Intellectual Property Law

1 Intellectual Property Law Chloe Bunn
Intellectual Property Law
(LW556)
The Patenting system deprives developing countries of the South from valuable life-saving drugs: A focus on Generic drugs and the
HIV/AIDS crisis in sub-Saharan
Africa.
Chloe Bunn
2004/2005
Word Count (excluding titles subheadings and tables): 5,437
Chloe Bunn 2 Intellectual Property Law
Contents
Contents
…………………………………………………………………………… ...
2
Abstract ……………………………………………………………………………. ...
3
Part 1 – Introduction, a look at what defines a generic drug, and the motivation for this article …………………..…………….... ….……………………………… 4-5
Part 2 – The reasons why this article favours generic drugs over patented pharmaceuticals ……………………………………………………………………...
6
2.1 The problem with patents…………………………………………………….……6
2.2 The benefits of generic drugs…………………………………………………....6-8
2.3 A small note: The generic drug Nevirapine...…………………………………...8-9
2.4 Why have the MNCs lobbied against Generic drugs? Are there any drawbacks to generic drugs?...........................................................................................................9-10
Part 3 – Barriers to generic drugs ...……………………………………………….
11
3.1 In order to understand how generic drugs are affected by the current intellectual property regime, the different ways in which generic drugs can be legitimately manufactured or accessed must first be established…………………………..…..11-12
3.2 The legislative barriers: The potentially disastrous effects of the provisions that hinder access to affordable generic drugs ………………………………………..12-13
3.3 Compulsory Licensing as an
‘escape hatch’
for countries to manufacture or import generic drugs: Article 31 TRIPS – ‘Other Use without authorisation of the right holder’ ……………………………….……………………………...………14-15
3.4 Multinational Corporations as a barrier to generic drugs………………..…...15-16
Part 4 – Studies from India and Brazil ...………………..…………………..…….17
4.1 Study 1 - India: A real time illustration of how the Generic industry is affected by the current intellectual property regime…………………………………………..17-19
4.2 Study 2 – Brazil’s ‘radical move’: An example of how a country can put patients over patents and reap vital rewards from the use of generic drugs….……………20-21
Part 5 – Possible solutions/reform to assist generic production and therefore access to essential medicines for the future and conclusion
…………………...…
22
Part 6 – Bibliography ……………………………………………………………….25
6.1 Cited Articles/Papers ……………………………………………………….........25
6.2 Cited Articles from Websites/Electronic
Sources……………………………………..……………………………………..25-27
6.3 Other cited websites……………………………………………………………...27
6.4 Background Reading……………………………………………………………..28
Chloe Bunn 3 Intellectual Property Law
ABSTRACT
‘There is nothing more valuable than life’
- The UNAIDS country coordinator, Dr.
Ruben Prado.
Generic drugs could be the difference between life and death for millions of people in developing countries, such as South Africa, Malawi and Zimbabwe to name a few, who are suffering from HIV/AIDS. This article argues that the current patent regime acts as a barrier to these cheaper generic drugs resulting in a devastating impact on the poorer people of the world. It will be illustrated that really, we are living in a world where priority is afforded to Patents over people,
“put baldly patents are killing people” 1
.
In support of this argument, the generic industry, and the benefits of these drugs such as cost and generic competition will be explored. It will be submitted that the WTO
TRIPS agreement 1994 since January 2005 increases monopoly over life-saving drugs by requiring countries to institute patents on the products ; this has a potentially disturbing affect on the generic industry particularly in India, and therefore on the developing countries, such as sub-Saharan Africa, who greatly rely on these generic drugs. Proposals for solutions to the problems these countries face will be addressed and Brazil’s ‘radical’ move to defy the pharmaceutical companies and manufacture their own generic drugs will be considered. In conclusion if these life-saving drugs were taken out of the patenting process, or the safeguards in the TRIPS agreement were strengthened and cheap generic versions of these drugs were made readily available to these countries, the crisis in countries like Africa would be eased.
1 Tina Rosenberg - The New York Times Magazine 28 th January 2001 www.nytimes.com/library/magazine/home/20010128mag-aids.html
Chloe Bunn 4 Intellectual Property Law
PART 1
Introduction, a look at what defines a generic drug, and the motivation for this article.
1.1 Why is it that in western countries AIDS is not the ‘unstoppable killer’ that it is in the Sub-Saharan Africa? The answer lies in the availability of anti-retroviral medications
2
(ARVs) which although have curtailed the deaths of the majority of suffering patients in western countries, they have been largely unavailable to the poorer countries of the world due to their high cost. Cheaper generic drugs therefore have been of extreme importance to these countries in providing a means of accessing essential medicines.
1.2 A generic drug has been defined as being ‘identical, or bioequivalent to a brand name drug in dosage form, safety, strength, route of administration, quality, performance characteristics and intended use’ 3 .
Basically, generic drugs are a chemically identical ‘copy’ of a brand named product 4 , and sold after the patent on the originator drug has expired, at a cheaper price. According to William Haddad
5
, it is estimated that when a generic drug first comes to the market the prices average at
66.6% of those of the brand name originator drug; and in the poorer nations of the world, a drug in generic form can average 1-5% of the patented price 6 .
1.3 Although this article acknowledges the fact that many issues influence the availability of essential medicines
7
, it will be illustrated as the main focus of the dissertation, that the decisions made in the developed countries i.e. the current intellectual property regime, greatly impact and restrict the access to affordable generic medicines in the poor and developing nations. The disturbing rate at which the
2 These are recommended as first line treatment for patients with AIDS by the World Health
Organisation.
3 The US Food and Drug Administration Centre for drug evaluation and research – Office of generic drugs - http://www.fda.gov/cder/ogd/#Introduction
4 For example Paracetamol is the generic form of Panadol® or Tylenol® - http://www.avert.org/generic.htm
5 William Haddad has had much experience in the manufacturing and political side of the generic industry, for example, among his other ventures he has been chairman of the CEO of the US Generic
Pharmaceutical Industry Association for 10 years.
6 ‘Generic Drugs: The Solution or the Problem?’ William Haddad
7 For example poverty, financing and lack of resources etc.
Chloe Bunn 5 Intellectual Property Law
HIV/AIDS epidemic is affecting the poorer countries of the world provides a real time example of this and is the motivation for this article.
