labor and delivery unit. However, this will not be true for all cases. For those deliveries that occur at other hospitals, postpartum data must be collected on the Labor and Delivery Form (LDF), the Neonatal Baseline Form (NBF), and the Neonatal Intensive Care Form (NIC). This may require a release of records and consent from the participant in order to allow the MOTOR staff to receive and abstract records from the delivering hospital. Once a participant has been identified as delivering or having delivered, a determination of discharge date must be made in order to obtain the remaining data. Participants may be discharged within a 24-hour period; however, most will be hospitalized for a minimum of 24 hours. Participants who deliver by C-section usually remain hospitalized for an additional day. It is crucial that the delivered participant be identified and that study data be collected prior to discharge. This will require the study staff to make an appointment with the delivered participant immediately to collect the participant interview and the bedside oral exam. Additional data collection on the neonate’s health status is possible during the first five years of the neonate’s life. This will be addressed in a later document. CHAPTER 8: Post-Partum Obstetric Data Collection 09/13/06 Page 8 - 1 8.3. Staffing Staff involved with collection of MOTOR postpartum OB data must have completed appropriate training and certification procedures (see Chapter 2). 8.4. Procedures and Forms The following procedures and data collection forms are required for postpartum OB data collection: Postpartum Specimen Collection o Maternal Blood Collection Form (MBF) o Postpartum OB Sample Collection Form (POS) o Maternal Serum Sample Collection Specimen Collection Packet #4 for Maternal Serum o Specimen Collection Packet #5 for Fetal/Placental Specimens Fetal Membrane Roll Placental Specimen Collection Umbilical Cord Sample Fetal Cord Blood Sample Collection Labor and Delivery Data Form (LDF) Neonatal Baseline Form (NBF) Neonatal Intensive Care Form (NIC) Note: Specimens are to be collected only on participants who have given consent for collection. Note: Specimen processing and/or shipping instructions and tracking logs are documented in Appendix 3. 8.4.1. Maternal Blood Collection 8.4.1.1. Postpartum Maternal Blood Collection Packet # 4 MOTOR specimen collection packet #4 contains the pre-labeled tubes necessary for postpartum maternal serum collection. In addition, extra pre-coded labels ending with ‘000’ are included as ‘paperwork’ labels, one to be affixed onto the POS, others for use in processing (such as centrifuge tubes). Maternal Blood Collection Form ID: ___ ___ ___ ___ ___ ___ ___ ___ Form: MBF Ver: A Visit #: __ __ Seq #: 01 Name: _________________________ Staff ID: __ __ __ Date: __ __ / __ __ / 20__ __ Instructions: This form is completed when either a baseline or postpartum maternal blood specimen is collected. Code MBF as Visit 02 for baseline and as Visit 04 for postpartum. Attach the corresponding extra label from the specimen collection packet in the box below. 1. Maternal blood sample collected Y 2. Date maternal blood sample collected N → Go to Q #5 __ __ / __ __ / 20 __ __ 3. Time of maternal blood sample collection (Record in military time) __ __ : __ __ 4. Place extra label from the OB Blood Collection Packet #1 (prenatal) or #4 (post-partum) in the box below. Enter specimen ID number into MOTOR DMS. Label from collection packet #1 (prenatal) or #4 (post-partum) here 5. Comments Y N ______________________________________________________________________________________ ______________________________________________________________________________________ 8.4.1.2. Maternal Blood Collection Form (MBF) CHAPTER 8: Post-Partum Obstetric Data Collection ______________________________________________________________________________________ ______________________________________________________________________________________ 09/13/06 Page 8 - 2 The Maternal Blood Collection Form (MBF) is used to document the collection of (or inability to collect) maternal blood specimens, and to provide the linkage of the participant ID number to the specimens that are shipped to the lab. When a specimen is collected, it is noted on the form with the date and time of collection. One of the extra labels (ending in ‘000’) from packet #1 is to be affixed to the form in the place indicated. Refer to the MBF QXQ’s for specific instruction on completing this data collection form. Note: Postpartum visits are recorded on the form as visit=04. 