Use - Bakersfield College
advertisement

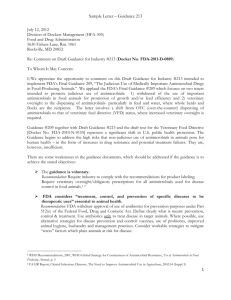
Exercise 12 – Controlling Microorganisms with Antimicrobials 1 Exercise 12 – Controlling Microorganisms with Antimicrobials 5. 6. 7. 8. Objectives 1. Discuss factors effecting chemotherapeutic agent effectiveness. 2. Compare and contrast narrow and broad spectrum drugs. 3. Use the Sanford guide to identify antibiotic uses and side effects. 4. Describe the major mechanism of actions for antibiotics. Perform a Kirby Bauer test for antimicrobial sensitivity and interpret zone sizes correctly. Evaluate sensitivity results with regards to clinical applications. Explain the characteristic antibiograms of bacterial species, particularly those highly resistant forms (MRSA, VRE, ERBL, and MDRTb). Analyze the presence of resistant and contaminating organisms during the testing procedure. Our lives have been greatly affected by the use of antimicrobial agents used in the treatment of infections. Agents produced by living organisms, such as bacteria or fungi, that inhibit or kill microorganisms are called antibiotics. Some antimicrobials are synthetically produced and altered, resulting in chemical variations referred to as generations of drugs. For instance, cephalosporin’s are now in their fourth generation (refer to the Sanford guide) each alteration enhances the activity of the drug by some means. Several factors impact the effectiveness of these chemotherapeutic agents: organism type method of use - absorbed (topical), ingested (P.O.), or injected (I.V. or I.M.) antimicrobial tissue concentration toxicity level interaction with other agents (synergy or inhibition) mode of action - lethal (-cidal) or inhibiting (-static) microbial resistance The activity of antimicrobials is usually specific, limited to bacteria, viruses, or fungi, usually not combinations of microbes. Susceptibility patterns (antibiograms) are so specific that they can be used to confirm the identity of many species of bacteria. The action of these substances targets metabolic functions in the organism. The best antimicrobials attack prokaryotic functions and have little or no effect on eukaryotic cells and are ineffective with viruses. However in some cases, antibiotics may be toxic to a particular tissue in humans or may cause other complications such as allergic reactions or disruption of normal flora. While antibiograms are fairly consistent, resistance factors carried on plasmids often result in geographically unique species with increased resistance to specific antibiotics. While physicians often treat empirically, the only way to know a specific antimicrobial’s effectiveness is to test it against the specific pathogen isolated form the infection. Labs test the true effectiveness of these substances by dilution tests, called Minimum inhibitory concentrations (MIC) in order to provide the physician with the most complete information available. Today most of these tests are automated and interpreted by computers. Our experiment will involve a simpler test, called the Kirby Bauer test, using sterilized filter discs that have been commercially impregnated with a given concentration of antimicrobial, placed upon a lawn culture of 3 different types of bacteria. Three species of bacteria will be studied for antimicrobial inhibition. Exercise 12 – Controlling Microorganisms with Antimicrobials 2 Susceptibility to these agents is often under genetic control and in recent years the most pathogenic organisms are the ones that have gained resistance to our antimicrobial agents. Various genes for resistance are carried on plasmids in bacteria, and therefore, easily transferred. MRSA (methicillin resistant Staph. aureus) plague hospitals and convalescent homes where the pressure to select for the survival of these organisms is strongest. In some cases there are organisms resistant to even the newest generations of drugs produced. It is the race against these organisms that drives antibiotic prices higher, and mandates the testing of every pathogen's susceptibility to a variety of antimicrobials rather than relying on a standard treatment. Materials and Methods: 3 Kirby Bauer plates (per group) 4 antimicrobial discs lab disinfectant discard beaker 6 sterile cotton swabs 3 sterile water McFarland dilution standard STOCK CULTURES: Staphylococcus aureus Pseudomonas aeruginosa E. coli forceps Bunsen burner First Lab Session 1. Put on your PPG and use eye protection for this lab. 2. Label 3 sterile water tubes and 3 Kirby Bauer plates for each stock culture Staphylococcus aureus, Pseudomonas aeruginosa, & E. coli. 3. Using a sterile swab and aseptic technique, prepare a standard concentration of each of the stock cultures in the sterile water tube by comparing them to the McFarland standard. (Refer to lab 5). 