1.4 To illustrate the scale of the problem of HIV/AIDS, UNAIDS figures reveal that although Sub-Saharan Africa has just over 10% of the world’s population, ‘ it is home to more than 60% of all people living with HIV/AIDS
8 ’ and it has been estimated that a mere 8% of people receive treatment in the form of ARVs 9 due to the high costs of patented pharmaceuticals. It is not hard to believe therefore that the disease is the leading cause of death in these parts of the world; it has been estimated that in 2003 the total number of deaths caused by the disease was 2.2 million
10
, with the numbers rising to 2.3 million in 2004
11
. The number of people now living with HIV/AIDS in sub-Saharan Africa is worryingly 25.4 million, and as a result of the pandemic the average life expectancy which should be 62 years, has been alarmingly reduced to 47 years
12
. Based on these shocking figures it is predicted that by 2010 the populations of many countries
13
will greatly decrease because of the number of people dying of
AIDS – and frighteningly, the population growth rate in Zimbabwe and Namibia will have slowed to almost zero
14
. Even where there is evidence of decline in the disease levels in countries such as Ethiopia, Kenya and Uganda, the future is still uncertain.
1.5 This future uncertainty is no doubt partially a result of the World Trade
Organisation’s Trade-related Aspects of Intellectual Property Rights (TRIPS
Agreement) 1994
15
which is currently a cause for grave concern amongst the poorer countries of the world, and it will be illustrated why this is so in the main thrust of the argument.
8 UNAIDS Factsheet - http://www.unaids.org/bangkok2004/factsheets.html - Based on the 2004
‘Global report on the HIV/AIDS epidemic’.
9 Article: ‘Providing drug treatment for millions’ - http://www.avert.org/drugtreatment.htm
10 http:/www.avert.org/subaadults.htm
11 UNAIDS (2004) ‘Report on the Global HIV/AIDS epidemic’ , - http://www.unaids.org/html/pub/publications/fact-sheets04/FS_SSAfrica_en_pdf/FS
12 At one end of the scale, the life expectancy at birth in Zimbabwe has greatly decreased from 52 years in 1990 to 34 years in 2003 see http://www.avert.org/aidsimpact.htm - Stanecki K. A. (2002)
‘The
AIDS pandemic in the 21 st Century ’, Draft Report, July 2002, XIV International Conference on AIDS,
Barcelona, US Census Bureau.
13 Including Botswana, Central African Republic, Lesotho, Malawi, Mozambique, Rwanda, Swaziland,
Zambia, and Zimbabwe.
14 ‘The impact on life expectancy’ - http://www.avert.org/aidsimpact.htm
15 TRIPS = Agreement on Trade Related Aspects of Intellectual Property rights 1994
Chloe Bunn 6 Intellectual Property Law
PART 2
The reason why this article favours generic drugs over patented pharmaceuticals.
2.1 The problem with patents
The currently over-protective patent laws allow large Multinational Corporations
(MNCs) such as Glaxo-Smith Kline, Merck & Co, and Bristol-Myers Squibb, which are some of the leading producers of US pharmaceuticals, to place
‘profits over people’ 16
. The system permits a select few pharmaceutical companies to have the advantage of a twenty year monopoly over life-saving anti-HIV/AIDS drugs; this power then enables the MNCs to gain high profit margins because they are able to control the price of their drug, for example, it is estimated that Glaxo-Smith Kline makes a profit of £6 billion per annum 17 . This has been made equally possible to achieve by western governments who are able to meet the high price demands from these corporations. Unfortunately while this profit is enjoyed by the few granted patent protection, this market exclusivity makes these drugs unaffordable to developing countries resulting in a devastating effect on the poorer people of the world.
2.2 The benefits of generic drugs
An obvious advantage to generic drugs therefore, is that because they can make use of expired patent products, the generic manufacturers do not have to spend large amounts of their budget on research and development costs that the MNCs do. For example, although the approximate expenditure of R & D greatly varies, in a recent report it was estimated that Glaxo-Smith Kline spends $500 million, over a period of about thirteen years, to develop a major drug 18 . This also means that there is not the pressure on generic manufacturers that MNCs have in recouping the initial expenditure. Therefore the generic industry can afford to lower the price barrier that restricts developing countries from accessing essential anti-HIV/AIDS treatment.
16 Article – ‘Profits over People’ AIDS India’s National Magazine - http://www.frontlineonnet.com/fl2116/stories/20040813003210400.htm
17 The Guardian Friday February 4
18 The Guardian Friday February 4 th 2005 – ‘Raking it in – How much is too much?’ th 2005 – ‘Raking it in – How much is too much?’
Chloe Bunn
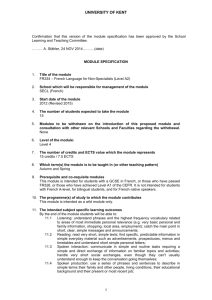
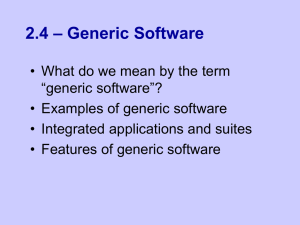
Table 1
ARV Combinations
1.
Combivir (brand)
(AZT 300mg + 3TC 150mg)
Duovir (generic)
(AZT 300mg + 3TC 150mg)
2.
D4T 40mg + 3TC 150mg (brand)
D4T 40mg + 3TC 150mg
(generic)
3.
D4T 40mg + ddI 100mg
(brand)
D47 40mg (generic) + ddI 100mg (brand)
4.
Triomune (generic) (D4T 40mg
+ 3TC 150mg
+ Nevirapine 200mg
7 Intellectual Property Law
$80
+ Nevirapine (200mg)
Brand Drug
$116
Generic Drug
$96
$60
$72
$52
$65
$64
$52
$47
$45
$44
40
*Lowest price in Uganda*
The table above indicates the difference in price between brand named and generic
ARV combinations (at lowest retail price) in Uganda for one month’s treatment supply 19 .
There is no clearer example of current price barriers when it is considered that the average monthly salary for a Ugandan Farmer is between $55 and $138, yet to receive one month’s supply of the brand-named ARV combination ‘Combivir + Nevirapine’ it would cost $116 20 . This can be compared to the most common, least expensive generic ARV drug on the market ‘Triomune’, which is produced by the Indian generic manufacturers Cipla and costs just $40 a month. It is therefore plain that generic medicines offer an
‘affordable difference between life and death’ 21
.