8.4.1.3. Postpartum Maternal Blood Specimen Collection Hospital or Motor staff should draw the maternal blood upon admission to the Labor and Delivery Unit. In the event the blood was not drawn, another needle stick during the patient’s hospital stay is necessary to collect this sample. The sample may be collected after delivery and the date and time the sample was taken must be recorded on the MBF (visit 04). After collection of maternal blood in a 5 ml red-topped SST (serum separator tube) the tube should sit at room temperature for 45 minutes to allow clot formation. The SST tube should be labeled with a “paperwork” barcode label (ending in “000”) provided in the collection packet #4. Centrifuge the SST between 10 to 15 minutes to produce an adequate separation of serum. An adequate separation occurs when the red cells are contained below the gel separator and the serum above the gel separator contains no red cells. Spin time will depend on RCF that can be achieved on the centrifuge used. Prior to transferring the serum from the tube personnel should wear appropriate personal protective equipment to prevent contamination from possible blood borne pathogens. Once the serum is visible, carefully remove the cap from the SST and, using a sterile pipette, transfer the serum to the red-capped vials with bar-coded suffixes 311 to 314. The serum should be aliquoted equally into each of the four vials unless the amount of serum is so small that aliquoting it into four samples would yield less than 0.7mls in each tube. If the amount of serum available is insufficient to put 0.7 mls in each tube, fill the tubes in ascending order i.e. 311 then 312. Once the serum is aliquoted make a note in the comments section of the MBF indicating which vials contain serum and which vials are empty. Care should be taken to aliquot the samples among the four vials if possible. Care should be exercised to use sterile materials and not contaminate the samples or inside of the vials or caps with materials from other subjects, personnel, or material in the serum preparation environment. Once the serum has been aliquoted into the 4 bar-coded tubes (making sure to match the first 6 digits of the barcode number on the tubes with the number on the SST collection tube) make sure an identifying paperwork label that matches is affixed to the MBF specimen collection form (sec 8.4.1 above). After the serum has been aliquoted place the tubes (311-314) either on dry ice or at or below -80°C. Detailed procedures for serum storage and shipping are found in Appendix 3. 8.4.2 Postpartum OB Specimen Collection CHAPTER 8: Post-Partum Obstetric Data Collection 09/13/06 Page 8 - 3 8.4.2.1. Postpartum OB Specimen Collection Form (POS) The Postpartum OB Sample Collection Form (POS) is used to document the collection (or inability to collect) postpartum specimens (described below) and to provide a link between the participant ID number and the specimens that are shipped to the lab. When a specimen is collected, it is noted on the form, and an extra label (ending in ‘000’) from the appropriate packet is placed on the form as indicated. Packet # 4 corresponds to question #1 fetal cord blood collection, packet #5 to the fetal membrane, umbilical cord and placenta specimens documented in questions 3-6. Data entry of the specimen ID number from the labels provides the link to the participant ID. It is critical to place the correct packet label with the correct question on the form. Post-Partum Obstetric Sample Collection Form ID: ___ ___ ___ ___ ___ ___ ___ ___ Form: POS Ver: A Visit #: 04 Name: _________________________ Staff ID: __ __ __ Date: __ __ / __ __ / 20__ __ Seq #: 01 Instructions: This form is completed when the Post-Partum Obstetric specimens are collected. Indicate all specimens collected. Attach the corresponding extra label from the specimen collection packet in the place indicated. A. Cord Blood Collection: 1. Fetal cord blood collected? Date processed: Time processed (24hr): Y N 2. Fetal membrane roll sample collected? Y N 3. Umbilical cord sample collected? Y N 4. Placental biopsy samples collected? Y N __ __ / __ __ / 20 __ __ __ __ __ __ B. Placenta Samples: Refer to the POS QXQ’s for specific instruction on completing this data collection form. 8.4.2.2. Postpartum OB Collection Packet # 5 5. Date placenta samples obtained and frozen: __ __ / __ __ / 20 __ __ 6. Time placenta samples obtained and frozen (24hr): __ __ __ __ 7. Place extra label from Postpartum OB Specimen Collection Packet # 5 in the box below. Enter specimen ID number into MOTOR DMS. Label