Van den Berghe et al
advertisement

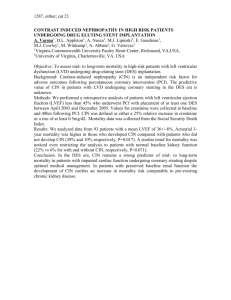
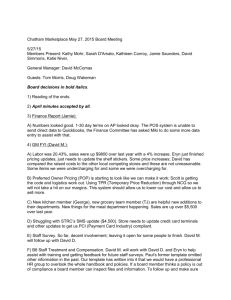
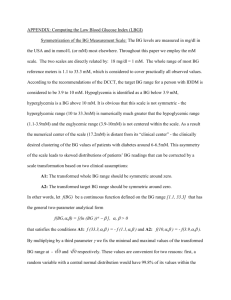
Relation between acute hyperglycemia and contrast-induced nephropathy (CIN) in patients undergoing primary percutaneous coronary intervention (PPCI) Yehia Kishk, Hamdy Soliman, Mahmoud Abdelsabour, Ahmed Mostafa Magdy. Abstract: Background: In a patient with ST-elevation myocardial infarction (STEMI), acute hyperglycemia is frequently encountered on presentation. Contrast-induced nephropathy (CIN) is also a common complication in those undergoing primary percutaneous coronary intervention (PPCI). We investigated the possible association between on-admission hyperglycemia and CIN in STEMI patients undergoing PPCI. Methods: This study included 60 patients that presented to the emergency department with STEMI who underwent PPCI. They were investigated for on-admission acute hyperglycemia defined as serum glucose > 198mg/dl, and subsequent CIN, defined as either ≥ 25% increase or ≥ 0.5 mg/dl absolute increase of on-admission baseline serum creatinine level within 4872 hours of radio-contrast administration. Results: Overall 37% of STEMI patients had acute hyperglycemia, and 35% developed CIN. Patients with on-admission hyperglycemia had 10 times the risk of developing CIN compared with normoglycemic patients. In-hospital mortality occurred more frequently in patients with acute hyperglycemia (13.6%) and CIN (14%). Patients with acute hyperglycemia that developed CIN had the highest mortality rate (21.4%). Conclusion: In STEMI patients undergoing PPCI, those with acute hyperglycemia are at high risk of CIN and in-hospital mortality. Introduction: PPCI is effective in securing and maintaining coronary artery patency. Randomized clinical trials comparing timely performed PPCI with inhospital fibrinolytic therapy have shown more effective restoration of patency, less re-occlusion, improved residual left ventricular function and better clinical outcome with primary PCI.(1) In patients undergoing PPCI, short- and long-term mortality rates were significantly higher in those who developed CIN. CIN is also associated with other post-PPCI adverse outcomes including MI and target vessel revascularization, bleeding requiring transfusion, and vascular complications).(2) Acute hyperglycemia occurs in about half of patients with STEMI, while about 25% has diabetes mellitus.(3) Acute hyperglycemia on admission has been reported to worsen the prognosis in AMI patients with and without known diabetes.(4,5) Hyperglycemia is usually due to insulin resistance and accelerated glucose production, known as ‘stress diabetes’ or ‘diabetes of injury’.(6) Several mechanisms of hyperglycemia during AMI have been postulated. These include enhanced oxidative stress, activation of blood coagulation and platelets, stimulation of inflammation, and endothelial cell dysfunction.(7) Several STEMI studies have reported that acute hyperglycemia is independently associated with acute increase in inflammatory immune markers, lower rate of TIMI flow grade 3 after primary stent implantation, "no-reflow" phenomenon, increased left ventricular dysfunction, larger infarct size, higher risk of congestive heart failure and cardiogenic shock, and increased hospital mortality.(8) Potential pathophysiologic mechanisms through which contrast administration may cause renal injury include oxidative stress, endothelial dysfunction, and apoptosis.(9) All these processes are also activated in the setting of acute hyperglycemia.