Because generic drugs cost less than brand name or innovator counterparts another benefit is that they play an important role in drug ‘competition’. This competition can drive down the prices of patented pharmaceuticals; for example, in 2001 following the significant price reductions from two Indian generic drug makers, Bristol-Myers
Squibb agreed not to use its patent in South Africa on the AIDS drug Zerit to block the country from legally buying generic copies of Zerit, but in doing so they offered to
19 Access to Antiretroviral therapy in Uganda – Kampala June 2002 http://www.oxfam.org.uk/what_we_do/issues/hivaids/downloads/arvaccessuganda.pdf
20 See ‘Access to Antiretroviral Therapy in Uganda’ page 15 www.oxfam.org.uk/what_we_do/ issues/hivaids/downloads/arvaccessuganda.pdf
21 Generic Medicines – The Solution or the problem by William (Bill) Haddad page 5
Chloe Bunn 8 Intellectual Property Law sell Zerit for $54 a year to Africa as opposed to $270 from the previous year
22
. This is an obvious advantage because it encourages the MNCs to become more willing to supply their drugs at a cheaper rate to poorer countries which results in an increase in the availability of the ARV drugs. Many argue that the benefit of generic competition is conditional upon whether the brand name companies respond to this competition or not, and claim that often they do not. However even if this were the case, generic competition is still advantageous as there may be competition between generic drugs themselves; i.e. the increasing number of manufacturers producing the same generic drug means that the average price of a generic drug will inevitably decrease. It was found that when 1-10 generic corporations manufacture and distribute generic forms of a particular drug, the price of that drug averages about 60% of the brand named price; when more than 10 generic manufactures enter the market, the average price declines to less than half of the brand name price.
23
2.3 As a small note to illustrate the real time effects of generic drug availability, looking at things on a larger scale, because the patenting system facilitates market monopoly, pregnant women in sub-Saharan Africa cannot afford the necessary drugs which prevent mother to child transmission of the HIV/AIDS disease and it is estimated that approximately 200 babies are born HIV positive each day in South
Africa. The availability of the cheap generic drug Nevirapine can greatly ease the crisis in developing countries in the future as the use of Nevirapine can reduce Mother to child transmissions by half
24
.
To summarise, generic drugs are obviously favoured above patented pharmaceuticals because a) the price of patented pharmaceuticals is too high to be accessible to places like sub-Saharan Africa b) patenting pharmaceuticals means that monopolies are created in favour of MNCs c) generic drugs benefit the economy by ‘holding down’ national spending on prescription drugs d) generic drugs provide a ‘benchmark’ for
22 The Wall Street Journal March 15 th 2001 ‘Bristol Myers Squibb offers to sell AIDS drugs in Africa at below cost’ -http://www.aegis.com/news/wsj/2001/WJ010312.html
23 See article ‘How increased competition from generic drugs has affected prices and returns in the pharmaceutical industry’ http://www.cbo.gov/showdoc.cfm?index=655&sequence=0&from=1
24 See ‘Effort to make the Government Provide Nevirapine to pregnant HIV+ women to prevent mother to child transmission of HIV’.
http://www.cptech.org/ip/health/sa/mtct.html
Chloe Bunn 9 Intellectual Property Law low prices through competition
25
and e) most importantly
‘using generic antiretrovirals offers the possibility of treating twice the number of people with the same amount of money.
26 ’
2.4 Why have the MNCs lobbied against Generic drugs? Are there any drawbacks to generic drugs?
The most obvious concern is that generic drugs are not the same standard of quality as the patented pharmaceuticals and this is what used to be predominantly argued by the large pharmaceutical companies
27
, often in an attempt to continue to hold market share and protect their profits. Despite the stigma which may have been attached to generic drugs in the past i.e.
that they are a
‘second class’
medicines
28
, their quality has been defended by the US FDA which regulates both generic and brand named pharmaceuticals 29 . Another argument which the MNCs have used to discourage the use of generic drugs is that generic drugs look different to patented pharmaceticals and the incorrect useage of the drugs could lead to a more resistant strain of the disease causing more harm than good; a common argument was that
‘uneducated people cannot stick to their medicine on time as patients in the United States can’.
This is based on fallacious grounds; however if this were true it would surely mean that people in the poorer countries would not be able to use patented pharmaceuticals either.
It can be said quite confidently that generic drug manufacturers are generally seen as a threat to the MNCs profits; this belief is not unfounded as the CBO
30
examined 21 brand name prescription drugs in its’ retail pharmacy data set and noted that at the end of the year in which the patent on the originator drugs had expired those drugs lost an average of 44% of their market to generic drugs.
31 While this article acknowledges the
25 For example, according to an Oxfam briefing paper ‘Generic competition, price and access to medicines’ it was found that due to the importation of generic drugs and price cuts induced by generic firms, the number of patients that were able to be treated in Uganda was increased from 962 – 3000
(2002 report), see http://www.oxfam.org.uk/what_we_do/issues/health/bp26_generic.htm
26 See article ‘Importation of generics cuts price in half’ www.oxfam.org.uk/press/releases/tac.htm
27 Such as Warner-Lambert and its subsidiary, Parke-Davis.
28 ‘Generic Medicines: The Solution or the Problem?’
By William Haddad page 9
29 It was a common belief in developing countries that generic drugs were ‘sub-standard’, see quote:
‘just because we are poor does not mean we should be treated with second class medicines.’ Article:
‘ Generic Medicines: The Solution or the Problem?’ – William Haddad page 9
30 CBO = Congressional Budget Office USA
31 See article ‘How increased competition from generic drugs has affected prices and returns in the pharmaceutical industry’ at http://www.cbo.gov/showdoc.cfm?index=655&sequence=0&from=1
Chloe Bunn 10 Intellectual Property Law fact that the MNCs should be able to reap the rewards for their innovative drugs, Bill
Haddad’s argument that ‘if the same drugs are life saving and the public is dying on account of non-affordability of the drug, then the MNCs should be ready for the option of bringing the price to the level of the dying person’s affordability, 32 ’ is heavily supported.
32 Interview William (Bill) Haddad a strong advocate of generics across the globe - ‘India should strive for postponement of WTO deadline to 2016’. Interview with William Haddad Thursday 25 th December
2003 by Prabodh Chandrasekhar
Chloe Bunn 11 Intellectual Property Law
PART 3
Barriers to Generic Drugs
3.1 In order to understand how generic drugs are affected by the current intellectual property regime, some of the different ways in which generic drugs can be legitimately manufactured or accessed must first be established.
A. ‘Voluntary licenses’
Voluntary licenses can be granted by the Multinational Corporations (MNC) to governments or generic companies which means that they would then be able to legally produce generic versions of certain patented drugs. For example, recently
33
the world’s largest pharmaceutical manufacturer of AIDS drugs, GlaxoSmithKline, granted a voluntary licence to Cipla-Medpro
34
a generic company in South Africa, for the importation and sale of generic versions of antiretroviral medicines including its patented drugs lamivudine, zidovudine and a combination of the two
35
. This would appear to be a model solution to the developing countries’ needs in accessing affordable medicines; however it is unsurprising to discover that generally the MNCs refuse to grant voluntary licenses. The reason for this is that as well as seeing generic drugs as a threat to their profits when they are sold in the poorer countries, the pharmaceutical industry fears also that the drugs will
‘find their way back into the richer markets.