from collection packet #5 here 8. Comments: Y N ______________________________________________________________________________________ ______________________________________________________________________________________ ______________________________________________________________________________________ MOTOR specimen collection packet #5 contains the pre-labeled tubes and vials necessary for postpartum OB specimen collection, including vials and labels needed for collection of fetal membrane roll (barcode suffice “401”), umbilical cord sample (“402”), and placental biopsy sites 1-6 (“403” through “408”). All of these vials have blue caps, so it is essential to look at the suffix numbers and make sure each specimen goes into the appropriate corresponding vial. The packet also contains pre-labeled specimen vials for fetal cord serum (red caps with barcode suffixes “351”-“353”), and fetal cord whole blood (lavender cap tubes, “551” and “552”) drawn in an EDTA tube. ______________________________________________________________________________________ The packet contains extra labels ending with ‘000’ provided for the ‘paperwork’ label to be placed onto the Post Partum OB Sample Collection Form (POS), and for collection primary containers, as well as processing tubes. 8.4.2.3. Fetal Membrane Sampling One tissue sample is obtained from the membranes within the first hour of delivery. This is a small excisional tissue biopsy of approximately 12X12 mm. It is collected using sterile tissue tweezers or hemostat and scissors. It is collected from the anatomical site shown in the following diagram and placed into the cryovial, suffix 401. The cryovial is snap frozen in liquid nitrogen prior to being placed on dry ice or stored in a -80 freezer. Ultimately, the sample must be stored in a -80 freezer. CHAPTER 8: Post-Partum Obstetric Data Collection 09/13/06 Page 8 - 4 Placental Membrane Biopsy Protocol Placenta Umbulicus Membranes VIAL 1 Excisional biopsy Site Figure 8.1 Placental Membrane Biopsy Protocol 8.4.2.4. Placental Samples Two placenta tissue blocks will be collected for each study participant. Using sterile tissue tweezers or hemostat and scissors a 5x5 mm section of the placenta will be cut from the fetal side of the placenta through to the maternal side. Each block of tissue will then be cut into three sections, a fetal section, a central section and a maternal section. Each section will be stored into a cryovial numbered for that tissue specimen, suffixes 403-408. The cryovials are snap frozen in liquid nitrogen prior to being stored on dry ice or in a -80 freezer. Ultimately, all samples must be stored in a -80 freezer. A diagram of the collection is outlined below: Figure 8.2 Placental Biopsy Protocol CHAPTER 8: Post-Partum Obstetric Data Collection 09/13/06 Page 8 - 5 Summary Placental & Membrane Biopsy Protocol VIAL 406 Fetal VIAL 407 Central VIAL 402 VIAL 408 Maternal VIAL 403 Fetal VIAL 404 Central VIAL 405 Maternal VIAL 401 Figure 8.3 Summary Placental and Membrane Biopsy Protocol The figures above illustrate the specimens to be collected and the suffixes on each of the vials. Care must be taken to use the appropriately labeled cryovials. 8.4.2.5. Umbilical Cord Sample One umbilical cord sample is obtained from the placenta within the first hour of delivery. This is a small cross-sectional tissue biopsy of approximately 3-4 mm in length. It is collected using sterile tissue tweezers or hemostat and scissors. The sample should be collected as close to the insertion of the cord to the placenta as possible. The diagram below shows the anatomical site for the sample. Once the sample is collected, it is placed in a cryovial, suffix 402, then snap frozen in liquid nitrogen. Once frozen the sample is stored in a -80 freezer. The sample may be stored temporarily on dry ice prior to final storage in the -80 freezer. 8.4.2.6. Fetal Cord Blood Collection Fetal cord blood should be collected within 30 minutes of delivery. The umbilical cord should be clamped distally and a syringe needle inserted into the umbilical vein. The syringe should be filled with venous fetal cord blood and then aliquoted into a 5 mL EDTA tube and a 5 mL red top tube (or SST tube). Blood should not be allowed to flow from the umbilical cord into a collection tube. This will allow a mixture of arterial and venous blood. If fetal cord blood was not collected as part of the delivery MOTOR study CHAPTER 8: Post-Partum Obstetric Data Collection 09/13/06 Page 8 - 6 specimens, identification of alternate sources of fetal blood and fetal cord serum