Hyperadrenocorticism (HAC)
advertisement
")
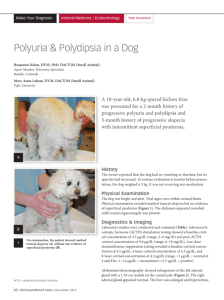
Does this dog have Cushing’s disease? Linda E. Luther, DVM, DACVIM (SAIM) Small Animal Track 2012 ISVMA Annual Conference Proceedings Hyperadrenocorticism (HAC) Two natural forms, one iatrogenic Pituitary-dependent HAC (PDH) (80-85%) o Functional tumor in pituitary gland o Endogenous ACTH levels are inappropriately elevated o Bilateral adrenal gland hyperplasia results Adrenal tumor (AT) (15-20%) o Referring to an adrenal cortical tumor vs. pheochromocytoma o Not always functional o 10% are bilateral o Half are a benign adenoma, half a malignant adenocarcinoma o Approximately half of all tumors mineralize Iatrogenic o Due to chronic exogenous glucocorticoid administration o Parenteral or topical Clinical signs of all three forms similar Clinical signs/PE findings (All may not be present): PUPD Alopecia/hyperpigmentation Pot-bellied appearance Hepatomegaly Polyphagia Muscle weakness Panting Obesity CBC, chemistry, bile acids Neutrophilia, monocytosis, lymphopenia Elevated ALP (85-95%) Mild increase in ALT Elevated cholesterol, triglycerides 10% become diabetic Bile acids may be mildly elevated Urinalysis Specific gravity is often less than 1.015-1.020 May be able to concentrate up to 1.025-1.035 Proteinuria is often present 46% have UTI (sediment may be inactive) Other clinical findings Hypertension Proteinuria Thromboembolism CUSHING’S DISEASE IS A CLINICAL VS. LABORATORY DIAGNOSIS IF THE DOG DOES NOT HAVE CLINICAL SIGNS THAT ARE SUGGESTIVE OF HAC, ADRENAL TESTING IS NOT RECOMMENDED. TEST RESULTS MAY BE MISLEADING IF SIGNIFICANT NONADRENAL DISEASE IS PRESENT. Screening tests Low dose dexamethasone suppression test (LDDS) o 85-95% sensitive; 70-75% specific o May also diff b/w PDH and AT o > 1.4 μg /dL at 8 hrs: Consistent with hyperadrenocorticism ACTH stimulation test o <60-85% sensitive;85-90% specific Urine cortisol:creatinine ratio o 97% sensitive; 20% specific CRH ACTH LDDS vs. ACTH stim More sensitive Lower cost Might ddx PDH v.s AT ACTH stim indications Iatrogenic HAC Monitoring HAC tx Dx hypoadrenocorticism CORTISOL Once a diagnosis of HAC confirmed, these tests differentiate between PDH and AT LDDS o 60% of PDH dogs have suggestive results (suppression at 4 h, but not at 8 h) o Suppression = < 1.4 μg/dL at 4 hrs < 50% baseline at 4 hrs < 50% baseline at 8 hrs HDDS o No suppression at 8 hours: 100% AT, 25% PDH Endogenous ACTH level o < 20 pg/mL suggests AT o > 45 pg/mL suggests PDH o 20-45 pg/mL is nondiagnostic Abdominal ultrasound o Rules out adrenal diseases, rules out nonadrenal disease o Dogs with PDH may (or may not) have enlarged adrenal glands CT/MRI Cases: Do these dogs have Cushing’s disease? 1. 8-year-old Fs Dachshund. History of PUPD. PE: BCS 8/9, pot-bellied, ventral alopecia. ALP 4x normal, Uspgr 1.035. LDDS pre: 6.8 μg/dL; 4 hr post: 1.0 μg/dL; 8 hr post: 1.7 μg/dL. 2. 7-yr-old Fs Boxer. History of PUPD. PE: BCS 8/9, pot-bellied, ventral alopecia. ALP 6x normal, Uspgr 1.020. LDDS pre: 6.8 μg/dL; 4 hr post: 6.2 μg/dL; 8 hr post: 6.2 μg/dL. Ultrasound appearance of adrenal glands: Right adrenal gland irregular in contour, oval-shaped, measures 3 x 6 cm. Left adrenal gland small. 