36 ’
B. Donations
For some products the MNCs generously donate their medicines to developing countries
37
especially in times of crisis; however although this no doubt makes access to drugs easier, the donations are too infrequent and the drugs to be donated are often selectively chosen enabling countries to treat a small number of ‘opportunistic fungal infections in HIV/AIDS patients 38 ’ ; this alone cannot curtail the majority of deaths in
33 14 th December 2004
34 Cipla-Medpro is a subsidiary of the major Indian manufacturing company Cipla which will be mentioned later on this dissertation.
35 See
‘Glaxo grants Cipla AIDS-Drug Licence’
http://allafrica.com/stories/200412150122.html
36 ‘Brazil to break AIDS drug patents’ 1 st December 2004 – http://news.bbc.co.uk/2/hi/health/4059147
37 For example Pfizer and the South African Government initiated a program in 2000 ‘ The Diflucan
Partnership Program’ which made their patented AIDS drug ‘Diflucan’ available for free in South
Africa with no time or dollar limit. This program has extended to other countries since then.
38 See Pfizer ‘Seeds of hope’ http://www.pfizer.com/are/investors_reports/annual_2002/p2002ar18_19_20_21.htm
Chloe Bunn 12 Intellectual Property Law these countries and the patent regime still allows for control over the many other life saving drugs unavailable to the poorer nations.
C. Process patents rather than product patents: before 2005
As noted above, anti-HIV/AIDS drugs cannot be afforded in poorer parts of the world such as sub-Saharan Africa, unless they can be cloned in the form of a generic drug.
The generic drug industries have been able to legally copy the originator drugs because it was the process of making the drug that was protected by patent laws and not the product itself; this means that 3 rd
parties, i.e.
generic drug industries, could produce the same drug by manufacturing the product through another process than that already protected under patent law. This method is of extreme importance and countries such as India which have the means to manufacture these drugs have been permitted to export them to countries which do not have a thriving generic pharmaceutical industry. Sub-Saharan Africa is a prime example; the people are therefore dependant on these generic imports. The problems that the generic industry and this method face in relation to the TRIPS agreement will now be illustrated below.
3.2
The legislative barriers: The potentially disastrous effects of the provisions that hinder access to affordable generic drugs.
The WTO TRIPS Agreement
When the member countries joined the WTO they signed several agreements and agreed to amend their domestic laws in order to conform with the international trade rules. The implementation of one of these agreements, the TRIPS agreement, poses a huge threat to accessing essential generic medicines in poorer countries. One reason for this can be found under article 27 which states:
27 (1) ‘Subject to the provisions of paragraphs 2 and 3, patents shall be available for any inventions, whether products or processes, in all fields of technology, provided that they are new, involve an inventive step and are capable of industrial application....’
Following this article, article 28 (1) (a) states that a product patent confers on its owner the exclusive right to prevent third parties from making, using, offering for sale, selling or importing for these purposes the product. This means that as well as imposing twenty year patents on all new products, TRIPS effectively abolishes the
Chloe Bunn 13 Intellectual Property Law right to manufacture generic medicines using the non-infringing patent process method.
2005 marks the year of arguably the greatest impact of these provisions in the TRIPS agreement as middle-income countries were granted until the 1 st January this year to start granting patents for processes and products. This is therefore an area of current concern as countries such as India, have had to adjust their patent law to comply with
TRIPS. The negative consequences that flow from this change are obvious, ‘Basically the TRIPS agreement that becomes virtual world law in 2005…will terminate the lifeline of essential medicines traditionally exported to poor nations by India
39 ’ this will mean that there will also be a reduction of the important generic competition which drives down the prices of brand name drugs, and the provisions pose a huge threat to the future of the generic industry
40
.
It has been remarked that the rules in TRIPS ‘have little to do with free trade and more to do with the lobbying power of the American and European pharmaceutical industries
41 ’.
It would appear to be true that because MNCs see generic drugs as a threat they use their patents as a weapon, along with their money and powerful western governments, to lobby against greater access to them in an attempt to protect their profits; as a point to note, this would appear to contradict the fundamental element of what TRIPS aims to achieve i.e.
‘that the measures and procedures to enforce intellectual property rights do not themselves become barriers to legitimate trade’.
The implementation of the TRIPS agreement has also opened the doors for ‘TRIPS-
Plus’ agreements which contain unnecessarily rigid provisions which further hinder generic production 42 ; ‘ the name of the game is to extend patents and block
39 ‘ Generic Medicines – The Solution or the problem’ by William (Bill) Haddad page 1
40 India will be focused on later as an illustration of how the Generic industry is affected by the current intellectual property regime and how this in turn affects the regions of sub-Saharan Africa.
41 ‘India’s Choice’ The New York Times Editorial January 18 th 2005
42 An illustration and the effects of a TRIPS-Plus agreement will be given in Part 4 Study 1: India.
Chloe Bunn 14 Intellectual Property Law competition
43 ’
. Therefore any safeguards within TRIPS which might assist generic production must now be explored.
3.3 Compulsory Licensing as an
‘escape hatch’
for countries to manufacture or import generic drugs: Article 31 TRIPS –
‘Other Use without authorisation of the right holder’
It would appear that the ‘safeguard’ of compulsory licensing serves to restrict the monopoly rights given to patent holders and therefore would assist in the availability of generic drugs. In basic terms a compulsory licence means that the government of a
WTO Member country can grant licences to a government agency or company for the production or importation of a patented drug without the permission of the patent holder in situations of national emergency, or for exporting medicine to countries facing public health emergencies. The legal basis for compulsory licensing is found under Article 31 TRIPS which allows for WTO member states to:
‘use the subject matter of a patent without the authorisation of the right holder, including use by the government or third parties authorised by the government’
In effect, by allowing production of the drug without the patent holder’s consent,
Article 31 of the TRIPS agreement would appear to overcome the problem of TRIPS as a legislative barrier to generic drugs as it acts as an
‘escape hatch 44 ’ to the product patent regime under article 27. However this provision is not without many artificial barriers also which block its use, including apparent contradictions and confusion over the terms, resulting in most governments not making use of the provision which in turn results in an adverse affect on the availability of generic drugs. One of the most prominent reasons for its lack of implementation has been due to the fact that the majority of developing countries do not have the sufficient means both in terms of economic efficiency and manufacturing capability etc, to produce ARVs. For example in places like India it would be relatively simple to grant a compulsory licence for the production of patented drugs as the pharmaceutical market is very large; however in
43 Testimony of William Haddad before the Committee on International Trade, European Parliament on
TRIPS and Access to medicines – see http://lists.essential.org/pipermail/ip-health/2005-January
/007394.html
44 ‘ Generic Medicines the Solution or the Problem?’ - William (Bill) Haddad page 1
Chloe Bunn 15 Intellectual Property Law sub-Saharan Africa where unfortunately the AIDS disease is most severe, the smaller market means that it might be difficult to establish economically viable production
45
.