(10) In the present study, we tried to examine the effect of the on-admission glucose levels and the risk of subsequent CIN in patients with STEMI who undergo PPCI. In-hospital mortality rate and other major adverse cardiac events (MACE) were also evaluated. Methods: Study population: This prospective observational study was conducted at the National heart institute, in Cairo in collaboration with the cardiology department of Assiut University, between August 2011 and November 2012. We enrolled 60 patients that presented with STEMI and underwent PPCI. Patients were included if they presented within 12 hours and 18 hours for AMI complicated with cardiogenic shock from onset of symptoms. The diagnosis of AMI was based on characteristic chest pain lasting for at least 30 minutes, not responsive to nitrates, with electrocardiographic ST-segment elevation of at least 0.1 mV in two or more contiguous leads, or new left bundle-branch block. Patients on long-term dialytic treatment were excluded. Patients with recent exposure to radiographic contrast (within two days of the study) were also excluded. Patients undergoing cardiac surgery for emergency coronary revascularization and/or mechanical complications were excluded from the analysis. The Ethical Committee of both Institutes approved the study, and written informed consents were obtained. Study design: In all patients, plasma glucose levels were assessed at hospital admission; and acute hyperglycemia was defined as glucose levels >198 mg/dl, regardless of the diabetic status.(11,12) Patients were recognized as having DM if they had a history of DM with the use of oral hypoglycemic agents or insulin. Serum creatinine concentration was measured at hospital admission, every day for the following 3 days, at discharge from the coronary care unit, and at hospital discharge. Glomerular filtration rate (eGFR) was estimated using the modified formula of cockroft, and preprocedural renal insufficiency was categorized as an eGFR <60 mL/(min 1.73 m2). Contrast-induced nephropathy was defined as an increase in creatinine >25% or an absolute increase of 0.5 mg/dl or more from the baseline value within the 72-hour period following PPCI.(13-15) Pharmacologic therapy during and after PPCI was left to the discretion of the interventional and CCU cardiologists, based on current standards of care.(16) PCI Procedure: Heparin (10,000 U) was administered after coronary anatomy was defined. Coronary artery stenosis > 70% was considered clinically significant. PPCI was performed by a 24-hours on-call interventional team. Balloon angioplasty and/or stent implantation were performed only for IRA with successful mechanical restoration of antegrade flow in all patients. A non-ionic, low-osmolality contrast agent was used and the amount of contrast used in every procedure was reported. Statistical Analysis: The collected data was revised, coded, tabulated and introduced to a PC using Statistical package for Social Science (SPSS 15.0.1 for windows; SPSS Inc, Chicago, IL, 2001). i. Descriptive statistics: 1. Mean, Standard deviation (± SD) and range for parametric numerical data. 2. Frequency and percentage of non-numerical data. ii. Analytical statistics: 1. Student T Test was used to assess the statistical significance of the difference between two study group means. 2. Correlation analysis (using Pearson's method): To assess the strength of association between two quantitative variables. The correlation coefficient denoted symbolically "r" defines the strength and direction of the linear relationship between two variables. 3. Chi-Square test was used to examine the relationship between two qualitative variables. 4. Fisher’s exact test: was used to examine the relationship between two qualitative variables when the expected count is less than 5 in more than 20% of cells. 