should be identified. These may include obtaining a sample from a hospital laboratory after their sampling is complete, i.e. a cord blood gas. After collecting fetal cord blood in the red-top or SST (serum separator tube) tube the blood should sit at room temperature for 45 minutes to allow clot formation. The SST tube should be labeled with a “paperwork” barcode label (ending in “000”) provided in the collection packet #5. Centrifuge the SST between 10 to 15 minutes to produce an adequate separation of serum. An adequate separation occurs when the red cells are contained below the gel separator and the serum above the gel separator contains no red cells. Spin time will depend on RCF that can be achieved on the centrifuge used. Prior to transferring the serum from the tube personnel should wear appropriate personal protective equipment to prevent contamination from possible blood borne pathogens. Once the serum is visible, carefully remove the cap from the SST and, using a sterile pipette, transfer the serum to the red-capped vials with bar-coded suffixes 351 to 353. The serum should be aliquoted equally into each of the three vials unless the amount of serum is so small that aliquoting it into three samples would yield less than 0.7mls in each tube. If the amount of serum available is insufficient to put 0.7 mLs in each tube see the directions below for small amounts of fetal cord blood and serum. Care should be exercised to use sterile materials and not contaminate the samples or inside of the vials or caps with materials from other subjects, personnel, or material in the serum preparation environment. Once the serum has been aliquoted into the 3 bar-coded tubes (making sure to match the first 6 digits of the barcode number on the tubes with the number on the SST collection tube) make sure an identifying paperwork label that matches is affixed to the POS specimen collection form. After the serum has been aliquoted place the tubes either on dry ice or at or below -80°C. After filling the EDTA tube with 5 mLs of cord blood, the vial should be inverted and if possible processed within two hours. If it is not possible to process the blood within two hours it is recommended that the EDTA tube be placed in the refrigerator and processed within 24 hours. Prior to transferring the blood from the tube personnel should wear appropriate personal protective equipment to prevent contamination from possible blood borne pathogens. Carefully remove the cap from the EDTA tube and, using a sterile pipette, transfer the blood to the lavender capped vials with bar-coded suffixes 551 and 552. The blood should be aliquoted into the two vials unless the amount of blood is so small that the aliquots would be less than 0.7 mLs. If the amount of blood is insufficient to put 0.7 mLs of blood in each of the tubes use the directions below for small amounts of fetal cord blood and serum. Care should be exercised to use sterile materials and not contaminate the samples or inside of the vials or caps with materials from other subjects, personnel, or material in the blood preparation environment. After the cord blood has been aliquoted place the tubes either on dry ice or at or below -80°C CHAPTER 8: Post-Partum Obstetric Data Collection 09/13/06 Page 8 - 7 If the amount of cord blood available is insufficient for 0.7 mLs aliquots in the serum and whole blood vials (351-353 and 551-552) the blood should be collected in the red top or SST tube. With gloved hands open the GeneMatch™ sticks. Making sure to not touch the wicking points tear the plastic sticks in half so that there are two sections of four sticks each. Then tear the one of the sections of four sticks in half again so that there are two sets of two sticks. Dip the sets of two sticks into the blood in the SST tube, wicking up blood on the white wicking points. The wicking sticks should be inserted into the blood long enough for the white wicking surface to be coated with blood- but not for an extended period of time. Place the collection sticks on a hard surface and allow them to air dry. Once they are dry, put one set of 2 sticks into the lavender tube #551 and the other set of 2 sticks in the lavender tube # 552 (from packet number 5) With the remaining blood centrifuge as instructed directly above and aliquot the blood into tubes 351-353. If there is not enough blood to aliquot all three tubes it is important to put a full aliquot into tube # 351 before aliquoting into tubes #352 and #353. Fill tube #352 and #353 as the serum allows. If it is not possible to collect all three tubes of