The next question that arises is whether the member states can issue compulsory licensing for importation, as this would greatly assist developing countries in accessing cheap generic drugs from other countries with adequate pharmaceutical sectors. The restrictions under article 31 (f) which states that “…any such use shall be authorised predominantly for the supply of the domestic market of the market of the
Member authorising such use;” meant that this too presented a problem in that it limited the amount of generic drugs which a country could export to poorer countries unable to manufacture their own drugs; developing countries would only be able to import generic drugs from countries where the patents have expired or the pharmaceuticals are just not patented. Paragraph 6 of the DOHA declaration addressed the problem
46
and on the 30 th
August 2003 there was decision to lift the
TRIPS restrictions on compulsory licensing for export of generic medicines to countries that
‘lack the capacity to manufacture the drugs themselves’ 47
. The generic
ARVs currently imported by the developing countries are not the major concern here as they make use of expired patents; therefore the concern is focused on that of future developments in AIDS treatments. The newer life saving drugs on the market are bound to become more advanced in future years due to the ever increasing innovation within the pharmaceutical industry, however these will inevitably not be easily accessible to countries such as sub-Saharan Africa. The patent restrictions are not the only problems that developing countries face in their struggle for generic medicines; in practice compulsory licensing is often ‘controlled by a political process where the vote of one WTO member can prevent implementation
48 ’ and also by using the threat of trade sanctions, the richer countries tend to bully poorer countries into disregarding their rights 49 . For example, the US often uses bilateral pressure to stop poorer
45 See
‘Implications of the DOHA Declaration on the TRIPS agreement and Public Health’
Page 19 - www.who.int/medicines/library/ par/who-edm-par-2002-3/doha-implications.doc
46 The DOHA Declaration aimed to ‘promote access to medicines for all’ and under paragraph 6 recognised that “WTO members with insufficient or no manufacturing capacities in the pharmaceutical sector could face difficulties in making effective use of compulsory licensing under the TRIPS
Agreement.”
47 ‘Undermining Access to medicines’ Oxfam Briefing note June 2004 http://www.oxfam.org.uk/what_we_do/issues/health/undermining_access_ftas.htm
48 ‘Generic Medicines: The Solution or the Problem?’ William Haddad page 1
49 See ‘ US bullying On Drug Patents: One Year After DOHA, Oxfam Briefing Paper no. 33’ www.oxfam.org.uk/policy/papers/24global fund.html
Chloe Bunn 16 Intellectual Property Law countries from using compulsory licensing for pharmaceuticals
50
. The results of this dilemma would appear ultimately to mean that developing countries have no choice but to eventually become completely reliant upon the expensive patented pharmaceuticals, a fate which the generic drug industry has for years desperately tried to avoid.
3.4
Multinational Corporations
It has already been mentioned why MNCs see generic drugs as a threat and that often they will spend a great deal of time and money lobbying to block other means to accessing essential medicines. The following case study provides an example of an aggressive attempt by the MNCs to protect their patent rights above public health in
South Africa.
Case study
The 'Medicines Act' 1997, was introduced by the South African government with its intended purpose being to bring down the price of essential medicines and promote national health above patent rights. The backlash was that the Pharmaceutical
Manufacturers' Association and forty brand name companies then took the South
African government to court to block the Act, naming Nelson Mandela as the main defendant and relying on the argument that the Act
‘broke their patent rights and would harm their profits
51 ’
. They withdrew the case in 2001 after a huge public outcry, but
‘this aggressive action revealed to the world the strength of the pharmaceuticals' grip on the availability of essential medicines, and their desire to protect their patents at all costs’
52
.
50 For example , ‘the US is actively pressuring South Africa and Thailand against the use of compulsory licenses of pharmaceuticals to treat AIDS’ See http://www.cptech.org/ip/health/cl/faq.html
51 http://www.peopleandplanet.org/stopaids/briefing.access.php - ‘Treat AIDS now – Blocking Access’.
52 See Treat AIDS now – Blocking Access’. http://www.peopleandplanet.org/stopaids/briefing.access.php - ‘Treat AIDS now – Blocking Access’.
Chloe Bunn 17 Intellectual Property Law
PART 4
4.1 Study 1 - India: A real time illustration of how the Generic industry is affected by the current intellectual property regime and how this in turn affects the regions of sub-
Saharan Africa.
India has been named the ‘world’s supplier of cheap generic AIDS drugs 53 ’ as it treats patients in over 200 countries
54
. The Indian Firm Cipla has notably done
‘groundbreaking work in developing an affordable AIDS treatment mode ’ 55 by reducing the cost of AIDS medications from $12,000-$ 15,000 to $140. India has been able to allow their generic industry to flourish by using ‘reverse engineering 56 ’ and the legitimate method of manufacturing generic drugs through a process different to that of its originator drug
57
. Since Indian law had no product patent constraints before 2005, generic companies have used drugs patented by different companies to develop combination pills which are extremely popular in treating HIV/AIDS. In developing countries; in sub-Saharan Africa particularly, there is a huge reliance on having these generic drugs imported.
However India is one of the many countries who are a member of the World Trade
Organisation and signed up to the TRIPS agreement. This meant that by the 1 st
January of this year, the Indian Government had to comply with the protection of
‘product patents’ regime under article 27(1) TRIPS. On the 26 th
December 2004, the
Indian government issued a Patent Ordinance which made several amendments to
India’s current patent regime (Patent Act 1970) in order to fulfil their obligation to the
WTO. Many of the provisions contained in the Ordinance are unnecessarily constraining and critics have described these as ‘TRIPS-Plus’ as they go beyond what is required to be in line with the TRIPS agreement, and it does not take full advantage of the WTO safeguards for the protection of public health 58 . The ordinance includes affording full TRIPS coverage to pharmaceuticals; among many other amendments 59 , it requires patents to be granted on products, it limits the grounds on which objections
53 The New York Times, January 18 2005
54 Medicins Sans Frontieres claims that about half of the 700,000 people receiving antiretroviral treatment for HIV/AIDS in developing countries relied on drugs from Indian generic drug makers.
55 http://yaleglobal.yale.edu/display.article?id=4808
56 This involves chemists ‘dissecting’ a patented molecule.
57 Refer to paragraph 3.1 C above for more information.
58 See ‘Global Day of Action against Indian Patent Ordinance’ 26 th February 2005 http://lists.essential.org/pipermail/ip-health/2005-February/007465.html
59 Over 70 amendments in total.
Chloe Bunn 18 Intellectual Property Law to patent applications may be made, and restricts the scope of compulsory licensing.
Y K Hamied, chairman of Cipla Ltd, argued that the compulsory licensing provision in particular should be amended;
60
as it was illustrated earlier that restraining compulsory licensing leads to a greater restriction in the availability of generic drug production and it also gives MNCs a greater chance to abuse the patent system by creating unfair monopolies
61
.
