case history
advertisement

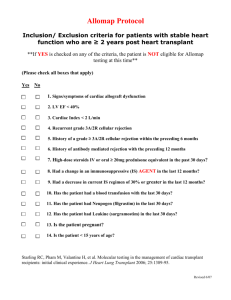
School of Health Professions, Department of Physical Therapy PT 7890, Case Management I A Heart Transplant Case Part I Mr. B. is a retired pharmacist who experienced a fairly rapid onset of decreasing cardiac function with signs and symptoms of congestive heart failure. In a period of less than three years, he was increasingly troubled by fatigue and episodes of faintness and rapid heartbeat. At one point, he apparently had a near death episode. He ultimately received a heart transplant that has restored him to a vigorous life, although he must take anti-rejection drugs and undergo various tests for the rest of his life. The chronology of his cardiac history follows. September, 1997: following complaints of increasing fatigue and shortness of breath with exertion, patient was initially diagnosed with idiopathic cardiomyopathy. Cardiac catheterization revealed narrowing of coronary arteries consistent with age, but there was nothing to suggest patient at high risk for coronary artery occlusion. Social History: DOB Oct. 6,1931 Married, his wife is a nurse; 5 children Owned and operated pharmacy for many years Parents deceased: father pancreatic cancer at age 88; mother CHF at age 93 Home: one story ranch with two steps to front door Hobbies include extensive travel. March, 1998: Patient experienced an acute onset of pronounced fatigue and shortness of breath during a driving trip in the Colorado mountains. He lost consciousness and apparently experienced a near-death episode. His ventricular fibrillation was cardioverted to normal sinus rhythm in an emergency room. He subsequently received an implanted automatic cardiac defibrillator, a pacemaker that controlled atrial and ventricular fibrillation. Dobutamide, 5 ug/kg/min qid, for one day only, was prescribed (DeTurk p.212). July, 1998: Experienced acute CHF while traveling in North Carolina; "I almost didn't make it home." Amiodarone (DeTurk p.210-211) was prescribed. November, 1998: A physician's note documenting patient progress noted that "he reported being able to carry shingles up to the roof of his house on a ladder." March , 1999: Patient reported that he had "passed out while driving". He also reported that a self prescribed trial period of going without Lasix had caused a significant increase in dyspnea. October, 1999: Symptoms of CHF were increasing with greater fatigue and SOB even on level ground. Arm and hand tremors and ease of bruising were observed. Poor appetite and weight loss were also noted. TSH levels were to be measured. Hypothyroidism, probably secondary to amionardone, was identified. February, 2000: Aortic regurgitation was identified during echocardiogram. Zebeta (DeTurk p.191-2) was prescribed. The patient queried the physician, asking: "Do you think it would be all right for my wife and me to travel to New Zealand by freighter?" Part 2 Page 1 of 3 June, 2000: The possibility that he might be a candidate for a heart transplant was raised. He had no significant, major contraindications to transplant surgery, although his age was viewed by some as problematic. Many tests were scheduled, including those to rule out infection, liver and kidney function, cancer risk, psychological preparedness, and family support. June 12, 2000: Medical History: No HTN, DM, or pulmonary symptoms Denies ever smoking; has not used alcohol for many years Hypothyroidism (probably secondary to amiodarone) Cataract surgery with prosthetic implants bilaterally TURP Hernia repair X 3 Skin cancers removed from face in 1994 (SCC), and 1998 (BCC) Gastric ulcers (recent onset) Sedentary lifestyle. Review of systems: Height: 6'3" Weight 180 (has lost more than 25# in past year) Eyes: mild icterus ENT: NL Cardiovascular: SI, S2, S3 SSM 1 /v 1 @ apex (from patient’s ECG results) Lungs: Bilat CTA GI: abd soft, NT, liver palpable, firm edge Neuro: grossly intact Endocrine: 0 Gastric ulcers (recent onset) July 12, 2000: Echocardiogram assessed cardiac ejection fraction as very low, having fallen from 39% to 20% to the current IO% over a two-year period. His medical diagnosis was idiopathic dilated cardiomyopathy and congestive hepatomegaly causing indirect hyperbilirubinemia, with mildly elevated BUN and creatinine. His medications included: Carafete 1 gm qid Lasix up to 10 mg qd p.189-91 Prevacid 30 mg qd Procainamid 750 mg bid p.210 Lanoxin .125 mg qd p.211-12 Enalapril 20 mg bid p.192-3 MgO 400 mg qd ASA 5gms Synthroid .125 qd As part of the preoperative program, cardiac rehabilitation program was initiated at 13:00. Resting vital signs: HR: 106 IRIR, RR: 26, BP 116/88. At 13:30, the patient c/o feeling flushed and having a rapid heartbeat. Resp. rate was 40. Patient was unresponsive for several moments during which his pulse was documented at 132 bpm, IRIR and "strong", BP was 72/44. Afterwards, the patient was documented as saying "this happens to me fairly frequently at home." Telemetry ECG showed PVCs with retrograde p and accelerated ventricular pacing. Part 3 Page 2 of 3 Between July 17 and 24, 2000, the pre-transplant medical workup was completed. Hematologic: Patient was Blood Group AB + Chemistry: 143 4.4 110 26 25 1.6 116 10.8 4.8 July 24, 2000: Mr. B was added to the heart transplant list. July 25, 2000: A donor heart matching Mr. B's immunological profile became available, and the heart transplant was carried out. The native heart described as extremely enlarged, with greatly dilated right and left ventricles, and dilated atria. The donor heart was a great deal smaller. Modifications of the standard implant procedure were used to secure the donor heart to the great vessels. August 8, 2000: Phase II OP Cardiac rehabilitation was initiated. October, 2000: Supervised cardiac rehabilitation was discontinued. A cardiac biopsy showed no evidence of rejection. Mr. B joined a health club in the community to continue with his rehabilitation. June, 2001: Repeat cardiac biopsy, no evidence of rejection. Page 3 of 3