serum make a note in the comments section of the POS indications which vials contain a sample and which ones are empty. Care should be exercised to use sterile materials and not contaminate the samples or inside of the vials or caps with materials from other subjects, personnel, or material in the serum preparation environment. Once the serum has been aliquoted into the 4 bar-coded tubes (making sure to match the first 6 digits of the barcode number on the tubes with the number on the SST collection tube) make sure an identifying paperwork label that matches is affixed to the POS specimen collection form. After the serum and cord blood has been aliquoted place the tubes either on dry ice or at or below -80°C. 8.4.3. Labor and Delivery Form (LDF) The Labor and Delivery Form (LDF) should be completed as soon as possible after the delivery, while the participant is still in the hospital. The form is completed from a thorough review of the participant’s medical records. Events that occur during delivery that are recorded in the medical records might also trigger the need for a Serious Adverse Event Form (SAE) and the required reporting (See Chapter 10 of the MOTOR MOP). Labor and Delivery Data Form ID: ___ ___ ___ ___ ___ ___ ___ ___ Form: LDF Ver: A Visit #: 04 Name: _________________________ Staff ID: __ __ __ Date: __ __ / __ __ / 20__ __ 13. Type of Labor (circle one): 1 = No Labor ADMISSION 1. Date of Admission: __ __/__ __/2 0 __ __ 2. Hospital if not study site: _________________________ CURRENT PREGNANCY HISTORY 3. Last weight measured prior to delivery: (in kg or lb) a) __ __ . __ kg or __ __ __ . __ lb b) Date weighed: __ __ / __ __ / 20 __ __ 4. Hypertension If YES, circle type 5. Pyelonephritis? Y N U 6. 3 Trimester vaginal bleeding? Y N U 7. Polyhydramnios? Y N U 8. Abdominal surgery? Y N U 9. HIV tested? If YES, circle result: Y N U Y N U 1 = chronic (no meds) 2 = pregnancy Induced If YES, highest BP: SBP: __ __ __, DBP: __ __ __ rd 1 = Positive 2 = Negative 3 = Unconfirmed 10. Infections or sexually transmitted diseases noted in charts? Y N U If YES, indicate diseases noted and if treated: a) GC Y N U Treated: Y N U b) GBS Y N U Treated: Y N U c) HSV Y N U Treated: Y N U d) VDRL Y N U Treated: Y N U e) Chlamydia Y N U Treated: Y N U f) Sym BV Y N U Treated: Y N U 11. Meds during Pregnancy including labor? Y N U If YES, indicate below: a) Tocolytic for pre-term labor Y N U b) Magnesium Sulfate Y N U c) Antibiotic Y N U If YES, specify: 1. __________________________ 2. __________________________ d) Metronidazole Y N U If YES, 1. date: __ __ / __ __ / 20 __ __ 2. Indication: _________________ e) Steroids for fetal lung maturation Y N U f) Progesterone for PTB prevention Y N U LABOR and DELIVERY 12. Membrane Rupture: 1 = spontaneous 2 = artificial a) Date: __ __/__ __/20 __ __ b) Time: __ __ __ __ (24 hr) CHAPTER 8: Post-Partum Obstetric Data Collection Seq #: 01 Instructions: Complete this form for all randomized participants based on delivery chart review. Answer all questions. 09/13/06 2 = Spontaneous 3 = Spontaneous, augmented 4 = Induced 5 = Unknown IF 2, 3, or 4, Date and time (24hr) of labor onset: a) Date: __ __/__ __/20 __ __ b) Time: __ __ __ __ 14. Febrile During Labor? Y N U If YES, a) Maximum Temperature __ __ __ . __°F b) Date of onset __ __/__ __/ 20 __ __ c) Time of onset (24hr) __ __ __ __ 15. Date and Time (24 hr) of Delivery: a) Date: __ __/__ __/20 __ __ b) Time: __ __ __ __ 16. Type of Delivery: 1 = Vaginal 2 = Cesarean 3 = Unknown 17. Delivery classification (circle one) 1 = Delivery > 37 weeks 0 days 2 = Spontaneous preterm labor with delivery → SAE 3 = PROM leading to spontaneous preterm delivery → SAE 4 = PROM leading to preterm induction/C-section → SAE 5 = Fetal indications 6 = Maternal indications 7 = Unknown 18. Check all conditions occurring. a. None b. Chorioamnionitis c. d. Abruption Previa e. f. Fetal distress IUGR (EFW<10%) g. h. Fetal death Preeclampsia i. j. Oligohydramnios (afi<5cm) Other ________________________ 19. Anesthesia at Delivery (circle one) 1 = none 6 = Epidural 2 = local 7 = Caudal 3 = Spinal/Saddle 8 = General 4 = Paracervical 9 = Other ________________ 5 = Pudental 10 = Unknown 20. Cord arterial gas? If YES, pH: ___.___ ___ Y N U base excess: ___ ___ ___.