4. Dispose of the swab in a small beaker of disinfectant. 5. Using a fresh sterile swab dipped one time in the standardized concentration of stock culture produce a LAWN culture. 6. Use the antimicrobial dispenser to apply the discs to the three plates. Each stock will be tested for the same antimicrobials. Note that the discs are labeled. Use the forceps to gentle tap the disc down, sterilize forceps in the incinerator. 7. On the table list the names and concentration of each antimicrobial. Look them up in the Sanford Guide and indicate key information about each. 8. Incubate these plates at 35C for 24 hours. 9. Replace equipment, discard stock cultures & contaminated materials as biohazards. Hospitals are required to collect the data concerning their specific isolates and their sensitivity each year and we refer to this pattern of resistance and sensitivity as the antibiogram. This data is made available to the physician's so that they can begin early treatment empirically. The antibiograms are specific to geographic regions and even individual hospitals within an area. The following antibiogram is used with permission of Kern Medical Center Microbiology Lab; please refer to following link KMC 2006 Antibiogram. N= the number of total isolates of that species of bacteria in the previous calendar year. The numbers for each species below the antibiotic represents the percent of sensitive isolates for that species to that specific antibiotic. For instance, only 44% of the E.coli isolated in during 2005 were sensitive to Ampicillin. The KMC antibiogram was determined by computerized techniques on a Vitek machine. We are using the standard Kirby Bauer disk diffusion technique but the results are comparable. Exercise 12 – Controlling Microorganisms with Antimicrobials 3 The diameter of the zone of inhibition is measured in millimeters and then interpreted using the chart below. Interpretation of the zone size depends upon the concentration of the antibiotic and the type of organism. When the lab reports out sensitivity results they will describe an organism as resistant, intermediate, or sensitive when doing a Kirby Bauer Sensitivity. In other cases a Minimum Inhibitory Concentration (MIC) will be reported indicating the smallest concentration that can be used to inhibit the growth of the organism. Use the chart below to interpret the zone sizes for the organisms tested in this lab. Antimicrobial Interpretation Chart Disc Antimicrobial Agent AM 10 Ampicillin 10mcg Gram Negative Staphylococci Enterococci Streptococci (not S. pneumoniae) Haemophilus sp. Listeria monocytogenes Methicillin 5mcg Staphylococci Penicillin 10 units Gram Negative(E.coli) Staphylococci Enterococci Streptococci(not S. ME5 P10 Resistant Intermediate Lactams - Penicillins Sensitive 13 28 16 21 14-16 18 19 19-21 22 20 9 10-13 14 13 28 14 19 14-16 17 29 15 28 Neisseria gonorrhea Listeria monocytogenes 26 19 27-46 47 20 Pipericillin 100mcg P. aeruginosa 17 17 18-20 21 18 22-29 20-27 17 29 17 30 pneumoniae) PIP100 AMC30 SAM20 CEC30 CFP75 CTX30 CRO30 CXM 30 FOX 30 IMP10 Lactam/Lactamase Inhibitors Amoxicillin 20mcg/Clavulanic Acid 10 mcg Staphylococci 19 Other organisms 13 14-17 Ampicillin 10mcg/Sublactam 10mcg Gram Negative enterics & 11 12-14 staph Cephalosporins Cefaclor 30 mcg 14 15-17 Haemophilus sp. 16 17-19 Cefoperazone 75 mcg 15 16-20 Cefotaxime 30 mcg 14 15-22 Ceftriaxone 30 mcg 13 14-20 Haemophilus sp N. gonorrhea 18 20 21 23 21 26 35 Cefuroxime 30 mcg Cefoxitin 30 mcg 15-17 15-17 18 18 14-15 16 Impenem 10mcg 14 14 Carbapenems 13 20 18 15 Exercise 12 – Controlling Microorganisms with Antimicrobials Disc Antimicrobial Agent Haemophilus sp Resistant VA30 Vancomycin Enterococci Other Gram Positives S. pneumoniae 4 Intermediate Sensitive 16 15-16 10-11 17 12 17 13-14 15 14-17 11-12 17-20 18 13 21 13 15 13 14-22 16-20 14-17 13 14-17 23 21 18 12 18 13-15 15-18 26-28 31-37 18-21 16 19 29 38 22 16-20 19-21 13-16 21 21 36 22 17 9-12 13-17 13 18 20 14 10 10 15-16 11-15 