Update
Indian law states that the Ordinance will lapse if it not ratified by lawmakers within six months of the issue date; since initially researching this area, the Indian Parliament went into session on the 25 th
of February
62
and on the Friday 18 th
March, despite objections from the opposing political parties
63
, the government introduced the
‘Patent Bill 2005’ which replicates that of the controversial ordinance promulgated in
December.
The negative effects of the new regime on the accessibility of generic drugs
The effects of this more ‘stringent’ intellectual property regime are predicted to increase prices for essential drugs as it will reduce the advantage of competition that the generic drugs provide; the balance of interests will therefore become more heavily in the favour of the MNCs resulting in a greater control over prices. In response to this criticism, Ajit Danji (Director General Organisation of Pharmaceutical Producers of India) argues that because over 95% of the drugs in the World Health Organisation list of essential drugs are already out of patent they will continue to be available at low prices; plus the National Pharmaceutical Pricing Authority (NPPA) will keep on monitoring medicine prices. This is indeed a valid point as the rules do not apply to drugs which were patented before 1995 which inevitably means that Cipla can continue to sell its widely distributed generic version of the HIV treatment AZT
64
; however the changes appear not to take into account the needs of poorer developing
60 This was published in a report recently by the Indian Drug Manufacturers Association.
61 The changes were also heavily opposed by many groups including the Affordable Medicines
Treatment Campaign (AMTC); of course the MNCs have backed these changes to the law as it is very much tilted in their favour.
62 Once Parliament goes into session, an Ordinance lapses within six weeks if a consensus is not reached between the government and the parties who oppose it.
63 Namely the Left parties in particular Bhartiya Janeta Party (BJP)
64 See ‘New patent law to shake up drug industry’ - http://lists.essential.org/pipermail/ip-health/2004
Chloe Bunn 19 Intellectual Property Law countries.
As noted above because the twenty year patent protection is afforded to products , a new or enhanced ARV or even a cure one day may be available to India through compulsory licensing, but will be out of reach for regions such as sub-
Saharan Africa because a) It is unlikely that many regions of Africa have the capabilities to manufacture drugs through compulsory licensing, b) the amendments
‘ prevent least developed countries from requesting the export from India of generic versions of a medicine that is not under patent in the least developed country in question.
65 ’ and c) MNCs will have complete monopoly over prices 66 . Also it does not seem to be considered that AIDS can only be treated in ‘half measures 67 ’ and ‘for
HIV patients unresponsive to the currently available formulations, access to the more expensive second-stage AIDS drugs is critical
68 ’
; the new anti-AIDS drugs that will cost more than basic ‘initial combinations’ will be out of reach to these sufferers.
In summary the Indian government in complying with TRIPS has gone too far and the provisions in the Bill are set to adversely affect the Indian generic drug industry which is relied upon by millions as a means of accessing affordable HIV/AIDS drugs.
Although the government has plans to negotiate with political parties to obtain changes to the bill, these have been viewed as
‘far from satisfactory in terms of protecting and ensuring the public’s future ability to access affordable medicines and healthcare
69 ’ and it remains to be seen how steady the grounds on which the future of the generic industry in India stands.
65 Criticism put forward by the ‘Affordable Medicines and Treatment Campaign ’ (AMTC) - http://lists.essential.org/pipeline/ip-health/2005-January/007368.html - ‘Indian Trips Legislation under fire’.
66 There was also the fear by many local industries that ‘evergreening’ would be permitted; this would further hinder generic drug production as it would mean that multinationals would be granted patents even when they make minor changes to drugs so that their patent lives get extended, thereby delaying the introduction of generic medicines. However it has been proposed that this will not be permitted under the Bill.
67 I.e.
Many patients do not respond positively to some of the ARV medicines available.
68 See ‘New Indian Patent Law pushes up prices of anti-AIDS drugs’ http://lists.essential.org/pipermail/ip-health/2005-February/007464.html
69 See http://lists.essential.org/pipermail/ip-health/2005-March/007625.html
Chloe Bunn 20 Intellectual Property Law
4.2 Study 2 – Brazil’s ‘radical move’: An example of how a country can put patients over patents and reap vital rewards from the use of generic drugs.
Brazil has been considered to provide an excellent example of a model solution to the
AIDS epidemic in poorer countries. The Brazilian government in 1996 felt that the prices of anti-retroviral treatments were ‘needlessly out of reach to the vast majority of the world’s population 70 ’ and was willing to ‘do anything necessary to source the lowest cost quality ARVs 71 ’ . The governement therefore implemented a national treatment programme: ‘Programme on Universal Access to Treatment of HIV/AIDS’.
Through this programme Brazil has made cheap generic versions of the unaffordable drugs themselves by setting up their own non-profit generics manufacturing company to provide free ARVs for all those who need them. Since 1996 Brazil has cut the number of people dying in half
72
and the hospitalisation rate has declined by 80%; because of this decline in hospitalisations and a decreased need to treat opportunistic infections, the government saved a total of $472 million (US Dollars) between 1997 and 1999 making the programme almost fund itself
73
! Another strategy that Brazil has adopted in relation to accesing these essential medicines is the aggressive negotiation tactics which the government has upheld towards MNCs with regards to the prices of their patented pharmaceuticals. For example, Brazil has often threatened to break patents and make some kinds of ARV drugs or import cheaper versions of them from other countries, as this pressurises the MNCs to lower their prices. A recent example of this took place in December 2004, when the head of the AIDS programme announced that Brazil intended to break patents on five anti-HIV/AIDS drugs this year; this initiated Merck & co. to make plans to allow Brazil to make their patented
AIDS drug ‘Stocrim’
74
. This illustrates that providing the artificial barriers of compulsory licensing are not an issue, it can be used as a tool for ‘patent busting’ so that generic drugs can be manufactured in this way. Pedro Chequer 75 stated clearly that any local production would comply with domestic and international laws i.e
. the
TRIPS agreement but also announced that ‘any law, be it national or international,
70 ‘Look at Brazil’
– www.nytimes.com/library/magazine/home/20010128mag-aids.htm
71 ‘ Look at Brazil’ – www.nytimes.com/library/magazine/home/20010128mag-aids.htm
72 See ‘The right fix?’ http://www.economist.com/agenda/displaystory.cfm?story_id=2020463 page 1
73 ‘Look at Brazil’ – www.nytimes.com/library/magazine/home/20010128mag-aids.htm
74 ‘Merck to allow Brazil to copy AIDS Drug Stocrim’ 2 nd December See http://www.bloomberg.com/apps/news?pid=10000086&sid=anv51yxhzdtk&refer=latin America
75 Coordinator for the Health Ministry’s sexually transmitted disease and AIDS Department.
Chloe Bunn 21 Intellectual Property Law that interferes with our ethnical interests, with the Brazilian governement’s commitment to universal access to patients, cannot be seriously considered
76 ’.