___ 21. Date of discharge __ __/__ __/ 20 __ __ Page 8 - 8 8.4.4. Neonatal Baseline Form (NBF) The Neonatal Baseline Form (NBF) captures the primary outcome data for the MOTOR study, date of birth and birth weight. Data is collected from a thorough review of the participant’s labor and delivery medical records. Some events will trigger the need for a Serious Adverse Event Form (SAE) and require reporting. Examples include stillbirths, intrauterine fetal demise, neonatal death, miscarriages, Neonatal Intensive Care Unit admission, or, for some birth anomalies. (For details on reporting serious adverse events, see Chapter 10 of the MOTOR MOP). Neonatal Baseline Form ID: ___ ___ ___ ___ ___ ___ ___ ___ Form: NBF Ver: A Visit #: 04 Name: _________________________ Staff ID: __ __ __ Date: __ __ / __ __ / 20__ __ Seq #: 01 Instructions: Complete this form for every baby/fetus, form is identified using maternal (participant) ID number. 1. Live or stillbirth (circle one) 1 = Live birth 2 = Antepartum stillbirth/miscarriage complete SAE form 3 = Intrapartum stillbirth Date of Diagnosis __ __/__ __/ 20__ __ complete SAE form 2. Pediatric estimate of gestational age ___ ___ wks 3. Sex (circle one) 1 = Male 2 = Female 4. Birth weight ___ ___ ___ ___ gms 5. Head circumference ___ ___ . ___ cm 6. Length ___ ___ . ___ cm 7. APGAR scores a. 1 minute b. 5 minutes ___ ___ ___ ___ 8. Fetal congenital abnormalities? Y N IF YES, specify anomalies and complete SAE form: a) _______________________________________________________________________ b) _______________________________________________________________________ c) _______________________________________________________________________ 9. Highest level of care required (circle one) 1 = N/A (stillbirth or neonatal death in L&D) complete SAE 2 = Well baby nursery/routine care Discharge date __ __/__ __/20__ __ 3 = NICU / Intermediate nursery complete NIC form 4 = Baby birthed at home, no hospitalization Neonatal Intensive Care Form 8.4.5. Neonatal Intensive Care Form (NIC) ID: ___ ___ ___ ___ ___ ___ ___ ___ Form: NIC Ver: B Visit #: 04 Name: _________________________ Staff ID: __ __ __ Date: __ __ / __ __ / 20__ __ Seq #: 01 Instructions: Complete this form for each live born infant admitted to the NICU/Intermediate care nursery. Admission of an infant to the Neonatal Intensive Care Unit during the Mother’s hospital stay is considered a Serious Adverse Event. An SAE form must be completed and all the reporting procedures must be followed. The Neonatal Intensive Care Form is competed from a thorough review of the infant’s medical records. The NIC is a checklist of the infant’s potential conditions and/or diagnoses. Conditions from this list, which are documented in the infants’ medical record/chart, should be indicated on the NIC. 1. Date of NICU admission: __ __/__ __/__ __ 2. Hospital Name if not study site: ____________________________________ 3. Neonatal Blood Gas Done? If YES: a) First neonatal arterial pH Y N ____ .___ ___ b) First base excess ___ ___ ___ .___mEq/l 4. Total Bilirubin Done? If YES: a) Highest total bilirubin: b) Date: Y N __ __.__mg/dl 17. Patent ductus arteriosus requiring medical or surgical treatment? Y N 18. Persistent pulmonary hypertension? Y N 19. Proven sepsis? Y N 20. Suspect sepsis? Y N 21. Cranial sonogram or CT performed? Y N If YES, Most severe Grade IVH? (circle one) 0 = None 1 = Grade I 2 = Grade II 3 = Grade III 4 = Grade IV __ __/__ __/__ __ c) Time: __ __:__ __ 22. PVL? Y N 23. Other Intracranial hemorrhage? Y N 24. Seizures? Y N 25. Retinopathy of Prematurity? Y N 26. Transferred from birth hospital NICU? Y (If sent to Chronic Care, answer No) N 5. Transient tachypnea (TTN) ? Y N 6. Respiratory Distress Syndrome? Y N 7. Pneumonia? Y N 8. Bronchopulmonary dysplasia? Y N Y N IF YES: a. Specify where baby was transferred (circle one): 10. Respiratory Support? Y If YES, check all that apply: a. High Frequency ventilation? N 1 = Birth hospital, another unit 2 = Transferred to another hospital, NICU 3 = Transferred to another hospital, non-NICU (O2 at 28 days)? 9. Chronic Lung disease? (O2 at 36 wks adj. b. Date of Transfer: b. Conventional Mechanical Ventilation? c. Nasal CPAP? 1 = Outcome unknown d. Supplemental Oxygen? 11. Duration of ventilator support: __ __/__ __/__ __ 27. Final status of Infant? (circle one) 2 = Died before final discharge _____days 12. Duration of supplemental oxygen _____days 3 = Transferred to Chronic care facility 4 = Discharged home 13. Received Surfactant? Y N a) If discharge/transferred: date __ __/__ __/20 __ __ 14. Received Indomethacin? Y N b) If died: → complete SAE 15. Pneumothorax? Y N 16. Necrotizing enterocolitis? IF YES, treatment required? Y Y N N 1. Cause of Death: ______________________________ CHAPTER 8: Post-Partum Obstetric Data Collection 09/13/06 2. Date __ __/__ __/20__ __ 3. Time (24hr) __ __:__ __ Page 8 - 9