Diabetes-Plan - Jackson County School District
advertisement

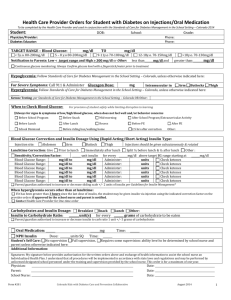
Dr. Michael Van Winkle Assistant Superintendent Michelle Thomas, RN, BSN School Nurse Jackson County School District St. Martin Attendance Center 11300 Yellow Jacket Blvd * Ocean Springs, MS 39564 Phone 228-875-8418 ext. 612 Fax 228-875-8426 DIABETES ACTION PLAN Student Information: Name of student: _______________________________________________ DOB: _______________________ Grade: ______ Classsroom Teacher/1st Period Teacher: ________________________________________________ Physical Education Days and Times: _______________________________________________________________ Emergency Information: Parent/Guardian Name: _____________________________________________ Phone (H) ___________________ Address: __________________________________________________ Phone (W) ___________________ Parent/Guardian Name: _____________________________________________ Phone (H) ___________________ Address: __________________________________________________ Phone (W) __________________ Physician’s name: _______________________________________________Telephone: _____________________ In case of emergency, contact: 1. ___________________________________________________________________________________________ 2. ___________________________________________________________________________________________ 3. ___________________________________________________________________________________________ TO BE COMPLETED BY PHYSICIAN: Target range of blood glucose: _______________________________ Specific dietary guidelines Meal/snack times: Breakfast ______________ AM snack _____________________ Lunch __________________ PM Snack _______________ Dinner ______________________ Bed ____________________ Blood glucose testing at school This student is able to test his/her own blood glucose? __________ Yes __________ No Dr. Michael Van Winkle Assistant Superintendent Michelle Thomas, RN, BSN School Nurse Adult supervision required? __________ Yes __________ No Method to be used Type of meter _____________________________________ Test strip required __________________________________ Routine testing times at school __________AM __________ Noon __________ PM Supplemental testing times: _____ before exercise _____ after exercise _____before snacks _____ with symptoms of high/low blood glucose Other _______________________________ Insulin at school _____ not at all _____ routine lunchtime dose _____ correction lunchtime dose If insulin is required at school Brand name and type: ____________________________________________________ Dose preparation by: _____ Student _____ Parent _____ Parent designee _____ Licensed nurse Number of SQ or insulin pump units determined by: _____ Student Form used: _____ Pre-filled syringe _____ Insulin pen _____ Insulin pump _____ Licensed nurse _____ Parent (telephone request acceptable) Written sliding scale as follows: Blood glucose from __________ mg/dl to __________ mg/dl = __________ units of insulin Blood glucose from __________ mg/dl to __________ mg/dl = __________ units of insulin Blood glucose from __________ mg/dl to __________ mg/dl = __________ units of insulin Blood glucose from __________ mg/dl to __________ mg/dl = __________ units of insulin SQ or insulin pump insulin administered by: _____ Student _____ Parent _____ Parent designee _____ Licensed nurse _____ Student with staff verification of the number of prescribed insulin units (all parent designees are trained by the parent and are not employees of the school or district) Specific sports/exercise guidelines: 1. This student may participate in daily PE? _____ Yes _____ No 2. After school sports? _____ Yes _____ No 3. Activity restrictions: _____ None _____ Other _________________________________ 4. Exercise should be delayed or avoided if blood glucose is higher than __________ mg/dl or lower than __________mg/dl. Treatment of LOW BLOOD GLUCOSE: (See signs & symptoms of low blood glucose) Low blood glucose must be treated immediately. An adult must stay with student until all signs and/or symptoms of low blood glucose are gone and blood glucose is 70mg/dl or higher. THIS IS AN EMERGENCY. IMMEDIATE TREATMENT IS NEEDED. This student’s blood sugar is considered low if __________ mg/dl or lower. Dr. Michael Van Winkle Assistant Superintendent Michelle Thomas, RN, BSN School Nurse If the student is conscious and able to swallow give one of the following: ITEM __________________________ __________________________ AMOUNT _________________________ _________________________ If the student is less cooperative then give one of the following: ITEM AMOUNT __________________________ __________________________ ROUTE _________________________ _________________________ _____________________ _____________________ If student begins to lose consciousness or is having a seizure, call 911 and parents immediately. If present and ordered by the physician, the school nurse may administer glucagon emergency kit. _____ Yes _____ No Treatment of HIGH BLOOD GLUCOSE (See signs & symptoms of high blood glucose) 1. 2. 3. 4. The student is hyperglycemic if blood glucose is above __________ mg/dl. Are urine ketones to be check at school? _____ Yes _____ No Check urine ketones if glucose is above _____ mg/dl _____ by student independently _____ with assist. Notify parents or physician if ketones are positive or when _________________________ Additional actions to be taken: (see insulin at school section) _____________________________ ______________________________________________________________________________. In the event of field trips, all diabetic supplies are taken and care is provided according to the Action Plan (a copy if taken on trip) In the event of classroom/school parties, food treats will be handled as follows: _____ Student will eat the treat _____ Put in baggie and take home with teacher note _____ Replace with parent supplied alternative _____ Modify treat as follows _______________ 3 day disaster diabetes supplies are recommended: _____ vial of insulin, 6 syringes _____ Glucagon kit _____ insulin pen with cartridge and needles _____ ketone strips/plastic cup _____ glucose gel product and glucose tablets _____ snack supply _____ blood glucose testing kit (testing strips lancing device with lancets) PARENT CONSENT FOR DIABETES MANAGEMENT IN SCHOOL The undersigned parent/guardian of the above-named student request that the specialized physical health care service for management of diabetes in school is administered to student. Parent will provide the necessary supplies and equipment, notify school if there is a change in student health status or attending physician and notify the school nurse immediately and provide new consent for any changes in doctor’s orders. I authorize the school nurse to communicate with the physician when necessary. Parent/Guardian Signature _________________________________________ Date ________________________ Dr. Michael Van Winkle Assistant Superintendent Michelle Thomas, RN, BSN School Nurse PHYSICIAN CONSENT FOR DIABETES MANAGEMENT IN SCHOOL My signature below provides authorization for the above written orders. I understand that specialized physical health care services may be performed by unlicensed designated school personnel under the training and supervision of the school nurse. The authorization is for maximum of one year. Physician Signature ___________________________________________ Date ________________________ Reviewed by School Nurse _____________________________________ Date ________________________