Despite aggressive complaints from MNCs, Brazil’s programme has
‘withstood the grumbles’
and stamped out any fallacies that the MNCs were prepared to suggest in relation to generic drugs 77 .
76 ‘Brazil to manufacture its own AIDS drugs’ 29 th November 2004 See Reuters Foundation http://www.alertnet.org/thenews/newsdesk/N29401620.htm
77
Refer to paragraph 2.4
‘Why have the MNCs lobbied against Generic drugs? Are there any drawbacks to generic drugs?’
Chloe Bunn 22 Intellectual Property Law
PART 5
5.1 Possible solutions/reform to assist generic production and therefore access to essential medicines for the future.
The current patent laws appear to infringe basic health rights and proposed reforms are needed to alleviate the grave problems which the world’s poor faces in relation to obtaining affordable generic medicines.
1. One proposal put forward in an Oxfam report
78
would allow generic drug prices to prevail for greater access to life saving medicines. The proposal is that developing countries should be allowed the freedom to decide both the
‘duration and scope of pharmaceutical patents
79 ’
and whether or not to exempt certain pharmaceutical products from patenting. By taking anti-HIV/AIDS drugs out of the patent regime and therefore out of the competitive market, the price of the drugs available would be greatly lowered and in fact the prices would mirror those of the current generic ARV prices. The reasons for this are that a) the monopoly that the MNCs enjoy over these life-saving drugs will be taken away, and b) poorer countries would no longer have to rely on the politically complicated ‘safeguard’ of compulsory licensing to produce or import generic drugs and this would mean that licensing fees would not have to be paid to a patent holder. It might be questioned who would manufacture these drugs; in an ideal world there should be private drug companies that were both efficient and behaved in a socially dependable way, however it seems that a sensible solution to keep the prices at a low cost would be ‘non-profit’ organisations ideally set up and funded by the government which would respond to the anti-HIV/AIDS drug demands of the specific developing countries.
2. There is a definite need for more generic drug production within developing countries themselves; this too would then be able to meet the market demand of the developing country it is set up to manufacture for. The approach that Brazil has taken has shown that this can be done if the government are willing to take a risk to solve their pandemic. The Governments in sub-Saharan Africa should stand up for their rights and compulsory licenses should be sought; bullying from the MNCs should be
78 See Oxfam’s recommendations in the article ‘The threat to public health’ May 2001 www.oxfam.org.uk/what_we_do/issues/health/drugcomp_Brazil.htm
79 www.oxfam.org.uk/what_we_do/issues/health/drugcomp_Brazil.htm
Chloe Bunn 23 Intellectual Property Law halted. If it is deemed too difficult to establish suitable pharmaceutical sectors in the majority of least developed countries, then following Brazil’s approach, it would appear that exerting pressure on the MNCs to lower their prices by threatening to produce or import generic versions of their drugs, would be a step in the right direction.
3. With regards to the legislative barriers and in particular TRIPS, it is suggested that what is needed in relation to generic drug availability is a more patient -friendly interpretation of the compulsory licensing provision in order to maximise the safeguard, and a reasonable interpretation of TRIPS in general. William Haddad suggests that
‘poor nations in need should have the right to produce or import medicines using a compulsory license and paying a fee approximating five percent to the innovator.
80 ’
This would serve to balance as best as it can the interests of both the patent holder and the poorer nations.
4. A fourth suggestion to increase access to cheaper generic drugs is that a greater number of voluntary licenses should be issued by the MNCs; the argument that this will lead to a loss in market share and will seriously threaten their research and development expenditure can be countered by statistical evidence which shows that the developing countries only account for a tiny proportion, less than 10%, of the entire pharmaceutical market
81
.
5.2 Conclusion
The current patent regime hinders the access to life-saving drugs by allowing them to be monopolised by MNCs making them unaffordable to the poorer countries of the world. The sensible solution up until now has been to allow the production of low cost generic drugs, in countries such as India, which offer an affordable alternative to expensive patented pharmaceuticals and therefore greatly assist in curtailing the deaths of millions in poorer nations. The threat that generic drugs pose to the MNCs has resulted in the price of brand named pharmaceuticals being lowered. However as this dissertation has illustrated, the current intellectual property regime has again
80 Generic Medicines: The Solution or the Problem?’ William Haddad page 25
81 Statistics from a 2003 report accessed at: http://www.yale.edu/yjhple/thoen.pdf
Chloe Bunn 24 Intellectual Property Law stepped in with the implementation of the TRIPS agreement and created another barrier denying millions the access to generic drugs. These artificial barriers must be amended as it appears that although ‘we have the medicines to convert a death sentence into a chronic illness…we are not using them 82 ’.
It is suggested that although the compulsory licensing provision and the DOHA Declaration go some way in providing a safeguard, their application is not without major practical and political barriers which often prevent their use. It is recognised that the balance which has to be struck between providing affordable medicines to the poor whilst protecting innovation can be a delicate one, but in light of the TRIPS agreement and how this affects the generic industry it appears that this balance has become tilted towards innovation and overlooks the interests of the suffering in the developing nations. It is clear that the solutions and reform as suggested above are greatly needed to ensure public health takes precedence over patent rights and generic drug production is facilitated not impeded. It should be noted that in attempting to increase the access to generic drugs this will almost certainly result in the MNCs teamed with the powers of western governments, using their lobbying powers to prevent this greater access
83
; this should be not be allowed at any cost because ‘if those in need are to continue to live, diseases are to be prevented and scientific advances are to be promoted and encouraged
84 ’; this includes promoting production of generic drugs.
‘The trauma of knowing life-saving drugs are readily available but unaffordable is deeply embedded in the hidden anger of the powerless.
85 ’
82 Quote from President William Clinton, see ‘Generic Medicines: The Solution or the Problem?’
William Haddad page 2
83 Refer to paragraph 2.4 ‘Why have the MNCs lobbied against Generic drugs? Are there any drawbacks to generic drugs?’
84 ‘Generic Medicines: The Solution or the Problem?’ William Haddad page 4
85 ‘Generic Medicines: The Solution or the Problem?’ William Haddad page 13
Chloe Bunn 25 Intellectual Property Law
BIBLIOGRAPHY
6.1 Cited Articles/Papers
‘India’s Choice’ The New York Times Editorial January 18 th 2005
‘Raking it in – How much is too much?’
The Guardian Friday February 4 th
2005
6.2 Cited Articles from websites:
‘Global report on the HIV/AIDS epidemic’.
UNAIDS
2004 http://www.unaids.org/html/pub/publications/fact-sheets04/FS_SSAfrica_en_pdf/FS
‘The AIDS pandemic in the 21 st
Century
’, Stanecki K. A.