3. 10-yr-old Mn Poodle. Presented for dental cleaning. No clinical complaints. PE: BCS 4/9, Grade 2 dental disease. Pre-anesthetic blood work showed ALP 10x normal. LDDS pre 9.3 μg/dL; 4 hr post 3.0 μg/dL; 8 hr post 2.6 μg/dL. 4. 7-year-old Fs Pug. History of PUPD. PE: BCS 8/9, pot-bellied. ALP 6x normal, Uspgr 1.020. LDDS pre: 7.0 μg/dL; 4 hr post: 5.0 μg/dL; 8 hr. post: 4.0 μg/dL. Ultrasound appearance of adrenal glands: Normal shape, cranial and caudal poles of both left and right adrenal glands = 0.8 cm. 5. 10-year-old Mn Bassett hound. History PUPD, polyphagia. PE: BCS 9/9, pot-bellied, thin hair coat. ALP 5x normal, ALT 2x normal, Uspgr 1.018. LDDS pre: 5.0 μg/dL; 4 hr post: 4.9 μg/dL; 8 hr. post: 4.0 μg/dL. Ultrasound appearance of adrenal glands: Both left and right adrenal glands round in shape, 2 cm in diameter. Endogeneous ACTH 32 pg/dL (> 45 pg/dL = PDH). 6. 7-yr-old Fs Lab. Three-month history of PUPD, polyphagia and weight loss. PE: BCS 7/9. ALP 6x normal, hyperglycemia (410 mg/dL), 3+ glucosuria, Uspgr 1.015. LDDS pre: 6.8 μg/dL; 4 hr post: 6.2 μg/dL; 8 hr. post: 6.2 μg/dL. 7. 8-year-old Mn Scottish Terrier. No clinical signs. PE: BCS 6/9. Senior wellness blood work revealed ALP 8x normal. Bile acid assay WNL. 8. 10-year-old Mn Boston Terrier. History of vomiting and weight loss. PE: BCS 4/9. ALP 10x normal, Uspgr 1.020. Urine cortisol/creatinine ratio 30 (normal 8-24). 9. 8-year-old Fs Cavalier King Charles spaniel. History of PUPD and anorexia. PE: BCS 5/9. ALP 7x normal, ALT 12x normal, Uspgr 1.026. 10. 9-year-old Mn Pomeranian. History of truncal alopecia. PE: BCS 7/9, sparse hair coat. ALP 4x normal, Uspgr 1.020. LDDS pre: 3.0 μg/dL; 4 hr post: < 0.5 μg/dL; 8 hr. post: < 0.5 μg/dL. Diagnosis of hyperadrenocorticism references Cook AK, Bond KG. Evaluation of the use of baseline cortisol concentration as a monitoring tool for dogs receiving trilostane as a treatment for hyperadrenocorticism. J Am Vet Med Assoc 2010;237:801-805. Forrester SD et al. Retrospective evaluation of urinary tract infection in 42 dogs with hyperadrenocorticism or diabetes mellitus or both. J Vet Intern Med 1999;13(6):557. Graham J, Adrenal glands, In Atlas of Small Animal Ultrasonography, Penninck D, d’Anjou M (eds), Blackwell Publishing, Ames, IA, 2008, pp. 385-396. Grooters AM et al. Ultrasonographic characteristics of the adrenal glands in dogs with pituitary-dependent hyperadrenocorticism: Comparison with normal dogs. J Vet Intern Med 1996;10:110-115. Helm JR, Mclauchlan G, Boden LA, Frowde PE, Collings AJ, Tebb AJ, Elwood CM, Herrtage ME, Parkin TDH, Ramsey IK. A comparison of factors that influence survival in dogs with adrenal-dependent hyperadrenocorticism treated with mitotane or trilostane. J Vet Intern Med 2011;25:251-260. Mamelak AN, Bruyette D, Owen TJ. Endoscopic transsphenoidal pituitary surgery. Proc Am College Vet Intern Med 2010. Melián C, Pérez-Alenza MD, Peterson ME, Hyperadrenocorticism in dogs. In Ettinger SJ, Feldman EC (eds.) Textbook of Veterinary Internal Medicine, 7th ed. Saunders Elsevier, St. Louis, 2010, pp. 1816-1840.