5. Logistic regression: useful in the prediction of the presence or absence of an outcome based on a set of independent variables. It is similar to a linear regression model but is suited when the dependent variable is qualitative (categorical). -P- value: level of significance -P>0.05: Non significant (NS). -P< 0.05: Significant (S). -P<0.01: Highly significant (HS). RESULTS This study included 60 patients (48 males and 12 females) with age ranging from 27 to 85 years with a mean of 54.5±11.6 years. There were 21 hypertensive (35%) and 26 diabetic (43.3%) patients. There was no significant difference between normoglycemic and hyperglycemic patients on admission as regard risk factors, as about 55% of hyperglycemics were diabetic while about 37% of normoglycemics were also diabetics, this was statistically insignificant, as well as the other risk factors. 100% 90% 80% Percent 70% 60% 50% 40% 30% 20% 10% 0% Smoker Dyslipidaemia DM HTN IHD Risk factors Figure (1) Risk factors among patient population. Ejection fraction, admission serum creatinine and GFR among studied patients: The mean ejection fraction (estimated by echocardiography) after intervention was 48.5 + 8.2 %. The mean baseline serum creatinine level of the studied population was 1.03 + 0.25 mg/dl, while the mean GFR was 89.9 + 32 (12 patients (20%) had GFR<60). Mean ±SD Minimum Maximum LVEF (%) 48.47 8.16 35.00 68.00 Admission serum creatinine (mg/dl) 1.03 .25 .60 1.89 GFR (mL/min/m²) 32.00 210.00 GFR<60 89.87 32.00 Yes (n %) 12 20.0% No (n %) 48 80.0% Table (1) LVEF and admission renal function of the patients. Twenty two out of 60 (36.6%) patients presented with on-admission acute hyperglycemia. 37% 63% Hyperglycemia No Yes Figure (2) Percentage of patients presenting with hyperglycemia. In-hospital complications and MACE: During hospital stay AF was recorded in 3 patients (5%), while 6 patients (10%) suffered VF. Cardiogenic shock was present in 4 patients, while 5 patients were mechanically ventilated. CIN occurred in 21 (35%) patients, of them 2 patients required hemofilteration. Overall, in-hospital mortality of the study population was 5% (n=3). In-hospital complications in relation to the presence or absence of hyperglycemia: Hyperglycemia Nº of cases No P* Sig Yes Nº % Nº % AF 3 1 2.6% 2 9.1% .548* NS VF 6 1 2.6% 5 22.7% .021* S Cardiogenic shock 4 0 .0% 4 18.2% .015* S Mechanical ventilation 5 0 .0% 5 22.7% .005* HS CIN 21 7 18.4% 14 63.6% .001** HS Dialysis 2 0 .0% 2 9.1% .131* NS Mortality 3 0 .0% 3 13.6% .045* S *Fisher exact test **Chi square test Table (2) In-hospital complications in relation to the presence or absence of hyperglycemia. CIN occurred in 14 patients (63.6%) with on-admission acute hyperglycemia, and in 7 patients (18.4%) without. All in-hospital complications (VF, mechanical ventilation, cardiogenic shock and mortality) were significantly more frequent among patients with hyperglycemia than those without. 100% 90% 80% 70% Percent 60% 50% 40% 30% 20% 10% 0% Hyperglycemic Normoglycemic CIN No CIN Figure (3) Incidence of CIN in hyperglycemic and normoglycemic patients. In-hospital complications in patients with and without CIN: Patients who suffered CIN were more prone to in-hospital complications and mortality. CIN Nº of cases No Yes P* Sig Nº % Nº % AF 3 1 2.6% 2 9.5% .278* NS VF 6 1 2.6% 5 23.8% .017* S Cardiogenic shock 4 0 0% 4 19.0% .012* S Mechanical ventilation 5 0 0% 5 23.8% .004* HS Dialysis 2 0 0% 2 9.5% .119* NS 3 0 0% 3 14.3% .039* S Mortality *Fisher exact test **Chi square test Table (3) Differences among patients with CIN regarding in-hospital MACE. 100% Percent 80% 60% 40% 20% 0% CIN No CIN Lived Died Figure (4) Relation between CIN and mortality. Multiple regression analysis to assess the association between acute hyperglycemia and CIN after adjustment of other patients’ characteristics: B P Sig. Hypertension 3.028 .130 NS .722 12.695 Dyslipidaemia 3.548 .099 NS .789 15.964 .108 NS .455 2783.262 .985 1.052 Admission serum creatinine 35.593 95.0% C.I.for EXP (B) GFR 1.018 .291 NS Hyperglycemia 10.275 .002 HS 2.340 45.109 .838 NS .264 5.164 DM 1.167 Table (4) Association between hyperglycemia and CIN after adjustment