(2002) Draft Report, July 2002, XIV
International Conference on AIDS, Barcelona, US Census Bureau. http://www.avert.org/aidsimpact.htm
‘Providing drug treatment for millions’ http://www.avert.org/drugtreatment.htm
‘The impact on life expectancy’
- http://www.avert.org/aidsimpact.htm
AIDS ‘Profits over people’ Walden Bello, Frontline – India’s National Magazine July
31 – August 13 th
2004 http://www.frontlineonnet.com/fl2116/stories/20040813003210400.htm
‘Access to Antiretroviral therapy in Uganda’
Oxfam Report, Kampala 2002 http://www.oxfam.org.uk/what_we_do/issues/hivaids/downloads/arvaccessuganda.pdf
‘Generic Medicines – The Solution or the problem’
by William (Bill) Haddad
October 21 st
2004 http://www.cptech.org/ip/health/generic/haddad10212004.doc
‘Bristol Myers Squibb offers to sell AIDS drugs in Africa at below cost’ The Wall
Street Journal March 15 th
2001 http://www.aegis.com/news/wsj/2001/WJ010312.html
‘How increased competition from generic drugs has affected prices and returns in the pharmaceutical industry’
June E. O'Neill Director Congressional Budget Office article July 1998 http://www.cbo.gov/showdoc.cfm?index=655&sequence=0&from=1
Chloe Bunn 26 Intellectual Property Law
‘Effort to make the Government Provide Nevirapine to pregnant HIV+ women to prevent mother to child transmission of HIV’ cp tech – Treatment Action Campaign
14 th December 2001 http://www.cptech.org/ip/health/sa/mtct.html
‘Generic competition, price and access to medicines’ Oxfam Briefing Paper
2002 report. http://www.oxfam.org.uk/what_we_do/issues/health/bp26_generic.htm
‘Importation of generics cuts price in half’
, Oxfam Press release
29 th
January 2002 http://www.oxfam.org.uk/press/releases/tac.htm
‘Glaxo grants Cipla AIDS-Drug Licence’
December 15 th
2004 http://allafrica.com/stories/200412150122.html
Brazil to break AIDS drug patents’
BBC News article
1 st
December 2004 http://news.bbc.co.uk/2/hi/health/4059147
‘Seeds of hope’
Pfizer
Annual report 2002. http://www.pfizer.com/are/investors_reports/annual_2002/p2002ar18_19_20_21.htm
‘Implications of the DOHA Declaration on the TRIPS agreement and Public Health’
World Health Organisation report
June 2002 http://www.who.int/medicines/library/ par/who-edm-par-2002-3/dohaimplications.doc
‘Undermining Access to medicines’
Oxfam Briefing note
June 2004 http://www.oxfam.org.uk/what_we_do/issues/health/undermining_access_ftas.htm
‘
US bullying On Drug Patents: One Year after DOHA’, Oxfam Briefing Paper no. 33 http://www.oxfam.org.uk/policy/papers/24global fund.html
‘Treat AIDS now – Blocking Access’ http://www.peopleandplanet.org/stopaids/briefing.access.php
‘Global Day of Action against Indian Patent Ordinance 26 th
February 2005’ Ip
Health Archives Lawyers
Friday 11 th
February http://lists.essential.org/pipermail/ip-health/2005-February/007465.html
‘New patent law to shake up drug industry’ Ip Health Archives Ram
Thursday 30 th
December http://lists.essential.org/pipermail/ip-health/2004
Chloe Bunn 27 Intellectual Property Law
‘Indian Trips Legislation under fire’
Ip health Mike Palmedo Bridges Weekly Trade
News Digest January 19, 2004. Vol 9, no. 1 http://lists.essential.org/pipeline/ip-health/2005-January/007368.html
‘New Indian Patent Law pushes up prices of anti-AIDS drugs’ http://lists.essential.org/pipermail/ip-health/2005-February/007464.html
‘Look at Brazil’ Tina Rosenberg, New York Times
28 th
January 2001 http://www.nytimes.com/library/magazine/home/20010128mag-aids.html
‘The right fix?’ from the Economist Global Agenda
1 st
September 2003 http://www.economist.com/agenda/displaystory.cfm?story_id=2020463
‘Merck to allow Brazil to copy AIDS Drug Stocrim’ Valor
Ip Health 2 nd
December http://www.bloomberg.com/apps/news?pid=10000086&sid=anv51yxhzdtk&refer=lati n America
‘Brazil to manufacture its own AIDS drugs’ Reuters Foundation
29 th
November 2004 http://www.alertnet.org/thenews/newsdesk/N29401620.htm
‘The threat to public health’
Oxfam’s recommendations
May 2001 report http://www.oxfam.org.uk/what_we_do/issues/health/drugcomp_Brazil.htm
6.3
Other Cited Websites/Electronic Sources: http://www.avert.org/generic.htm http:/www.avert.org/subaadults.htm http://www.cptech.org/ip/health/cl/faq.html http://www.fda.gov/cder/ogd/#Introduction http://lists.essential.org/pipermail/ip-health/2005-January /007394.html http://lists.essential.org/pipermail/ip-health/2005-March/007625.html http://www.nytimes.com/library/magazine/home/20010128mag-aids.htm http://www.unaids.org/bangkok2004/factsheets.html http://www.yale.edu/yjhple/thoen.pdf http://yaleglobal.yale.edu/display.article?id=4808
Chloe Bunn 28 Intellectual Property Law
6.4 Background Reading
Books:
Blackstone’s Statutes on Intellectual Property
7 th Edition
Andrew Christie & Stephen Gare
Pages 561-572
Intellectual Property Rights in the WTO and Developing Countries
Kluwer Academic Publishers 2001 Edited by Jayashree Watel
Pages 86 – 128
Journals:
Intellectual Property Quarterly
Issue 2 (2004)
Thompson – Sweet & Maxwell Editor: Dr. Margaret Llewelyn
Article:
‘Use of pharmaceutical Patents without Authorisation: Some thoughts from
South Africa’ Andries van der Merwe
Intellectual Property Quarterly
Volume 4 (2000)
London – Sweet & Maxwell 2000 Editor: Professor John N. Adams
Article:
‘Analysis: Affordable Medicines – TRIPS and the United States Policies’
Electronic sources: http://www.news24.com/News24/Africa/Features/0,6119,2-11-37_1453168,00.html
Article: ‘Africa wants generic AIDS drugs’ 01/12/2003 http://www.oxfam.org.uk/what_we_do/issues/health/drugcomp_Brazil.htm
Article: ‘Drug Companies Vs Brazil: The Threat to Public Health’ http://www.globaltreatmentaccess.org/content/press_releases/01/111401_WTO_TRIP
S_Decl.html
‘Declaration on the TRIPS Agreement and Public Health’
Ministerial Conference
Fourth Session
Doha, 9-14 November 2001