11-15 21 17 16 16 10 15 11-15 16-18 16 19 Glycopeptides GM10 Gentamicin 10mcg CLR15 Clarithromycin 15 mcg Haemophilus sp S. pneumoniae E15 Erythromycin 15 mcg S. pneumoniae Azithromycin Haemophilus sp S. pneumoniae AZM15 DO30 TE30 Doxycycline 30 mcg Tetracycline 30 mcg Haemophilus sp N. gonorrhea S. pneumoniae CIP5 Ciprofloxacin 5mcg Haemophilus sp N. gonorrhea Lomefloxacin 10 mcg Norfloxacin 10 mcg LOM10 NOR10 B10 C30 FD 300 TMP 5 SxT 14 9 Aminoglycosides 12 Macrolides 13 10 16 Bacitracin 10 units Chloramphenicol 30mcg S. pneumoniae Nitrofurantoin 300mcg Trimethoprim 5mcg Trimethoprim1.25mcg/ Sulfamethoxazole 23.75mcg Haemophilus S. pneumoniae Tetracyclines 12 14 25 30 17 Quinolones 15 18 12 Others 8 10 List of Antibiotics typically available in lab Amikacin Ampicillin Ampicillin/Sublactam (Synercid) Amoxicillin/Clavulanic Acid (Augmentin) Ceftriaxone (Rocephin) Cefoperazone (Cefobid) Cefuroxime (Zinacef) Chloramphenicol Clindamycin Nitrofurantoin (Macrodantin) Oxacillin or Nafcillin Pipercillin Penicillin Quinupristin (Synercid) Exercise 12 – Controlling Microorganisms with Antimicrobials Azithromycin Bacitracin Cefaclor (Ceclor) Cefazolin (Ancef, Kefzol) Cefixime (Suprax) Ciprofloxacin Doxycycline Erythromycin Gentamicin Lincomycin Nafcillin (Unipen) or Oxacillin 5 Sulfamethoxazole trimethoprim (SXT-Bactrim) Tetracycline Unasyn Vancomycin Lab Report #12 Name________________________ 1. Data Chart Record the zone of inhibition by measuring the diameter in millimeters and referring to the interpretation chart, write S (for sensitive), I (for intermediate), or R (for resistant) next to the measured results. Antimicrobial Concentration Staphylococcus aureus mm Interp Pseudomonas aeruginosa mm Interp. Escherichia coli mm Interp. Exercise 12 – Controlling Microorganisms with Antimicrobials 6 NOTE: The size of the diameter can not be compared between organisms and antibiotics because the concentration of the antibiotics is different. Exercise 12 – Controlling Microorganisms with Antimicrobials 2. Refer to the text, Sanford guide or Prescription Drug Guide for the antimicrobials below and their mode of action. Antimicrobial Mode of Action Drugs in the same family Precautions & Warnings Penicillin Any Cephalosporin Ciprofloxacin Erythromycin Tetracycline Trimethosulfa (Bactrim, SXT) 3. Using the interpretation chart decide which antibiotic would be most effective against Staph aureus who’s zone sizes are: Penicillin 25mm, Ampicillin 26mm, Methicillin 18mm 4. Is the above organism an MRSA? Why or why not? 7 Exercise 12 – Controlling Microorganisms with Antimicrobials 8 5. At KMC the number of MRSA isolates in 1970 was nearly zero. But over the years, the number of MRSA isolates has increased to 65% out of 1719 isolates. Look at the increase in MRSA isolates at these North Carolina Hospitals. What are the implications of the data? Table 1. Streptococcus pneumoniae susceptibility to nine antimicrobial agents, North Carolina, 1996–2000 % of all susceptible isolates Year Penicillin Erythromycin Cefotaxime Levofloxacin Tmpsmxb Tetracycline Clindamycin Vancomycin Chloramphenicol 1996 65 78 85 100 64 96 90 100 93 1997 63 69 80 100 57 79 76 100 95 1998 56 64 83 92 51 83 88 100 89 1999 54 61 80 94 51 84 85 100 92 2000 52 61 77 98 50 81 88 100 94 b Tmp-smx, trimethoprim-sulfamethoxazole 6. What do you think explains the increase in MRSA across the United States? Exercise 12 – Controlling Microorganisms with Antimicrobials 7. How would you explain a zone where there are a few colonies of organisms growing within an apparent area of inhibition? As seen in the top two zones on this sensitivity 8. Antibiotics that affect the growth of both gram negative and gram positive organisms are referred to as broad spectrum antibiotics because they affect a wide variety of organisms. Antibiotics affecting only gram negative organisms or only a few families of organisms, are referred to as narrow spectrum antibiotics. Why wouldn't a physician use a broad spectrum antibiotic to treat an infection and save the patient the time and money involved in culturing and testing for sensitivities? For another sample antibiogram see http://www.ohsu.edu/pharmacy/DraftAntibiogram2004.pdf#search='antibiogram' For antibiotic resistance http://www.microbeworld.org/htm/cissues/resist/resist_0.htm http://www.cdc.gov/Ncidod/eid/vol9no2/02-0123.htm Date last updated 2/18/2016 ©Janet Fulks 9