of other patients’ characteristics. After adjustment of all confounding variables, patients with admission hyperglycemia have 10 times the risk of developing CIN compared to normoglycemic patients. DISCUSSION The results of the present study showed that acute hyperglycemia in STEMI patients undergoing PPCI is a significant and independent predictor of CIN and poor in-hospital outcome. The study included 60 patients with STEMI who were treated with PPCI. Neither age nor sex differences had a significant effect on the incidence of CIN. Acute hyperglycemia is common in patients with STEMI, even in the absence of a history of type 2 DM.(17) Even mild hyperglycemia has adverse prognostic implications in patients with acute myocardial infarction. (18) Stranders et al (2004) reported that, for every 18-mg/dl (1-mmol/L) increase in glucose level, there is a 4% increase in mortality in nondiabetic patients.(19) Moreover, for the same increase in glucose level, an adjusted increase in mortality risk of 10% has been reported for STEMI patients undergoing PPCI.(20) Acute hyperglycemia is associated with several adverse effects Which include endothelial dysfunction, increased cytokine activation, increased oxidative stress, impaired microcirculatory function as manifested by postPCI "no-reflow" phenomenon, and impaired ischemic preconditioning.(21) Hyperglycemia has also several prothrombotic effects such as enhanced thrombin formation, platelet activation, and fibrin clot resistance to lysis that may contribute to an increased risk for thrombotic complications.(22) In our study population, 22 out of 60 patients presented with acute hyperglycemia. Contrast-induced nephropathy occurred in 21 (35%) patients, while 2 patients required hemofilteration. Overall, in-hospital mortality of the study population was 5% (n = 3). In the current study, all in-hospital complications occurred more frequently in the hyperglycemic group. VF occurred in 23% of hyperglycemic patient Vs. 3% in non-hyperglycemics. Mechanical ventilation was required in 23% of hyperglycemics Vs. 0% in nonhyperglycemics. Furthermore, cardiogenic shock and mortality occurred in 18% and 14% of hyperglycemic patients (respectively). Oxidant stress-mediated injury and renal medullary hypoxia and ischemia, due to vasoconstriction in response to contrast medium administration, have been implicated as causative factors for CIN.(23) Moreover, acute hyperglycemia may induce osmotic diuresis, resulting in volume depletion and dehydration and further increasing CIN risk and severity. Marenzi et al (2010) reported that, patients with acute hyperglycemia had a 2-fold higher incidence of CIN than those without. Furthermore, there was 40% in-hospital mortality in patients with acute hyperglycemia who developed CIN. Surprisingly, among patients with acute hyperglycemia, CIN rate was higher in nondiabetic than in diabetic patients (38% vs 16%, P = .003).(24) In our study, contrast-induced nephropathy occurred in 14 patients (63.6%) with acute hyperglycemia, compared with 7 patients (18.4%) in those without acute hyperglycemia. There was also positive correlation between on-admission serum glucose levels and serum Creatinine. Worth mentioning is that the contrast volume used was nearly equal in both groups. There was positive correlation between admission serum glucose level and the incidence of CIN, which is also the case with admission serum creatinine. Also, in this study group, hypertension and dyslipidemia had positive correlation with the incidence of CIN. The importance of a tight control of hyperglycemia as a strategy for improving prognosis in STEMI patients and, in general, in all critically ill patients is still under debate. Growing evidence, however, suggests that control of hyperglycemia during acute illness among diabetic and nondiabetic patients may be associated with improved outcome.(25) Van den Berghe et al (2001) showed that, in 1,548 surgical ICU patients, those rendered relatively euglycemic with insulin infusion had a 41% reduction of renal failure requiring a renal replacement therapy (4.8% vs 8.2%, P = .007) and a lower incidence of acute kidney injury (9% vs 12.3%, P = .04).(26) These findings underline the importance of control of acute hyperglycemia as a possible prophylactic strategy for prevention of CIN in STEMI patients undergoing primary PCI. After adjustment of all confounding variables in the present study, patients with on-admission hyperglycemia have 10 times the risk of developing CIN compared with normoglycemic patients. The current study had the following limitations: The sample size was rather small and the follow-up time was shortterm. The causal relationship between acute hyperglycemia and CIN remains uncertain. However, multivariate analysis showed that acute hyperglycemia was an independent predictor of CIN after adjustment for major clinical variables associated with infarct size and with development of acute kidney injury. There was no standard hydration procedure for prevention. And also we do not have enough information about the percentage of use of ACE-Is, ARBs, and diuretics. Finally, the lack of screening for patients with newly detected diabetes and with impaired glucose tolerance, and of measurement of glycated hemoglobin A1c, which would have provided some insights into the possible relationship of acute versus chronic hyperglycemia and CIN risk, represents further limitations of our study. Recommendations Based on the results of our study, future research should focus on the effect of prophylactic strategies based on tight glycemic control in prevention of CIN and improvement of the clinical outcome of patients with STEMI. Identification of high risk patients for CIN to make all attempts at the time of intervention to prevent CIN, including adequate hydration, minimization of contrast use, use of low-osmolar contrast, and possibly administration of N-acetylcysteine. Monitoring of the patients that underwent PPCI for CIN, by daily serum creatinine in the CCU, which is sometimes missed by the junior staff. Dehydration should be avoided; hydration has been proven to be safe, cheap, effective and rapid method that can be easily applied to all patients and during emergency (e.g. PPCI). Therefore prophylaxis is crucial, especially in patients considered to be at high risk for CIN. Careful use of nephrotoxic drugs that are routinely used in CCU after PPCI (e.g. ACEI, LMWHs), and modification or omission of the doses according to kidney functions. Conclusion Based on the results of the current study it can be concluded that: In STEMI patients treated with primary PCI, acute hyperglycemia is closely associated with CIN risk and in-hospital morbidity and mortality. References 1-Keeley EC, Boura JA, Grines CL, et al: Primary angioplasty versus intravenous thrombolytic therapy for acute myocardial infarction: a quantitative review of 23 randomized trials. Lancet 2003;361:13-20. 2-Rudnick M, Feldman H. Contrast-induced nephropathy: what are the true clinical consequences? Clin J Am Soc Nephrol 2008;3:263-272. 3-Wahab NN, Cowden EA, Pearce NJ, Gardner MJ, Merry H, Cox JL: Is blood glucose an independent predictor of mortality in acute myocardial infarction in the thrombolytic era? J Am Coll Cardiol 2002;40:1748–1754. 4-Norhammar A, Ryden L, Malmberg K: Admission blood glucose: independent risk factor for long-term prognosis after myocardial infarction even in non-diabetic patients. Diabetes Care 1999;22:1827–1831. 5-Capes SE, Hunt D, Malmberg K, Gerstein HC: Stress hyperglycemia and increased risk of death after myocardial infarction in patients with and without diabetes: a systematic review. Lancet 2000;355: 773–778. 6-Fava S, Aquilina O, Azzopardi J et al. The prognostic value of blood glucose in diabetic patients with acute myocardial infarction. Diabet Med 1996;13:80–83. 7-Ceriello A: Acute hyperglycemia: a “new” risk factor during myocardial infarction. Eur Heart J 2005;26:328–331. 8-Yang Z, Laubach VE, French BA, et al. Acute hyperglycemia enhances oxidative stress and exacerbates myocardial infarction by activating nicotinamide adenine dinucleotide phosphate oxidase during reperfusion. J Thorac Cardiovasc Surg 2009;137:723–9. 9-Persson PB, Tepel M. Contrast medium-induced nephropathy: the pathophysiology. Kidney Int 2006;69 (Suppl 100):S8-S10. 10-Ceriello A. Cardiovascular effects of acute hyperglycemia: pathophysiological underpinnings. Diabetes Vasc Dis Res 2008; 5: 260–8. 11-Nakamura T, Ako J, Kadowaki T, et al. Impact of acute hyperglycemia during primary stent implantation in patients with STelevation myocardial infarction. J Cardiol 2009;53:272–7. 12-Malmberg K, Ryde L, Wedel H, et al. Intense metabolic control by means of insulin in patients with diabetes mellitus and acute myocardial infarction (DIGAMI 2): effects on mortality and morbidity. Eur Heart J 2005;26:650–61. 13-Guitterez NV, Diaz A, Timmis GC et al: Determinants of serum creatinine trajectory in acute contrast nephropathy. J Interv Cardiol 2002;15: 349–354. 14-Marenzi G, Lauri G, Assanelli E, et al. Contrast-induced nephropathy in patients undergoing primary angioplasty for acute myocardial infarction. J Am Coll Cardiol 2004;44:1780–5. 15-Marenzi G, Assanelli E, Campodonico J, et al. Contrast volume during primary percutaneous coronary intervention and subsequent contrastinduced nephropathy and mortality. Ann Intern Med 2009;150:170–7. 16-Van de Werf F, Ardissino D, Betriu A, et al. Management of acute myocardial infarction in patients presenting with ST-segment elevation. Eur Heart J 2003;24:28–66. 17-Oswald GA, Yudkin JS. Hyperglycemia following acute myocardial infarction: the contribution of undiagnosed diabetes. Diabet Med 1987;4:68– 70. 18-Otten R, Kline-Rogers E, Meier DJ, et al. Impact of pre-diabetic state on clinical outcomes in patients with acute coronary syndrome. Heart J 2005;91:1466–8. 19-Stranders I, Diamant M, van Gelder RE, et al. Admission blood glucose level as risk indicator of death after myocardial infarction in patients with and without diabetes mellitus. Arch Intern Med 2004;164:982–8. 20-Ishihara M, Kojima S, Sakamoto T, et al. Acute hyperglycemia is associated with adverse outcome after acute myocardial infarction in the coronary intervention era. Am Heart J 2005;150:814–20. 21-Yang Z, Laubach VE, French BA, et al. Acute hyperglycemia enhances oxidative stress and exacerbates myocardial infarction by activating nicotinamide adenine dinucleotide phosphate oxidase during reperfusion. J Thorac Cardiovasc Surg 2009;137:723–9. 22-Undas A, Wiek I, Stepien E, et al. Hyperglycemia is associated with enhanced thrombin formation, platelet activation, and fibrin clot resistance to lysis in patients with acute coronary syndrome. Diabetes Care 2008;31:1590–5. 23-Persson PB, Tepel M. Contrast medium-induced nephropathy: the pathophysiology. Kidney Int 2006;69 (Suppl 100):S8-S10. 24-Marenzi G, MD; Monica De Metrio, MD; Mara Rubino, MD; Gianfranco Lauri, MD; Annalisa Cavallero, MD; Emilio Assanelli, MD; Marco Grazi, MD; Marco Moltrasio, MD; Ivana Marana, MD; Jeness Campodonico, MD; Andrea Discacciati, MSC; Fabrizio Veglia, PhD; Antonio L. Bartorelli, MD Posted: 01/31/2011; American Heart Journal 2010;160(6):1170-1177. 25-Marfella R, Di Filippo C, Portoghese M, et al. Tight glycemic control reduces heart inflammation and remodeling during acute myocardial infarction in hyperglycemic patients. J Am Coll Cardiol 2009; 53:1425–36. 26-Van den Berghe G, Wouters P, Weekers F, et al. Intensive insulin therapy in critically ill patients. N Engl J Med 2001;345:1359–67.